I now have everything needed. Here is the full explanation of PA 31.7 - Pancreatic Cancer:
PA 31.7 - Pancreatic Cancer
Etiology, Pathogenesis, Manifestations, Laboratory, Morphology, Complications & Metastases
1. Overview & Epidemiology
Pancreatic cancer refers predominantly to infiltrating ductal adenocarcinoma, the most common exocrine malignancy of the pancreas. It is the 3rd leading cause of cancer death in the United States (behind lung and colon). Despite being less common than those two, it has one of the highest mortality rates of any cancer - 5-year survival is approximately 12%, largely because >80% of patients present with surgically unresectable disease.
- ~64,000 Americans diagnosed per year
- 80% of cases occur between ages 60-80
- Mean time from diagnosis to death is often just months
2. Etiology (Risk Factors)
| Risk Factor | Notes |
|---|
| Smoking | Strongest environmental risk - doubles the risk |
| Chronic pancreatitis | Both risk factor AND possible manifestation of the cancer |
| Long-standing diabetes | Increased risk; new-onset diabetes in older adults can be the first sign |
| Age | 80% of cases between 60-80 years |
| Familial/Genetic | Germline BRCA2 mutations (~10%), mismatch repair gene mutations, PALB2, ATM, CDKN2A |
| Obesity | Modestly elevated risk |
Note: Chronic pancreatitis and diabetes can be caused by pancreatic cancer too (e.g., a head-of-pancreas tumor obstructs the duct, causing pancreatitis in the distal pancreas). About 1% of older adults with new-onset diabetes harbor unsuspected pancreatic cancer.
3. Pathogenesis
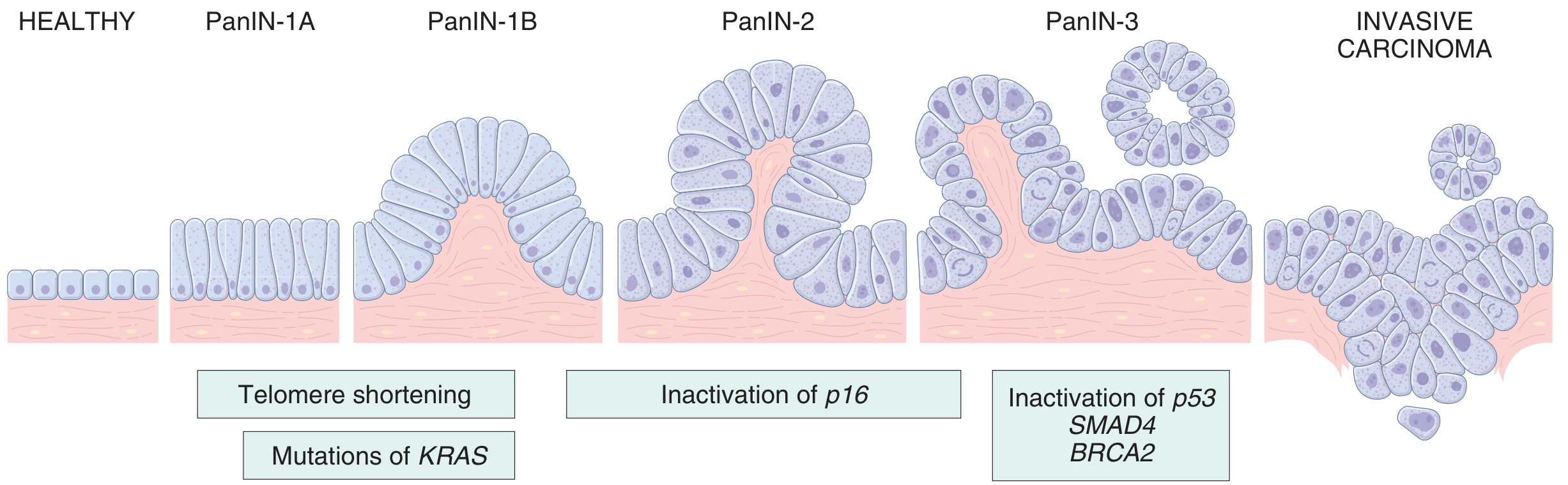
Pancreatic cancer arises from a stepwise accumulation of mutations through Pancreatic Intraepithelial Neoplasia (PanIN) - microscopic precursor lesions in small ducts. >85% of pancreatic cancers arise from PanIN.
The progression model:
PanIN progression model - Robbins & Kumar Basic Pathology
Key Molecular Alterations (in order of acquisition):
Early (PanIN-1):
- Telomere shortening - allows chromosomal instability
- KRAS mutation (chr 12p) - present in >90% of pancreatic cancers. Activating point mutation impairs GTPase activity, leaving KRAS constitutively active. This drives uncontrolled proliferation via the MAPK and PI3K pathways.
Intermediate (PanIN-2):
- CDKN2A/p16 inactivation (chr 9p) - present in ~30%. Encodes two suppressors: p16/INK4a (blocks CDK4, halts cell cycle at G1) and ARF (stabilizes p53). Inactivated by point mutations or homozygous deletion.
Late (PanIN-3 / high-grade):
- TP53 inactivation (chr 17p) - present in 70-75%. Removes the key checkpoint for DNA damage response, apoptosis, and senescence.
- SMAD4 inactivation (chr 18q) - present in 55%. Highly specific to pancreatic cancer. SMAD4 mediates TGF-β tumor suppression signaling. Its loss is near-unique to pancreatic cancer among all solid tumors.
- BRCA2 - mutated late in a subset of cases (both germline and somatic)
Summary table of key mutations:
| Gene | Chr | Frequency | Function |
|---|
| KRAS | 12p | >90% | GTPase signal transducer (oncogene) |
| TP53 | 17p | 70-75% | DNA damage response, apoptosis |
| SMAD4 | 18q | 55% | TGF-β tumor suppressor |
| CDKN2A/p16 | 9p | ~30% | Cell cycle brake (G1/S checkpoint) |
4. Morphologic Features
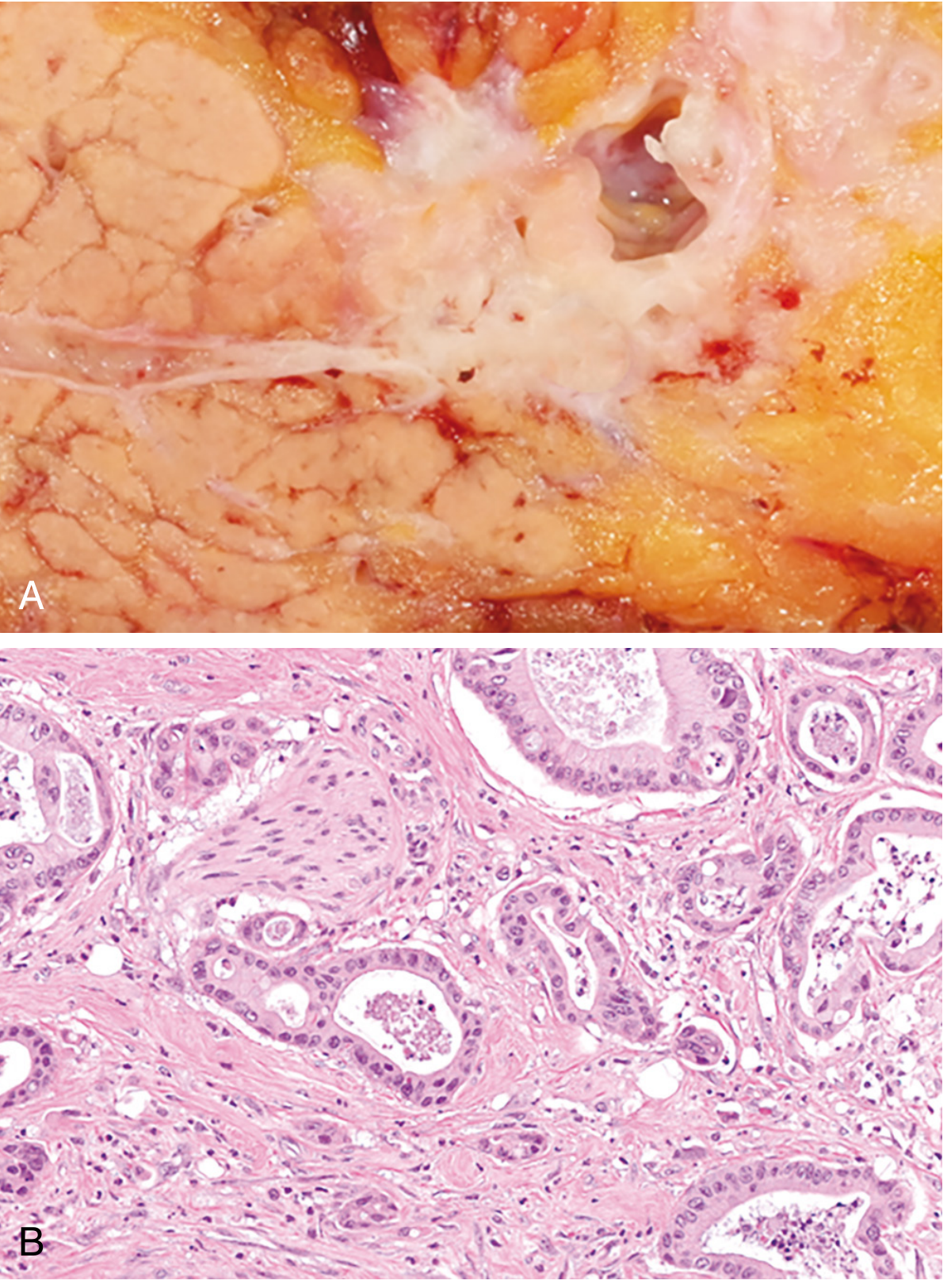
Gross (Macroscopic):
- 60% arise in the head of the pancreas; 15% in the body; 5% in the tail; 20% diffuse
- Hard, gray-white, stellate, poorly defined mass
- Highly invasive even at early stages
- Head-of-pancreas tumors typically obstruct the common bile duct → biliary dilation, jaundice
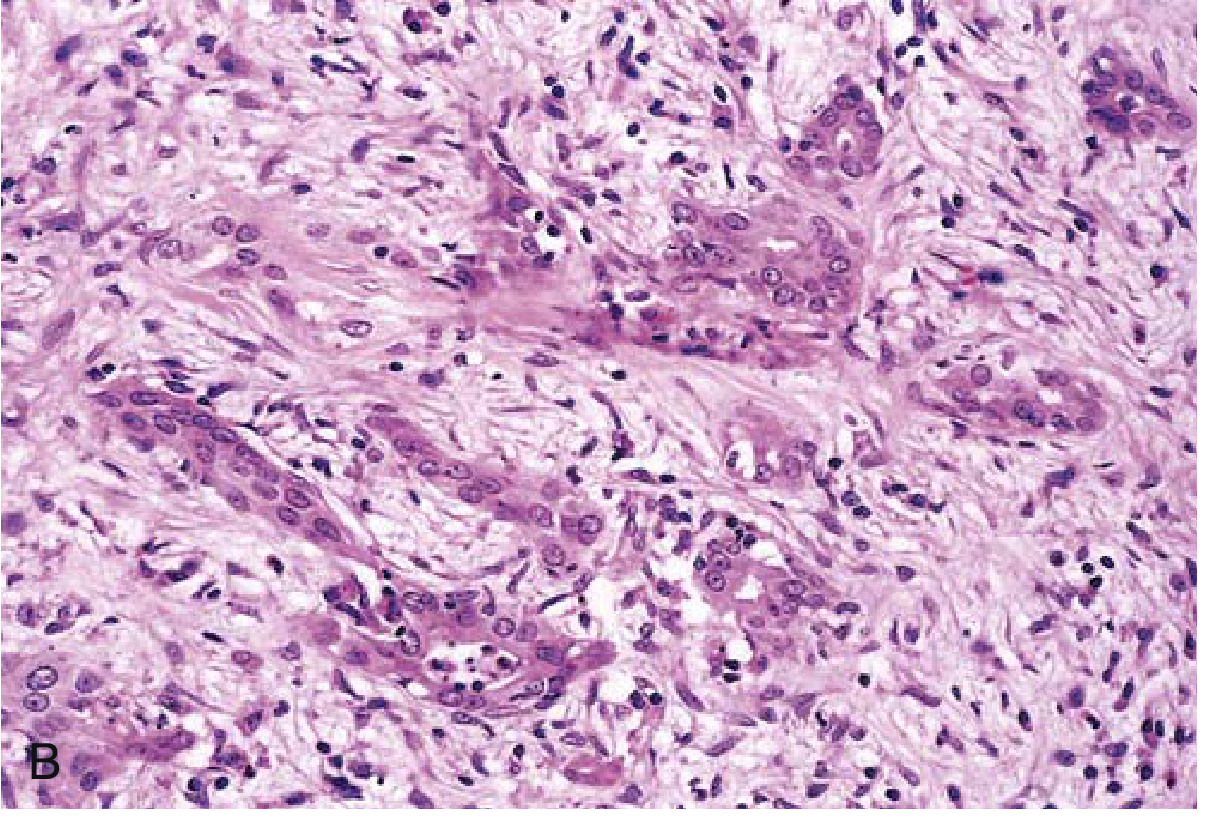
Microscopic (Histology):
Fig: (A) Gross white mass centered on the pancreatic duct. (B) Moderately to poorly formed malignant glands within densely fibrotic stroma, with perineural invasion - Robbins, Cotran & Kumar
Fig: Poorly formed glands in a densely desmoplastic stroma - Robbins & Kumar Basic Pathology
Key histological features:
- Moderately to poorly differentiated adenocarcinoma
- Abortive gland formation with mucin secretion
- Dense desmoplastic stroma (intense host fibrotic reaction) - this stromal reaction is a hallmark
- Perineural invasion - classic and important (accounts for pain)
- Lymphovascular invasion - commonly seen
- Aggressive, deeply infiltrative growth pattern even in "early" lesions
5. Clinical Manifestations
Pancreatic cancer remains silent until it obstructs or invades adjacent structures. This is why most patients present late.
| Symptom | Mechanism | Notes |
|---|
| Abdominal/back pain | Perineural invasion, retroperitoneal involvement | Usually the first symptom; by this point, often unresectable |
| Obstructive jaundice | Common bile duct obstruction by head lesion | Painless jaundice is classic for head of pancreas |
| Courvoisier sign | CBD obstruction → gallbladder distension | Palpably enlarged, non-tender gallbladder + painless jaundice |
| New-onset diabetes | Islet cell destruction, duct obstruction causing pancreatitis | Can be the first clue in ~1% of older adults |
| Weight loss, anorexia, malaise | Advanced disease, cancer cachexia | Profound loss of skeletal muscle and visceral fat |
| Migratory thrombophlebitis (Trousseau sign) | Tumor secretes procoagulants and platelet-aggregating factors | Occurs in ~10% of patients |
6. Laboratory Features
| Test | Finding | Clinical Significance |
|---|
| CA 19-9 | Elevated | Most commonly used tumor marker; NOT sensitive or specific enough for screening, but useful for monitoring treatment response |
| CEA | Elevated | Similarly not specific enough for screening |
| Circulating tumor DNA (ctDNA) | Often elevated | Useful for treatment monitoring but lacks sensitivity for early detection |
| Liver function tests | Elevated bilirubin, ALP (obstructive pattern) | With biliary obstruction |
| Blood glucose | Elevated | New-onset diabetes |
| Amylase/Lipase | May be elevated if duct obstruction causes pancreatitis | |
USPSTF does not recommend screening the general population due to poor sensitivity/specificity of available tests. Surveillance is recommended only for high-risk individuals with germline mutations (BRCA2, PALB2, ATM, Lynch syndrome).
Imaging:
- Endoscopic ultrasound (EUS) - best for small lesions and tissue sampling
- CT scan (pancreatic protocol) - standard for staging; assesses resectability
- ERCP / MRCP - evaluates biliary/pancreatic duct involvement
7. Complications
| Complication | Mechanism |
|---|
| Biliary obstruction | Tumor in pancreatic head compresses common bile duct |
| Duodenal obstruction | Tumor invades or compresses the duodenum |
| Malabsorption/steatorrhea | Pancreatic duct obstruction → exocrine insufficiency |
| Diabetes mellitus | Islet cell destruction or duct obstruction-induced pancreatitis |
| Migratory thrombophlebitis | Hypercoagulable state (Trousseau syndrome) |
| Cancer cachexia | Profound wasting, systemic cytokines |
| Chronic pain | Perineural invasion and celiac plexus involvement |
| Gastric varices/portal hypertension | If splenic or portal vein is invaded |
8. Metastases
Pancreatic cancer metastasizes early and widely. The pattern follows:
Local/Regional spread (most common and earliest):
- Retroperitoneal invasion (wraps around vessels and nerves)
- Peripancreatic lymph nodes → gastric, mesenteric, omental, portahepatic nodes
- Direct invasion of: spleen, adrenal glands, transverse colon, stomach, vertebral column
- Encasement of major vessels (SMA, celiac trunk, portal vein) = unresectable
Distant metastases:
- Liver - most common distant site; liver is often massively enlarged with metastatic deposits
- Lungs
- Bones (less common)
- Peritoneal seeding (carcinomatosis)
The high rate of unresectability (>80% at diagnosis) is driven by both local vascular invasion and distant metastases - most commonly to the liver.
Key Concepts Summary
- Most common type: Infiltrating ductal adenocarcinoma
- Location: 60% in the head
- Key precursor lesion: PanIN (pancreatic intraepithelial neoplasia)
- Most common mutation: KRAS (>90%)
- Hallmark histology: Desmoplastic stroma + poorly formed glands + perineural invasion
- Classic presentation: Painless jaundice (head lesion) OR pain (late finding)
- Trousseau sign: Migratory thrombophlebitis in 10%
- Best tumor marker: CA 19-9 (for monitoring, not screening)
- 5-year survival: ~12% (dismal due to late presentation)
- Most common metastatic site: Liver
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar - Basic Pathology