Classification of ILD radiology
Reading File
Finding Sources
Finding Sources
Searching the Web
classification of ILD interstitial lung disease radiology HRCT patterns 2022 2023
Finding Sources
Finding Sources
Searching Images
ILD interstitial lung disease HRCT classification patterns UIP NSIP
Reading File
Reading File
Reading Web Page
https://www.dirjournal.org/articles/radiologic-patterns-of-i…
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a detailed answer. Let me compile the full classification.
Classification of ILD Radiology
Interstitial lung diseases (ILDs) are a heterogeneous group of diffuse parenchymal disorders with varying degrees of inflammation and fibrosis affecting >200 conditions. HRCT (high-resolution CT) is central to diagnosis, serving as the cornerstone of multidisciplinary discussion.
Broad Classification Framework (2025 ERS/ATS Update)
The 2025 European Respiratory Society/American Thoracic Society consensus update organizes ILDs into three CT-based pattern groups:
- Interstitial patterns (fibrotic and non-fibrotic)
- Alveolar filling disorders
- Rare or unclassified disorders
I. IDIOPATHIC INTERSTITIAL PNEUMONIAS (IIPs)
The 2013 ATS/ERS consensus classification (still foundational) groups IIPs clinically and radiologically:
| Clinical Entity | Histological Pattern | Primary HRCT Features |
|---|---|---|
| IPF | UIP | Subpleural/basal reticular + honeycombing ± traction bronchiectasis |
| NSIP | NSIP | Bilateral ground-glass + reticulation; subpleural sparing; traction bronchiectasis; honeycombing rare |
| COP (Cryptogenic OP) | Organising pneumonia | Peripheral/peribronchovascular consolidation ± ground-glass |
| AIP (Acute IP) | Diffuse alveolar damage | Diffuse ground-glass ± traction bronchiectasis |
| RB-ILD | Respiratory bronchiolitis | Diffuse patchy centrilobular ground-glass nodules |
| DIP | DIP | Bilateral ground-glass (lower lobe); limited emphysema |
| LIP | LIP | Ground-glass + thin-walled cysts |
| IPPFE | Pleuroparenchymal fibroelastosis | Bilateral upper lobe irregular pleural thickening + subpleural reticular pattern |
II. UIP HRCT Diagnostic Categories (ATS/ERS/JRS/ALAT Guidelines)
This is the most clinically critical classification for IPF diagnosis:
| Category | Distribution | Key Features |
|---|---|---|
| Typical UIP | Subpleural, basal predominant; often heterogeneous | Honeycombing ± peripheral traction bronchiectasis; mild GGO variably present |
| Probable UIP | Subpleural, basal predominant | Reticular pattern + peripheral traction bronchiectasis; no honeycombing |
| Indeterminate for UIP | Subpleural, basal | Subtle reticulation; mild GGO or distortion; distribution not typical |
| Alternative Diagnosis | Peribronchovascular, perilymphatic, upper/mid-lung | Cysts, marked mosaic attenuation, profuse micronodules, consolidation, centrolobular nodules |
Typical UIP is virtually pathognomonic for IPF when clinical features support it — the "propeller blade distribution" where fibrosis creeps peripherally from the posterior basal regions up into anterior upper lobes is characteristic.
HRCT comparison of UIP (irreversible fibrosis) vs NSIP (relatively reversible)
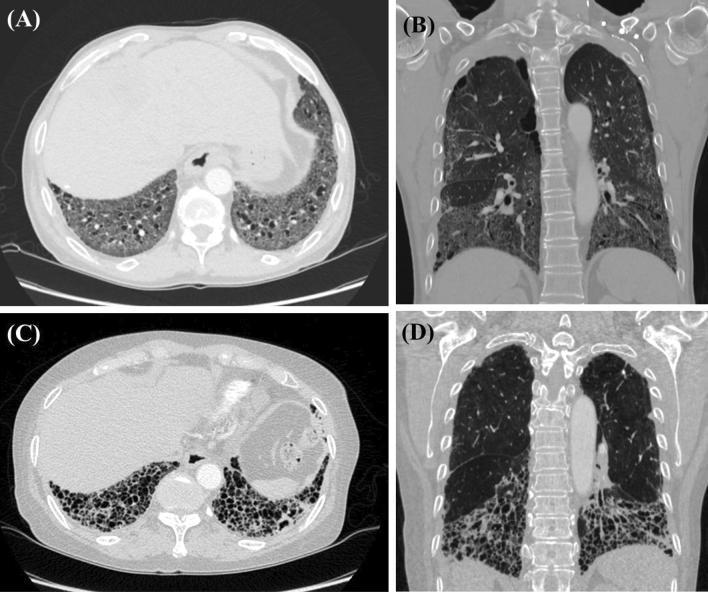
UIP (A/B): extensive subpleural honeycombing, traction bronchiectasis, lower-zone architectural distortion. NSIP (C/D): bilateral symmetric ground-glass with mild traction bronchiectasis, basal predominance.
III. HRCT Pattern Groups — Fibrotic vs Non-Fibrotic
Fibrotic Interstitial Patterns
Distortion, traction bronchiectasis, and honeycombing indicate often irreversible remodeling:
| Pattern | Hallmark HRCT Features | Key Associations |
|---|---|---|
| UIP | Honeycombing, traction bronchiectasis, subpleural basal reticulation | IPF, RA-ILD, asbestosis, CTD, chronic HP |
| NSIP | Bilateral GGO + reticulation, subpleural sparing, traction bronchiectasis, honeycombing rare | CTD-ILD (SSc, DM/PM), drug-induced |
| Chronic HP (fibrotic) | Reticulation, traction bronchiectasis, honeycombing (mid-zone or variable); air trapping on expiratory CT | Antigen inhalation |
| IPPFE | Upper lobe irregular pleural thickening + subpleural fibrosis | Idiopathic, post-transplant |
| BIP (new 2025) | Airway-centered fibrosis, tree-in-bud, centrilobular nodules, peribronchiolar reticulation | HP, CTD, aspiration, drug-induced |
Non-Fibrotic / Inflammatory Patterns
Reflect inflammation or acute injury without established fibrosis — generally more treatment-responsive:
| Pattern | Hallmark HRCT Features | Key Associations |
|---|---|---|
| Organising pneumonia (OP/COP) | Peripheral ± peribronchovascular consolidation; "atoll sign" (reversed halo); can migrate | Idiopathic (COP), drug, infection, CTD |
| DIP | Diffuse bilateral GGO (lower zones); limited emphysema | Smoking-related |
| RB-ILD | Centrilobular ground-glass nodules, bronchial wall thickening | Smoking-related |
| Acute eosinophilic / AIP | Diffuse GGO; bilateral opacities ± traction bronchiectasis (organising phase) | Idiopathic, drug-induced |
IV. Classification by Etiology (Clinical)
| Category | Examples | Predominant HRCT Pattern |
|---|---|---|
| Idiopathic IIPs | IPF, NSIP, COP, AIP, RB-ILD, DIP, LIP, IPPFE | See table above |
| CTD-ILD | SSc, RA, PM/DM, SLE, Sjögren's | NSIP most common; also UIP, LIP, OP |
| Hypersensitivity pneumonitis (HP) | Bird/farmer's lung | Centrilobular nodules (acute), mosaic attenuation, air trapping (subacute), fibrosis (chronic) |
| Smoking-related | DIP, RB-ILD, PLCH, combined pulmonary fibrosis/emphysema (CPFE) | Cysts (PLCH), GGO (DIP/RB-ILD), mixed fibrosis + emphysema (CPFE) |
| Occupational/Environmental | Silicosis, CWP, asbestosis, berylliosis | Upper-lobe nodules (silicosis/CWP), pleural plaques + UIP (asbestosis) |
| Granulomatous | Sarcoidosis | Peribronchovascular nodules; bilateral hilar lymphadenopathy; Scadding stages I–IV |
| Drug-induced | Amiodarone, methotrexate, immunotherapy | Heterogeneous — OP, NSIP, or DAD patterns |
| Alveolar filling disorders | PAP, eosinophilic pneumonia, DAH | Crazy-paving (PAP); peripheral consolidation/GGO |
| Rare/Cystic | LAM, PLCH, BHD syndrome | Thin-walled cysts (LAM: diffuse; PLCH: upper/mid with nodules) |
V. Key Discriminating HRCT Features
| Feature | Significance |
|---|---|
| Honeycombing | Irreversible fibrosis; hallmark of definite UIP |
| Traction bronchiectasis | Fibrotic distortion; present in both UIP and NSIP |
| Subpleural sparing | Characteristic of NSIP (vs. subpleural predominance of UIP) |
| Air trapping (expiratory CT) | Bronchiolocentric disease; key for chronic HP vs UIP/NSIP |
| Peribronchovascular distribution | Sarcoidosis, OP, lymphangitic carcinomatosis |
| Bilateral hilar lymphadenopathy | Sarcoidosis |
| Upper-lobe predominance | Sarcoidosis, HP (some), IPPFE, silicosis, PLCH |
| Crazy-paving pattern | PAP, ARDS, PCP infection |
| Reversed halo / atoll sign | Organising pneumonia |
| Cysts (bilateral diffuse) | LAM (women), PLCH (upper/mid), LIP (cysts + GGO) |
Reversibility Perspective
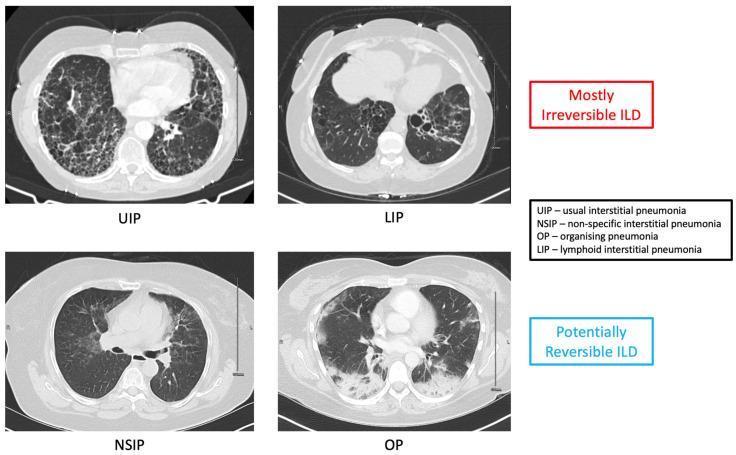
| Mostly Irreversible | Potentially Reversible |
|---|---|
| UIP/IPF, LIP | NSIP (cellular > fibrotic), OP/COP |
Sources
- Grainger & Allison's Diagnostic Radiology, Chapter 9 (ILD HRCT classification, UIP diagnostic categories)
- Harrison's Principles of Internal Medicine 22e (2025), Chapter 304 (ILD)
- Washington Manual of Medical Therapeutics (IIPs classification)
- 2025 ERS/ATS ILD Classification pictorial review — Diagnostic and Interventional Radiology
This is a shared conversation. Sign in to Orris to start your own chat.