Explain antianginal drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information to write a thorough answer. Let me compile it:
Antianginal Drugs
Angina pectoris occurs when myocardial oxygen demand exceeds supply. The three main patterns are: stable (effort-induced) angina from fixed atherosclerotic obstruction, unstable angina from plaque rupture/thrombosis, and Prinzmetal/vasospastic angina from coronary artery spasm. All antianginal drugs work by improving the O2 supply-demand balance.
The Four Drug Classes
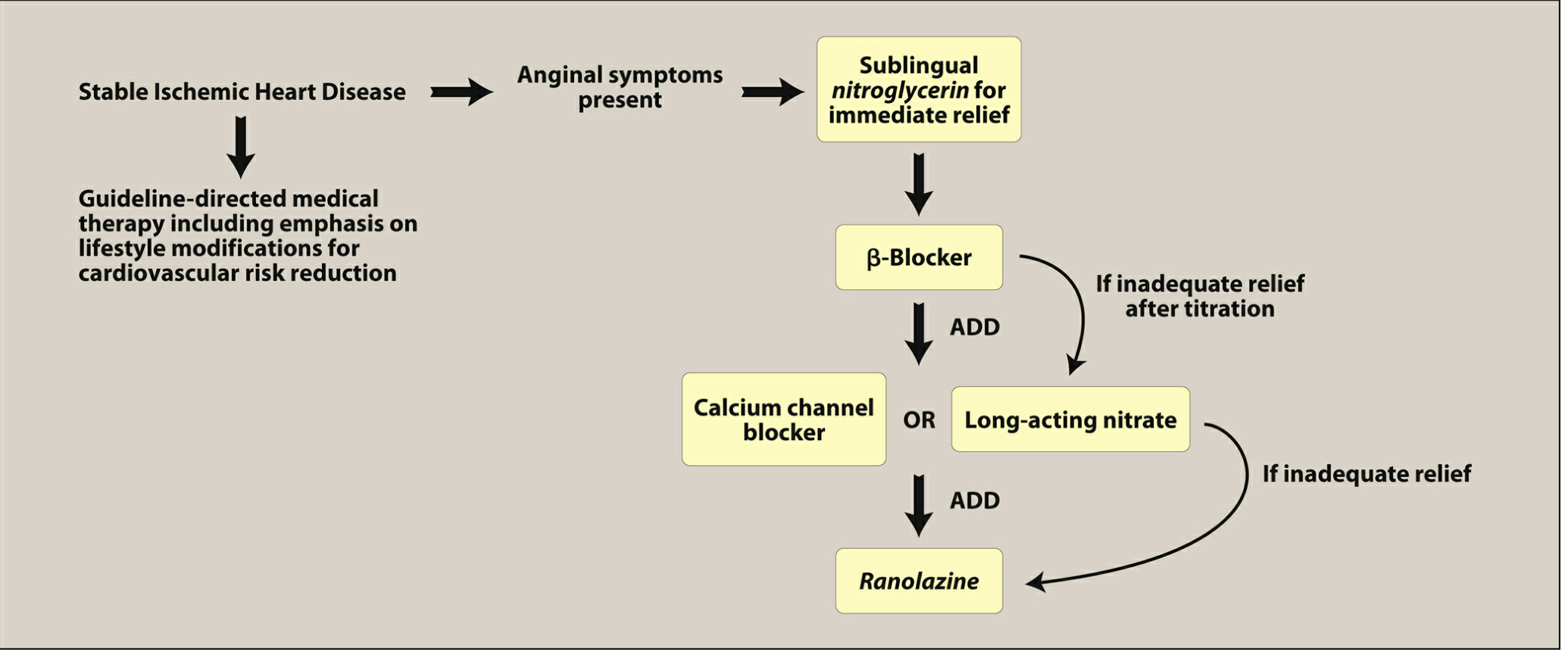
Figure: Treatment algorithm for stable ischemic heart disease - Lippincott Pharmacology
1. Beta-Adrenergic Blockers (First-Line)
Mechanism: Block β1 receptors → decreased heart rate, contractility, and cardiac output → reduced myocardial O2 demand. Effective at rest and during exertion.
Key drugs:
- Propranolol (prototype, non-selective β1+β2)
- Metoprolol and atenolol (cardioselective β1 - preferred)
- Carvedilol, labetalol (also have α-blocking effects)
Clinical use:
- First-line for stable effort-induced angina
- Reduce risk of death and MI in post-MI patients
- Improve mortality in heart failure with reduced ejection fraction (HFrEF)
Contraindications and cautions:
- Avoid in vasospastic (Prinzmetal) angina - can worsen coronary spasm
- Avoid in severe bradycardia and AV block
- Avoid non-selective agents in asthma (bronchospasm via β2 blockade)
- Mask hypoglycemia symptoms in diabetics (except diaphoresis)
- Agents with intrinsic sympathomimetic activity (ISA) like pindolol should be avoided in angina and post-MI
- Never stop abruptly - taper over 2-3 weeks to prevent rebound angina, MI, and hypertension
2. Calcium Channel Blockers (CCBs)
Mechanism: Block L-type calcium channels in vascular smooth muscle and myocardium → arterial vasodilation (reduces afterload) + decreased heart rate and contractility (non-DHPs). Coronary vasodilation is the main benefit in vasospastic angina.
A. Dihydropyridines (DHPs) - Peripheral vasodilators
- Amlodipine, nifedipine (ER), felodipine, nicardipine
- Minimal cardiac conduction effects; mainly arteriolar vasodilators
- Reflex tachycardia can occur (sympathetic activation from BP drop)
- Amlodipine is preferred for vasospastic angina
- Short-acting nifedipine is avoided in CAD (increased MI risk)
B. Non-Dihydropyridines - Central cardiac effects
- Verapamil: Most negative inotropic; slows AV conduction and sinus rate; weak vasodilator. Contraindicated in preexisting AV conduction abnormalities.
- Diltiazem: Intermediate profile - slows AV conduction + coronary vasodilator. Useful in variant angina.
Selectivity ranking (peripheral to central): Amlodipine > Diltiazem > Verapamil
Important: Non-DHPs (verapamil, diltiazem) can worsen HFrEF due to their negative inotropic effects - avoid in this population.
3. Organic Nitrates
Mechanism: Intracellularly converted to nitric oxide (NO) → activates guanylate cyclase → increased cGMP → dephosphorylation of myosin light chain → vascular smooth muscle relaxation.
Two main effects:
- Venodilation (large veins) → reduces preload (venous return) → reduces myocardial O2 demand
- Coronary artery dilation → increases O2 supply (major effect in variant angina)

Key formulations:
| Drug | Route | Onset | Use |
|---|---|---|---|
| Nitroglycerin (NTG) | Sublingual tablet/spray | ~1 min | Acute attack relief (all angina types) |
| NTG transdermal patch | Skin | Delayed | Prophylaxis (12h on, 12h off) |
| NTG IV | Intravenous | Rapid | Unstable angina/ACS |
| Isosorbide dinitrate | Oral | 15-30 min | Prophylaxis |
| Isosorbide mononitrate | Oral | ~30 min | Prophylaxis (better bioavailability, no first-pass) |
Nitroglycerin undergoes extensive hepatic first-pass metabolism, so it is given sublingual or transdermally. Isosorbide mononitrate has better oral bioavailability.
Adverse effects:
- Headache (most common - due to cerebral vasodilation)
- Postural hypotension, flushing, reflex tachycardia at high doses
- Dangerous hypotension with PDE-5 inhibitors (sildenafil, tadalafil) - combination is contraindicated
Tolerance: Develops rapidly due to vessel desensitization. Prevented by a 10-12 hour nitrate-free interval (usually overnight). Exception: in variant angina (which worsens in the morning), the free interval should be in the late afternoon instead.
4. Sodium Channel Blocker - Ranolazine (Newer Agent)
Mechanism: Inhibits the late inward Na+ current (late I-Na) → reduces intracellular Na+ → reduces Ca2+ overload via the Na+/Ca2+ exchanger → decreases diastolic wall tension, contractility, and myocardial O2 demand. Does not affect heart rate or blood pressure significantly.
Use: Add-on therapy for stable angina when other agents fail. Approved in the US.
Adverse effects / cautions:
- Prolongs QT interval (but has not been associated with torsades de pointes in most patients)
- Inhibits metabolism of digoxin and simvastatin
- Less effective in women
- Multiple drug interactions
5. Newer and Investigational Antianginals
| Drug/Class | Mechanism |
|---|---|
| Ivabradine | Blocks If (funny current) in sinoatrial node → pure heart rate reduction without affecting contractility |
| Trimetazidine | pFOX inhibitor - inhibits fatty acid oxidation (LC-3KAT) → shifts metabolism to glucose oxidation, less O2 per ATP. Used in many countries (not USA) |
| Nicorandil | Potassium channel activator + nitrate-like → dual vasodilation |
| Perhexiline | Shifts cardiac metabolism (fatty acid → glucose); limited by CYP2D6-dependent toxicity |
| Fasudil | Rho-kinase inhibitor |
| L-arginine | Nitric oxide donor |
Drug Selection by Angina Type and Comorbidities
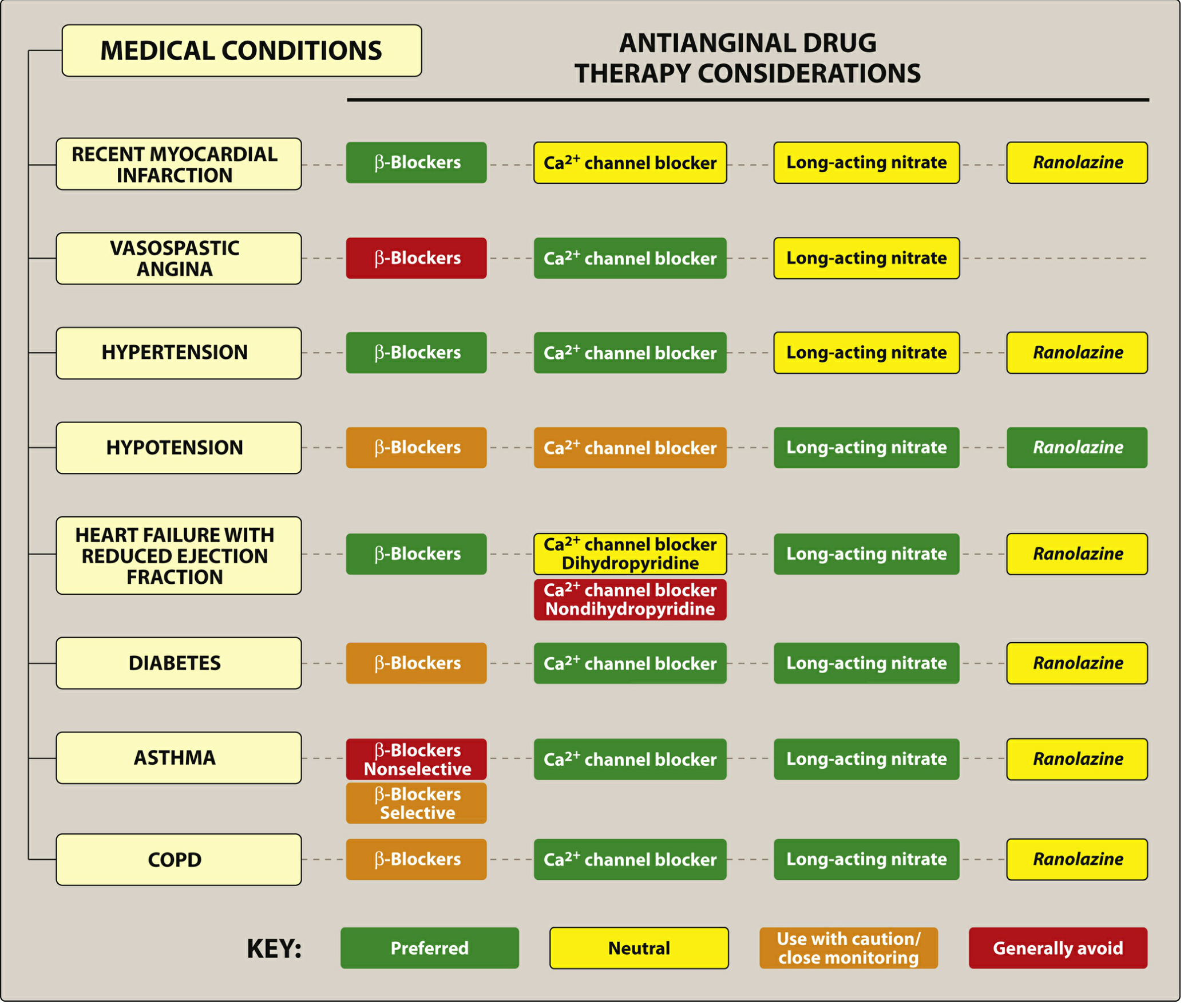
Figure: Antianginal Drug Therapy Considerations by Comorbidity - Lippincott Pharmacology
| Condition | Preferred | Avoid |
|---|---|---|
| Stable angina | Beta-blocker (first-line) + CCB or long-acting nitrate | - |
| Vasospastic (Prinzmetal) | CCBs + nitrates | Beta-blockers (can worsen spasm) |
| Unstable angina/ACS | Antiplatelet + heparin + percutaneous intervention | - |
| Post-MI | Beta-blockers (reduce mortality) | - |
| HFrEF | Beta-blockers, dihydropyridine CCBs | Non-DHP CCBs (worsen HF) |
| Asthma | Selective CCBs; nitrates | Non-selective beta-blockers |
| Hypertension | Beta-blockers, CCBs (both lower BP) | - |
| Bradycardia/AV block | Nitrates, DHPs | Beta-blockers, verapamil, diltiazem |
Key Points Summary
- The primary mechanism of most antianginal drugs is reducing myocardial O2 demand (beta-blockers: reduce HR, contractility; nitrates: reduce preload; CCBs: reduce afterload/HR/contractility)
- Increased O2 supply via coronary dilation is the main effect of nitrates and CCBs in vasospastic angina
- Sublingual nitroglycerin is the drug of choice for acute anginal attacks for all patients
- Beta-blockers are first-line for chronic stable angina and the only class with proven mortality benefit (in post-MI and HFrEF)
- Nitrate tolerance is prevented by a 10-12 hour drug-free interval daily
- PDE-5 inhibitors (sildenafil) + nitrates = absolutely contraindicated (severe hypotension)
- Beta-blockers must be tapered when discontinuing, never stopped abruptly
Sources: Lippincott Illustrated Reviews Pharmacology, 7th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed. | Katzung's Basic and Clinical Pharmacology, 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.