Phosphorous use in icu
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypophosphatemia ICU management
Finding Sources
Finding Sources
Searching PubMed
phosphate replacement critically ill patients
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to provide a thorough answer. Let me compile it.
Phosphorus in the ICU
Phosphorus (as inorganic phosphate, Pi) is the most abundant intracellular anion and plays a central role in energy metabolism (ATP), 2,3-DPG synthesis, cell signaling, and bone mineralization. Serum concentration normally ranges from 2.5 to 4.5 mg/dL. Both hypo- and hyperphosphatemia are clinically significant in ICU patients.
1. Physiology Relevant to Critical Care
- 85-90% of body phosphorus is in bone as calcium phosphate (apatite); less than 1% is in the extracellular fluid
- Pi is essential for ATP production - depletion directly impairs every energy-dependent cellular process
- Red cell 2,3-DPG synthesis depends on adequate Pi: low Pi causes a left shift of the oxyhemoglobin dissociation curve, reducing O2 delivery to tissues
- Renal handling: freely filtered at the glomerulus, reabsorbed in the proximal tubule; regulated by FGF-23, PTH, and calcitriol
- Dietary phosphorus is abundant in protein (~15 mg phosphorus per gram of protein ingested)
2. Hypophosphatemia
Incidence in the ICU
- Present in 10-20% of critically ill patients (some series report up to 28-34% of ICU patients, and 65-80% of patients with sepsis)
- Strongly associated with in-hospital mortality, though causality is uncertain
Mechanisms (three main categories)
| Mechanism | ICU examples |
|---|---|
| Internal redistribution (most common) | Refeeding syndrome, DKA recovery, respiratory alkalosis, catecholamine surge, insulin/glucose administration |
| Increased renal losses | Metabolic acidosis (recovery), diuretic use, glucocorticoids, post-renal transplant, Fanconi syndrome |
| Decreased intestinal absorption | Phosphate-binding antacids (chronic use), vitamin D deficiency, chronic diarrhea, malnutrition |
In the ICU, internal redistribution dominates - alkalosis, insulin release with feeding, and catecholamines all drive phosphate into cells acutely. Major hepatic resection causes a specific pattern where phosphate is consumed for hepatocyte regeneration. Trauma and burns also cause hypophosphatemia through extracellular fluid shifts, alkalosis from lactated Ringer's resuscitation, and hypermetabolism.
Refeeding Syndrome - a Critical ICU Entity
Occurs when nutrition is reintroduced after starvation (>5 days), especially in prolonged malnutrition. Within 72 hours of refeeding:
- Insulin secretion rises with carbohydrate load
- Anabolic processes accelerate, demanding Pi for ATP synthesis
- Already-depleted serum phosphate shifts rapidly intracellularly
- Hallmark electrolyte abnormality: severe hypophosphatemia
- Concomitant hypokalemia, hypomagnesemia, and thiamine deficiency are common
- Clinical consequences: cardiac failure, respiratory muscle weakness, immune dysfunction, death if unrecognized
Management: slow refeeding, close electrolyte monitoring, aggressive IV electrolyte repletion, caloric restriction during initial phase.
Clinical Manifestations
| System | Manifestations |
|---|---|
| Respiratory | Diaphragm dysfunction, respiratory failure, difficulty weaning from ventilator |
| Cardiovascular | Congestive heart failure, arrhythmias, cardiovascular collapse (severe) |
| Neurologic | Paresthesias, delirium, encephalopathy, seizures, coma |
| Musculoskeletal | Proximal myopathy, rhabdomyolysis, bone pain |
| Hematologic | Hemolysis (increased RBC rigidity), platelet dysfunction, impaired PMN phagocytosis |
| Metabolic | Insulin resistance, impaired gluconeogenesis |
Key ICU implication: Hypophosphatemia causes diaphragm dysfunction and prolonged ventilator weaning - always check and correct phosphate before attempting liberation from mechanical ventilation.
Severe hypophosphatemia (Pi <1.0 mg/dL) can cause life-threatening organ failure. Moderate hypophosphatemia (1.0-2.5 mg/dL) is usually asymptomatic in terms of specific signs, though still metabolically significant.
Treatment
Severe hypophosphatemia (Pi <1.0 mg/dL) - IV repletion:
- Potassium phosphate or sodium phosphate IV
- Dose: 0.2-0.68 mmol/kg (5-16 mg/kg) over 12 hours
- For very severe cases: up to 45 mmol total, at a rate not exceeding 20 mmol/hr
- Choose KPhos vs NaPhos based on concurrent potassium level
- Rate must not exceed 1-3 mEq/hr in standard practice (risk of hypocalcemia from calcium phosphate precipitation; severe cases risk calciphylaxis)
- Monitor Pi, K+, and Ca2+ closely during and after repletion
Moderate hypophosphatemia:
- Oral repletion preferred, over 3-10 days depending on severity
- Up to triple the normal intake in divided doses
Patients with refeeding syndrome: require additional supplementation and more frequent electrolyte monitoring
3. Hyperphosphatemia
Incidence
- Affects 20-45% of ICU patients
- More common with ongoing critical illness; associated with increased all-cause mortality
Causes in the ICU
| Category | Examples |
|---|---|
| Reduced excretion | Acute kidney injury, CKD (most common cause overall) |
| Increased endogenous load | Rhabdomyolysis, tumor lysis syndrome, hemolysis, sepsis, trauma, cell lysis |
| Exogenous load | Phosphate-based laxatives/enemas, high-dose fosphenytoin, excess phosphate supplementation |
Hyperphosphatemia combined with concurrent hypocalcemia should always prompt evaluation for hypoparathyroidism (especially post-thyroidectomy). In the ICU, do not correct hypocalcemia before addressing the elevated phosphorus in acute hyperphosphatemia.
Clinical Consequences
- Symptoms are usually related to the underlying cause (e.g., renal failure)
- Acute severe hyperphosphatemia: hypotension, signs of hypocalcemia (tetany, seizures)
- Chronic: soft tissue calcification, vascular calcification, secondary hyperparathyroidism
Treatment
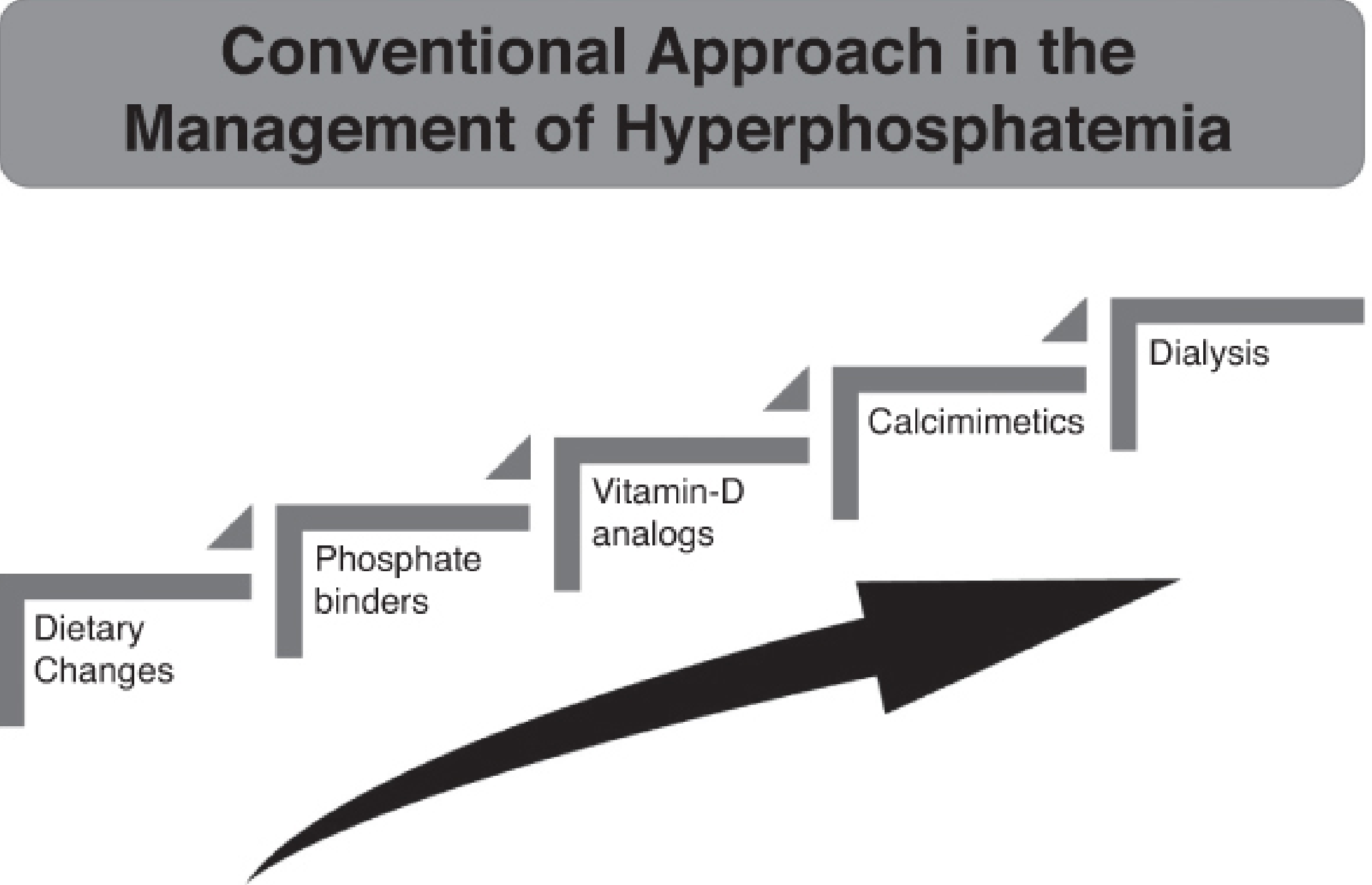
The approach is stepwise and depends on renal function:
- Dietary restriction of phosphate (first-line with intact renal function)
- Phosphate binders with meals:
- Calcium carbonate (also helps if hypocalcemia co-exists)
- Calcium acetate
- Sevelamer (non-calcium-based, preferred in CKD)
- Sucralfate or aluminum-containing antacids (historically used; risk of aluminum toxicity limits long-term use)
- Promote renal excretion: volume expansion, loop or thiazide diuretics, carbonic anhydrase inhibitors
- Vitamin D analogs - reduce PTH-driven bone resorption (in CKD/secondary hyperparathyroidism)
- Calcimimetics - further reduce PTH indirectly
- Dialysis - for severe symptomatic hyperphosphatemia, anuric renal disease, or refractory cases; hemodialysis or peritoneal dialysis
The "3 D's of hyperphosphatemia management: Diet, Drugs, and Dialysis."
With normal GFR, dietary restriction alone usually corrects hyperphosphatemia. With renal dysfunction, the stepwise approach above applies.
4. Special ICU Considerations
| Scenario | Phosphate consideration |
|---|---|
| Ventilator weaning failure | Always exclude hypophosphatemia (diaphragm dysfunction) |
| Post-major hepatic resection | Monitor for hypophosphatemia from regeneration-related phosphate consumption |
| Trauma/burns | High risk of hypophosphatemia; alkalosis from resuscitation worsens it |
| DKA treatment | Insulin shifts phosphate intracellularly; monitor closely |
| Refeeding after starvation | Refeeding syndrome risk; correct electrolytes before/during feeding |
| AKI on CRRT | Can develop either hypo- or hyperphosphatemia depending on dialysate composition; closely monitor |
| Rhabdomyolysis | Risk of hyperphosphatemia from intracellular release despite normal/elevated apparent serum levels |
| Sepsis | Very high incidence (65-80%) of hypophosphatemia |
Sources:
- Barash Clinical Anesthesia, 9e (Chapter 16, pp. 1243-1246)
- Brenner and Rector's The Kidney, 2-Volume Set (Chapter 18, pp. 822-824)
- Sabiston Textbook of Surgery (Chapter on fluid/electrolyte management, p. 607)
- Current Surgical Therapy, 14e (Refeeding Syndrome section)
This is a shared conversation. Sign in to Orris to start your own chat.