Explain portal hypertension, pathophysiology and causes of portal hypertension , investigation , clinical featurea and management of portal htn .
Reading File
Finding Sources
Finding Sources
Searching PubMed
"portal hypertension" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed to compile a comprehensive, well-structured answer. Let me write it up.
Portal Hypertension - Complete Clinical Overview
1. Definition
Portal hypertension is defined as an abnormal increase in pressure within the portal venous system. In clinical practice, it is measured indirectly by the Hepatic Venous Pressure Gradient (HVPG):
HVPG = Wedged Hepatic Venous Pressure (WHVP) - Free Hepatic Venous Pressure (FHVP)
| HVPG Value | Significance |
|---|---|
| < 5 mmHg | Normal |
| 5-9 mmHg | Portal hypertension (subclinical) |
| ≥ 10 mmHg | Clinically significant portal hypertension |
| ≥ 12 mmHg | Threshold for variceal development and ascites |
| > 20 mmHg | High risk of rebleeding and mortality |
- Current Surgical Therapy 14e, p.455; Sleisenger and Fordtran's GI & Liver Disease
2. Pathophysiology
The pathophysiology of portal hypertension is governed by Ohm's law applied to the portal circulation:
Portal Pressure = Portal Blood Flow × Intrahepatic Resistance
Both components are elevated in portal hypertension, creating a two-hit mechanism:
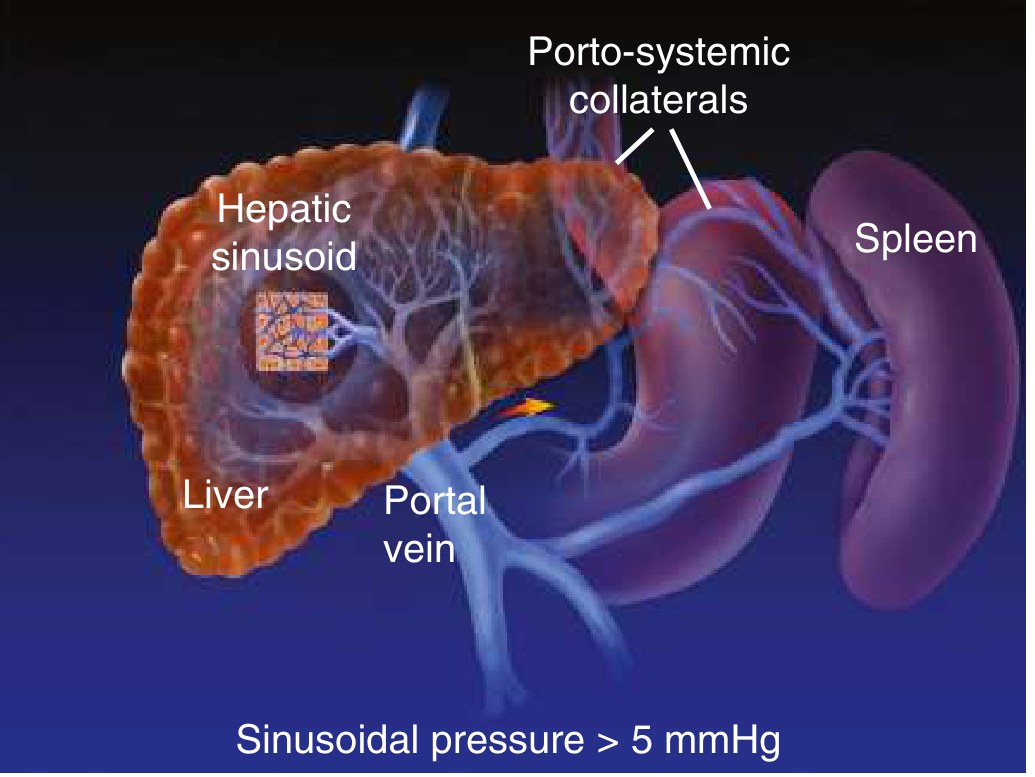
Portal hypertension in cirrhosis: sinusoidal pressure > 5 mmHg, splenomegaly, portosystemic collaterals form - Goldman-Cecil Medicine, Fig. 13-3
A. Increased Intrahepatic Resistance (Mechanical + Functional)
Mechanical component:
- Progressive collagen deposition and regenerative nodules distort sinusoidal architecture
- Scarring compresses sinusoids and disrupts normal blood flow
Functional (dynamic) component (accounts for ~30% of resistance):
- Contraction of vascular smooth muscle cells, myofibroblasts, and hepatic stellate cells
- Decreased nitric oxide (NO) production by sinusoidal endothelial cells → intrahepatic vasoconstriction
- Increased release of endothelin-1, angiotensinogen, and eicosanoids → further vasoconstriction
- Sinusoidal remodeling with arterio-portal anastomoses in fibrous septa imposes arterial pressures on the low-pressure portal venous system
B. Increased Portal Blood Flow (Hyperdynamic Circulation)
- Splanchnic arterial vasodilation is the key driver - primarily mediated by overproduction of NO in the extrahepatic circulation (a paradox vs. the intrahepatic NO deficiency)
- Other mediators: prostacyclin, TNF-alpha, glucagon
- Splanchnic vasodilation → increased splanchnic venous return → increased portal inflow
- This drives a hyperdynamic circulatory state: increased cardiac output, increased total blood volume, decreased systemic vascular resistance
- Activation of renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system (SNS) → sodium and water retention → further plasma volume expansion
The paradox of portal hypertension:
-
Intrahepatic: NO deficiency → vasoconstriction → increased resistance
-
Extrahepatic (splanchnic): NO excess → vasodilation → increased flow
-
Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine
3. Causes of Portal Hypertension
Portal hypertension is classified anatomically into three types:
Prehepatic (Pre-sinusoidal, Extrahepatic)
- Portal vein thrombosis (most common prehepatic cause)
- Splenic vein thrombosis
- Congenital narrowing/stenosis of portal vein
- Splenomegaly with increased splenic blood flow (e.g., myelofibrosis, tropical splenomegaly)
- Arteriovenous fistula (splenic)
Intrahepatic
Pre-sinusoidal:
- Schistosomiasis (most common worldwide cause overall)
- Primary biliary cholangitis (even without cirrhosis)
- Congenital hepatic fibrosis
- Nodular regenerative hyperplasia
- Sarcoidosis / diffuse fibrosing granulomatous disease
- Infiltrative malignancy (primary or metastatic)
Sinusoidal (most common in Western countries):
- Cirrhosis - by far the leading cause (alcohol, viral hepatitis B/C, NAFLD/NASH, autoimmune)
- Massive fatty change
- Amyloidosis
Post-sinusoidal (intrahepatic):
- Veno-occlusive disease (hepatic sinusoidal obstruction syndrome)
- Focal malignancy with portal vein invasion (especially HCC)
Posthepatic (Post-sinusoidal, Extrahepatic)
- Budd-Chiari syndrome (hepatic vein thrombosis)
- Severe right-sided heart failure
- Constrictive pericarditis
- Inferior vena cava obstruction/web
Key epidemiological point: In North America/Europe, cirrhosis accounts for ~90% of cases. Worldwide, schistosomiasis and portal vein thrombosis are far more common.
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Current Surgical Therapy 14e
4. Clinical Features
Symptoms
- Abdominal distension (ascites)
- Hematemesis or melena (variceal bleeding)
- Altered consciousness, confusion (hepatic encephalopathy)
- Fatigue, malaise
- Symptoms of the underlying liver disease
Signs
Consequences of portal hypertension directly:
| Feature | Mechanism |
|---|---|
| Splenomegaly | Congestive; often with hypersplenism (thrombocytopenia, leukopenia, anemia) |
| Ascites | Sinusoidal hypertension + hypoalbuminemia + splanchnic vasodilation + sodium retention (HVPG ≥ 12 mmHg required) |
| Esophageal varices | Portosystemic collaterals via coronary/gastric veins; develop at HVPG ≥ 10-12 mmHg |
| Gastric varices | Fundal (IGV1) or elsewhere (IGV2); higher risk of fatal bleeding |
| Caput medusae | Dilated periumbilical veins via recanalized umbilical vein (paraumbilical collaterals) |
| Portal hypertensive gastropathy | Dilated mucosal/submucosal venous plexus; "snakeskin" appearance on endoscopy |
| Anorectal varices | Rectal portosystemic collaterals |
Signs of underlying liver disease:
- Jaundice, spider angiomas, palmar erythema
- Gynecomastia, testicular atrophy (hyperestrogenism)
- Leukonychia, Dupuytren's contracture
- Hepatomegaly or small liver (late cirrhosis)
Complications:
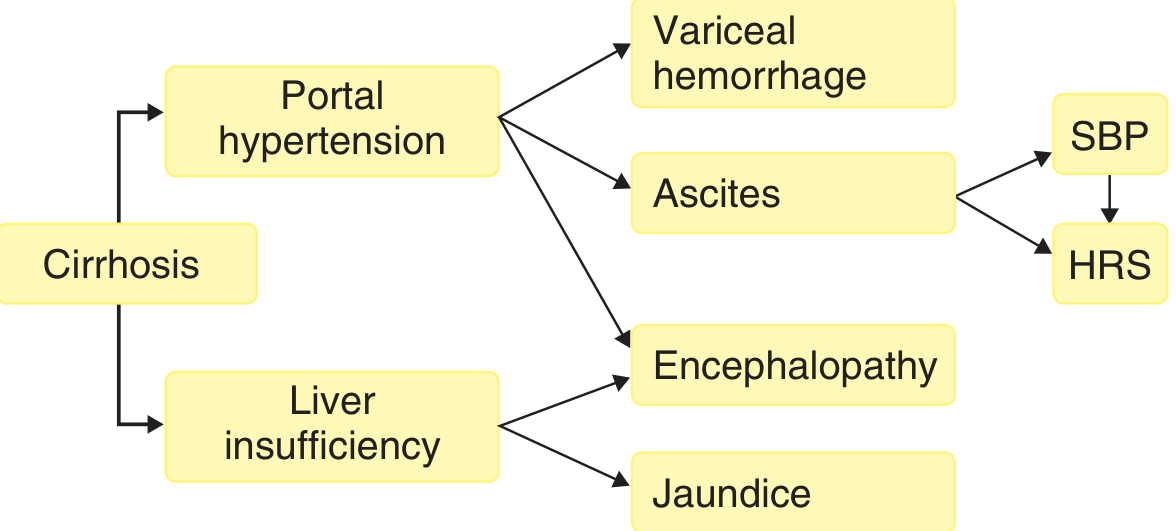
Complications of cirrhosis - varices and ascites from portal hypertension; encephalopathy and jaundice from liver insufficiency - Goldman-Cecil Medicine, Fig. 139-2
- Variceal hemorrhage - most immediately life-threatening; mortality ranges 5-68% depending on Child-Pugh class
- Ascites - occurs in 85% of cases from cirrhosis; may lead to SBP or hepatorenal syndrome
- Hepatic encephalopathy - due to portosystemic shunting (ammonia bypass) and liver insufficiency
- Spontaneous bacterial peritonitis (SBP) - bacterial translocation from gut into ascitic fluid
- Hepatorenal syndrome (HRS) - extreme peripheral vasodilation → renal vasoconstriction
- Hepatopulmonary syndrome / portopulmonary hypertension
- Goldman-Cecil Medicine; Robbins, Cotran & Kumar; Current Surgical Therapy 14e
5. Investigations
Laboratory Tests
| Test | Finding |
|---|---|
| CBC | Thrombocytopenia, leukopenia, anemia (hypersplenism) |
| LFTs | Raised bilirubin, AST, ALT, ALP (underlying liver disease) |
| Serum albumin | Low (synthetic dysfunction) |
| PT/INR | Prolonged (coagulopathy) |
| Serum sodium | Low (dilutional hyponatremia in advanced disease) |
| Serum creatinine/urea | Raised in hepatorenal syndrome |
| Urine sodium | Low (<10 mEq/day in sodium retention) |
Scoring Systems for Severity
- Child-Turcotte-Pugh (CTP) score - based on ascites, encephalopathy, bilirubin, albumin, PT; classifies A (5-6), B (7-9), C (10-15)
- MELD score = [0.957 × LN(creatinine) + 0.378 × LN(bilirubin) + 1.12 × LN(INR) + 0.643] × 10; used for transplant listing
- MELD-Na - incorporates serum sodium for improved mortality prediction
Imaging
Ultrasound (first-line):
- Portal vein diameter > 13 mm (dilated)
- Splenomegaly (>12 cm)
- Ascites
- Reversed/sluggish portal flow on Doppler
- Detection of collaterals (e.g., recanalized umbilical vein)
Doppler Ultrasound:
- Measures portal venous flow velocity and direction
- Hepatofugal flow (reversed) confirms portal hypertension
CT Abdomen with contrast:
- Identifies varices, splenomegaly, ascites, caudate lobe hypertrophy
- Detects portal vein thrombosis, Budd-Chiari, HCC
- Demonstrates portosystemic collaterals
MRI / MR Angiography:
- Better delineation of hepatic/portal venous anatomy
- Useful for Budd-Chiari syndrome
Direct Pressure Measurement - Gold Standard
Hepatic Venous Pressure Gradient (HVPG):
- Transjugular catheterization of hepatic vein
- WHVP - FHVP = HVPG (reflects sinusoidal pressure)
- HVPG ≥ 10 mmHg = clinically significant portal hypertension
- HVPG ≥ 12 mmHg = risk of variceal bleeding and ascites
- HVPG > 20 mmHg = high risk of treatment failure
- Limitation: Only accurate for sinusoidal/postsinusoidal causes (not for prehepatic)
EUS-guided Portal Pressure Gradient (PPG):
- Newer technique; theoretically accurate for pre-sinusoidal, sinusoidal, and postsinusoidal causes
- PPG = PVP - HVP
Endoscopy
Upper GI endoscopy (EGD):
- Mandatory for all patients with suspected portal hypertension
- Diagnoses esophageal varices (grade I-IV), gastric varices (GOV1, GOV2, IGV1, IGV2)
- Portal hypertensive gastropathy - mosaic/snakeskin pattern with cherry-red spots
- Identifies active bleeding source
Liver Biopsy
- Determines etiology and stage of liver disease
- Gold standard for fibrosis staging (Metavir, Ishak scales)
- Not always needed if clinical picture is clear
Serum-Ascites Albumin Gradient (SAAG)
-
SAAG ≥ 1.1 g/dL = portal hypertension (97% accuracy)
-
SAAG < 1.1 g/dL = exudative cause (malignancy, TB, pancreatitis)
-
Frameworks for Internal Medicine; Current Surgical Therapy 14e; Sleisenger and Fordtran's GI & Liver Disease
6. Management
Management is directed at: (1) treating the underlying cause when reversible, (2) reducing portal pressure, (3) preventing and treating complications, and (4) liver transplantation when indicated.
A. Medical Management
Non-selective Beta-blockers (NSBBs):
- Propranolol (20-80 mg BD) or Nadolol (40-240 mg OD) or Carvedilol (6.25-12.5 mg OD)
- Reduce portal pressure by: β1 blockade (reduces cardiac output) + β2 blockade (splanchnic vasoconstriction)
- Target: reduce HVPG by ≥ 20% from baseline, or to < 12 mmHg
- Used for: primary prophylaxis of first variceal bleed and secondary prophylaxis after banding
Vasoactive drugs (acute variceal bleeding):
- Terlipressin (first-line): splanchnic vasoconstrictor; reduces portal pressure
- Octreotide / Somatostatin: inhibit vasodilatory hormones (glucagon) → splanchnic vasoconstriction
- Start immediately on suspicion of variceal bleed, before endoscopy, continue for 3-5 days
Antibiotics (acute variceal bleed):
- Short-course prophylactic antibiotics (e.g., ceftriaxone 1g IV OD x 7 days) reduce SBP risk and improve survival
Diuretics (ascites):
- Spironolactone (aldosterone antagonist, 100-400 mg/day) + Furosemide (40-160 mg/day) - combination preferred
- Target weight loss: 0.5 kg/day (without peripheral oedema), 1 kg/day (with peripheral oedema)
- Refractory ascites: large-volume paracentesis (LVP) + albumin infusion (8 g per litre removed)
Lactulose / Rifaximin (hepatic encephalopathy):
- Lactulose reduces gut ammonia absorption
- Rifaximin (non-absorbable antibiotic) reduces secondary prevention of hepatic encephalopathy
B. Endoscopic Management
Endoscopic Variceal Ligation (EVL) - Band Ligation:
- Preferred over sclerotherapy for esophageal varices
- Primary prophylaxis: for large varices or varices with red signs in Child B/C patients who cannot tolerate NSBBs
- Acute bleeding: combined with vasoactive drugs (emergency EGD within 12 hours)
- Secondary prophylaxis: EVL every 1-2 weeks until eradication; then surveillance EGD every 3-6 months
- Superior to sclerotherapy: faster eradication, less rebleeding, fewer complications
Endoscopic Sclerotherapy (EST):
- Injection of sclerosant (ethanolamine, polidocanol) into varices
- Now second-line to EVL; still used for gastric varices
- Risk of esophageal ulceration, stricture
Endoscopic cyanoacrylate glue injection:
- Preferred for gastric varices (GOV2, IGV1) where EVL is less effective
Balloon Tamponade (temporary bridging only):
- Sengstaken-Blakemore tube, Minnesota tube, Linton-Nachlas tube
- Controls bleeding in ~80% but temporary (max 24 hours); high complication rate (aspiration, esophageal perforation, necrosis)
- Only used as bridge when definitive treatment unavailable
C. Radiological Interventions
TIPS (Transjugular Intrahepatic Portosystemic Shunt):
- Creates a shunt between hepatic vein and portal vein through hepatic parenchyma using expandable metallic stent
- Reduces portal pressure by bypassing hepatic resistance
- Indications: refractory variceal bleeding, refractory ascites, Budd-Chiari syndrome, hepatorenal syndrome, bridge to transplant
- Contraindications: hepatic encephalopathy (relative), severe right heart failure, polycystic liver disease
- Complication: hepatic encephalopathy (30-50%)
- Has largely replaced surgical shunts in current practice
D. Surgical Management
Surgical Portosystemic Shunts:
Reserved for when TIPS is unavailable, not feasible, or fails, and in extrahepatic portal hypertension with intact liver function.
| Shunt Type | Description | Comments |
|---|---|---|
| Non-selective (total) shunts | End-to-side or side-to-side portacaval shunt; diverts all portal flow to systemic | Very effective; high encephalopathy rate |
| Selective distal splenorenal shunt (Warren shunt) | Decompresses varices via splenic vein to left renal vein; preserves hepatopetal flow | Less encephalopathy; preferred when feasible |
| Rex shunt (meso-left portal bypass) | Jugular vein graft from SMV to intrahepatic left portal vein | For children with extrahepatic portal vein thrombosis; restores hepatopetal flow |
- Both non-selective and selective shunts achieve >90% hemorrhage control with similar rebleeding rates and survival; encephalopathy is significantly lower with distal splenorenal shunt.
Devascularization Procedures:
- Sugiura procedure: ligation of gastroesophageal collaterals + esophageal transection + splenectomy
- Now rarely performed; high morbidity/mortality (up to 35%)
Liver Transplantation:
- Gold standard and only cure for portal hypertension due to cirrhosis
- Treats both the underlying liver disease and all complications of portal hypertension
- MELD score guides prioritization
- Indicated when MELD ≥ 15, recurrent variceal bleeding despite optimal therapy, refractory ascites, hepatorenal syndrome, or SBP
- Not appropriate for non-cirrhotic etiologies with intact liver function
E. Management of Specific Complications
| Complication | Management |
|---|---|
| Acute variceal bleed | Resuscitation + vasoactive drugs (terlipressin) + antibiotics + urgent EGD (EVL) within 12 hours; TIPS if fails |
| Primary prophylaxis | NSBB (propranolol/nadolol/carvedilol) OR EVL for large varices |
| Secondary prophylaxis | NSBBs + EVL combined |
| Ascites | Sodium restriction (< 2g/day) + diuretics (spironolactone + furosemide); LVP + albumin for refractory |
| SBP | IV ceftriaxone or cefotaxime + IV albumin (1.5 g/kg day 1, 1 g/kg day 3) to prevent HRS |
| Hepatic encephalopathy | Treat precipitant + lactulose + rifaximin; dietary protein restriction no longer recommended |
| Hepatorenal syndrome | Terlipressin + albumin; TIPS as bridge; liver transplant definitive |
- Current Surgical Therapy 14e; Goldman-Cecil Medicine; Sleisenger and Fordtran's GI & Liver Disease; Robbins, Cotran & Kumar Pathologic Basis of Disease; Maingot's Abdominal Operations
Recent Evidence (2024-2026)
Recent systematic reviews have updated specific areas:
- A 2025 meta-analysis on non-cirrhotic portal hypertension (PMID 40081810) examined hepatic encephalopathy prevalence, finding it relevant even in non-cirrhotic cases.
- A 2024 systematic review on ectopic variceal bleeding (PMID 38935315) confirmed TIPS as effective management for ectopic varices.
- A 2025 systematic review on portal cavernoma cholangiopathy (PMID 41085547) updated understanding of biliary complications in extrahepatic portal hypertension.
Summary: Portal hypertension results from increased intrahepatic resistance (cirrhosis being the dominant cause) compounded by splanchnic vasodilation-driven hyperdynamic circulation. The HVPG is the gold standard measurement. Key clinical consequences are varices (HVPG ≥ 12 mmHg), ascites, and hepatic encephalopathy. Management follows a stepwise approach: medical (NSBBs, vasoactive drugs), endoscopic (EVL), interventional (TIPS), surgical (shunts), and ultimately liver transplantation.
This is a shared conversation. Sign in to Orris to start your own chat.