Explain in details nutrition care in icu and anaesthesiology subject based on latest findings and guidelines without hallucinating
Reading File
Finding Sources
Finding Sources
Searching PubMed
"nutritional support" AND "critical care" AND "intensive care unit"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading Article
PMID: 38799065
Reading File
Reading Article
PMID: 39317131
Reading Article
PMID: 42095216
Loading Image
I now have everything needed for a comprehensive, well-cited answer. Let me compose it.
Nutrition Care in the ICU and Anaesthesiology - A Detailed Evidence-Based Review
1. Why Nutrition Matters in Critical Illness
Critical illness - whether from major surgery, sepsis, trauma, burns, respiratory failure, or cardiac failure - triggers a profound hypermetabolic and hypercatabolic state. Cytokine release, neuroendocrine stress responses, and systemic inflammation drive catabolism that exceeds the patient's ability to self-nourish voluntarily. The consequences are predictable and serious:
- Progressive loss of lean body mass (muscle wasting)
- Impaired wound healing and immune function
- Increased infection rates and ICU length of stay
- Higher mortality
Numerous studies have confirmed that energy deficit in critical illness correlates with longer ICU stays, greater incidence of infectious complications, and increased mortality. Up to 40% of ICU admissions have moderate-to-severe malnutrition on presentation. This makes nutritional support a standard-of-care component, not an optional add-on.
Barash Clinical Anesthesia, 9e, p. 4855: "Poor nutritional status is associated with increased mortality and morbidity among critically ill patients. Therefore, appropriate nutrition is an important aspect of critical care and adequate nutritional support should be considered a standard of care."
2. Phases of Critical Illness and Nutritional Goals
The metabolic trajectory of ICU illness is not linear. Understanding the phases prevents both under- and over-feeding:
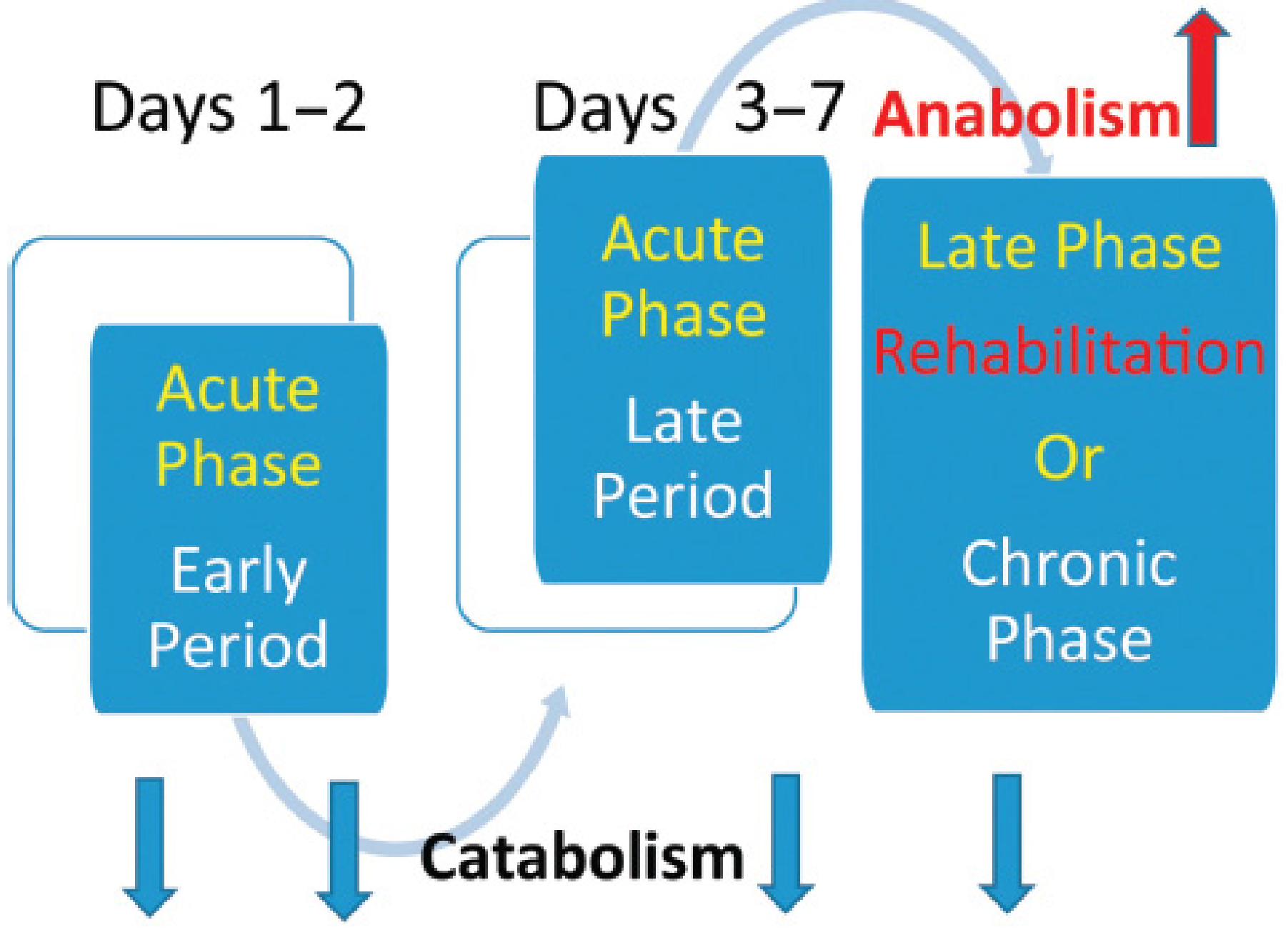
Figure: Acute (catabolic, Days 1-7) and late/rehabilitation (anabolic) phases following critical illness/injury. From Mulholland & Greenfield's Surgery, 7e.
| Phase | Timing | Metabolic State | Nutritional Approach |
|---|---|---|---|
| Early Acute | Days 1-2 | Peak catabolism, fluid shifts | Permissive underfeeding (trophic feeding), avoid overfeeding |
| Late Acute | Days 3-7 | Persistent catabolism | Gradual escalation toward target |
| Rehabilitation | Days 7+ | Anabolic window | Full caloric and protein delivery, support muscle recovery |
3. Nutritional Risk Screening and Assessment
3.1 Validated Screening Tools
All patients admitted to the ICU should undergo a nutritional risk assessment. Two tools are well validated:
- NUTRIC score - incorporates age, APACHE II/SOFA, days from hospital to ICU admission, number of comorbidities, and IL-6 (if available). Scores ≥5 (without IL-6) or ≥6 (with IL-6) identify high nutritional risk.
- NRS-2002 - evaluates nutritional status and disease severity; widely used for surgical patients.
Mulholland & Greenfield's Surgery, 7e, p. 135: "Upon admission to the ICU, some assessment of nutritional risk should be performed. There are several validated tools, including the NUTRIC and NRS 2002, both of which evaluate nutritional status and disease severity."
3.2 Serum Markers - What NOT to Use
Albumin, prealbumin (transthyretin), and transferrin are negative acute-phase reactants. In acute illness, hepatic protein synthesis shifts toward inflammatory proteins, vascular permeability increases, and these markers fall regardless of nutritional intake. ASPEN 2021 guidelines explicitly recommend against using albumin or prealbumin as proxies for nutritional status in critically ill patients. Their values must be interpreted in the full clinical context.
Sabiston Textbook of Surgery, p. (Ch 11): "ASPEN recommends against using such markers as proxies for nutritional status, and their values should be interpreted in conjunction with a patient's hospital course and clinical status."
3.3 Energy Expenditure Measurement
Indirect calorimetry (measuring VO2 and VCO2 to calculate resting energy expenditure) is the gold-standard method. However, it is not universally available and can overestimate basal energy expenditure by 10-15% in stressed/ventilated patients. Predictive equations (Harris-Benedict, Penn State, etc.) are simpler but less accurate. Over 200 formulas have been proposed; none is universally endorsed by ASPEN or SCCM as the preferred equation.
A recent 2025 systematic review (PMID 41146556) highlights growing evidence for the use of indirect calorimetry to guide personalized energy delivery, rather than relying on fixed formula-based estimates.
4. Energy Requirements in the ICU
4.1 Current Caloric Targets
The 2021 ASPEN guidelines recommend:
12 to 25 kcal/kg/day
This is a deliberate reduction from older recommendations of 80-100% of predicted caloric needs. The evidence base includes the TARGET trial (energy-dense vs. routine enteral feeding), which failed to demonstrate mortality benefit with higher-calorie delivery.
Sabiston Textbook of Surgery: "The most recent (2021) ASPEN guidelines for the critically ill patient recommend feeding 12 to 25 kcal/kg/day. This represents a change from prior recommendations for higher-calorie feeding and is reflective of more recent evidence suggesting, at a minimum, a lack of harm of lower-calorie feeding."
4.2 Early Permissive Underfeeding vs. Full Feeding
- Early "full nutrition" is likely harmful and associated with higher infection rates in the first days of critical illness.
- The goal in the early acute phase is a caloric target below actual energy expenditure, with the aim of providing >80% of estimated total energy goals gradually by Day 3 to 4.
- Early enteral feeding (even at trophic rates) protects the intestinal epithelial barrier function and maintains microbiome diversity.
- A meta-analysis showed no significant difference in overall mortality between underfeeding and full feeding groups, but a subgroup fed more than one-third of caloric requirements showed lower mortality.
4.3 Hypocaloric (Permissive Underfeeding) in Obese Patients
In critically ill obese patients, a hypocaloric high-protein strategy is recommended:
- 11-14 kcal/kg actual body weight (or 22-25 kcal/kg ideal body weight)
- Protein: 2.0-2.5 g/kg ideal body weight/day
This differs from the approach of "permissive underfeeding" (1500 kcal/d, 40 g protein/d) - in obese patients, calories are restricted but protein is not.
5. Protein Requirements
Protein is proportionally more important than caloric substrate in critical illness. Adequate protein is required for:
- Wound healing
- Maintenance of lean body mass
- Immune function support
Current Recommendations
1.2 to 2.0 g/kg actual body weight/day is the target for most critically ill patients (SCCM/ASPEN guidelines).
Requirements may be higher in:
- Burns (up to 2.5 g/kg/day or more)
- Polytrauma
- Patients on continuous renal replacement therapy (CRRT), which removes amino acids
The High-Protein Controversy - Latest Evidence
A 2024 systematic review and meta-analysis (PMID 38799065, PeerJ, 17 RCTs, n=2,965) found:
No significant benefit of higher protein dosing (≥1.2 g/kg/day) vs. lower dosing on mortality, ICU LOS, hospital LOS, duration of mechanical ventilation, or incidence of acute kidney injury.
This aligns with the updated 2021 ASPEN guidelines, which stepped back from the push for high-protein supplementation. The optimal protein dose thus remains individualized and uncertain, especially in high-risk subpopulations.
6. Route of Nutrition: Enteral vs. Parenteral
6.1 Enteral Nutrition (EN) - First Choice
EN is the preferred route for nutritional support in patients with a functional gastrointestinal tract, for several reasons:
- Lower cost than parenteral nutrition
- Avoids complications of IV access (infection, thrombosis)
- Maintains gut barrier integrity - the gut mucosa depends on luminal nutrients for trophic effects; disuse leads to diminished sIgA production, bacterial overgrowth, altered mucosal immune defenses, and potential bacterial translocation
- Reduces infectious complications (meta-analyses confirm significant reductions vs. PN)
However, a large European RCT comparing early isocaloric EN vs. PN in adult critically ill patients with shock showed no reduction in mortality or secondary infections, and a greater risk of digestive complications including intestinal ischemia with early EN. This is an important caveat.
Schwartz's Principles of Surgery, 11e, p. 94: "While EN is recommended as the first choice for nutritional support in patients who can tolerate it, a recent large trial from Europe comparing early isocaloric EN vs. PN in adult critically ill patients with shock did not reduce mortality or the risk of secondary infections but was associated with a greater risk of digestive complications including intestinal ischemia."
6.2 Timing of Enteral Nutrition
Start within 24-48 hours of ICU admission (SCCM/ASPEN bundle; reaffirmed in ESPEN ICU guidelines).
- Enteral feeding should begin as soon as the patient is hemodynamically stable (adequate urine output is a practical guide).
- Presence of bowel sounds and passage of flatus/stool are NOT absolute prerequisites.
- High gastric residual volumes (>200 mL over 4-6 hours) or abdominal distension may warrant cessation and rate adjustment.
6.3 Gastric vs. Post-Pyloric Feeding
- Most critically ill patients can be fed safely into the stomach (gastric route).
- If gastric feeding intolerance persists despite prokinetic agents, convert to post-pyloric (nasojejunal) feeding.
- Despite early enthusiasm for post-pyloric feeds, studies show no clinically significant reduction in pneumonia, ICU length of stay, or mortality compared to gastric feeding.
- Routine monitoring of gastric residual volumes is no longer recommended (SCCM/ASPEN 2016 update).
6.4 Continuous vs. Intermittent Enteral Feeding
A 2026 updated meta-analysis (PMID 42095216, 22 RCTs, n=1,662) directly compared intermittent enteral nutrition (IEN) vs. continuous enteral nutrition (CEN):
| Outcome | IEN vs. CEN |
|---|---|
| Diarrhea | Significantly higher with IEN (RR 1.56) |
| Abdominal distension | Significantly higher with IEN (RR 1.68) |
| Constipation | Lower with IEN (RR 0.74) |
| ICU length of stay | Longer with IEN (MD +0.91 days) |
| ICU mortality | No significant difference |
| Aspiration pneumonia | No significant difference |
Conclusion: Continuous enteral feeding (CEF) is preferred for most critically ill patients, particularly those on mechanical ventilation. CEF may also promote protein anabolism by inhibiting protein breakdown.
6.5 Parenteral Nutrition (PN) - When and How
Indications:
- GI tract non-functional (obstruction, high-output fistula, GI ischemia, severe ileus)
- EN is not feasible or well-tolerated
- As supplement when EN is meeting <60% of energy/protein requirements after 1 week
Timing of PN:
- In low nutritional risk patients: delay PN initiation until Day 7-10. Earlier initiation was historically associated with higher infectious complications, though more recent data suggest this was driven by excessive caloric delivery rather than PN per se.
- In high nutritional risk patients (NUTRIC ≥5, severe malnutrition): start PN early if EN is not feasible.
Schwartz's Surgery, 11e, p. 100: "PN use is recommended for those critically ill or injured patients who are at high nutritional risk, when EN is not possible. Alternately, PN can also be used to supplement EN after 1 week of use if use of EN is unable to meet >60% of energy and protein requirements."
Total Parenteral Nutrition (TPN):
- Requires central venous access (high dextrose concentration: 15-25%)
- All macronutrients and micronutrients delivered via this route
Peripheral Parenteral Nutrition (PPN):
- Lower osmolality (dextrose 5-10%, protein 3%)
- Not suitable for severely malnourished patients or long-term use (>2 weeks)
- Use when central access unavailable or supplemental support needed short-term
Complications of PN to monitor:
- Line sepsis (catheter-related bloodstream infections)
- Hyperglycemia
- Hepatic steatosis/cholestasis
- Electrolyte imbalances
- Essential fatty acid deficiency (with fat-free solutions - manifests as dry scaly dermatitis, hair loss; prevent with periodic lipid emulsion infusions)
- Vitamin K deficiency (not in standard IV vitamin preparations - supplement weekly)
7. SCCM/ASPEN Nutrition Bundle - Summary of Core Recommendations
From McClave SA, Taylor BE, Martindale RG, et al. JPEN 2016;40(2):159-211:
- Assess all ICU patients on admission for nutritional risk; calculate energy and protein requirements.
- Initiate EN within 24-48 hours of onset of critical illness and ICU admission; increase to goals over first week.
- Reduce aspiration risk and improve tolerance: prokinetic agents, continuous infusion, chlorhexidine mouthwash, elevate head of bed 30-45°, consider diverting feeding level in GI tract.
- Implement feeding protocols with institution-specific strategies to promote EN delivery.
- Do NOT routinely monitor gastric residual volumes in ICU patients on EN.
- Start PN early when EN is not feasible/sufficient in high-risk or poorly nourished patients.
8. Enteral Formula Selection
Choice of formula depends on:
| Factor | Consideration |
|---|---|
| GI tract function | Intact: standard polymeric formula; Impaired absorption: peptide-based, MCT-enriched formula |
| Organ dysfunction | Renal failure, hepatic failure, pulmonary failure, diabetes - use organ-specific formulas |
| Diarrhea | Soluble fiber supplementation improves stool consistency |
| Malabsorption (IBD, short bowel) | Hydrolyzed protein formulas endorsed by guidelines |
| Standard care | Formulas rich in water-soluble dietary fiber are considered standard for surgical patients |
No single formula category has been proven conclusively superior in outcomes for all ICU patients. Institutional nutritional support committees generally develop cost-efficient formularies for common disease categories.
9. Immunonutrition
Immunonutrition refers to enteral or parenteral formulas enriched with specific pharmaconutrients designed to modulate immune function and reduce inflammatory/infectious morbidity.
9.1 Glutamine
- Best-studied immunonutrient
- Conditionally essential in critical illness; serves as a fuel for enterocytes and immune cells
- Strongest data in burns and trauma patients
- High-concentration glutamine formulas have the strongest evidence base among immunonutrients
Barash Clinical Anesthesia, 9e, p. 4856: "Specific enteral formulations, particularly those with high concentrations of glutamine, have the strongest data to support their use."
9.2 Arginine
- Precursor to nitric oxide; roles in wound healing, immune cell proliferation
- Benefit primarily in elective surgical patients and trauma
- Use remains controversial in sepsis (theoretical risk of excess nitric oxide production)
9.3 Omega-3 Polyunsaturated Fatty Acids (PUFAs)
- Anti-inflammatory mechanism (compete with arachidonic acid pathway)
- Some data suggest reduction in ICU length of stay; no mortality benefit demonstrated
- Current guidelines do not support the use of various fatty acid formulations as routine immunonutrition in critically ill patients.
Barash Clinical Anesthesia, 9e: "The use of various fatty acids is not supported by current guidelines."
9.4 Micronutrients (Trace Elements and Vitamins)
- Selenium, zinc, vitamins A, C, E - deficiencies common in critical illness
- Supplementation is generally considered safe
- Evidence supporting their use is of overall low quality and high risk of bias; should be interpreted with caution
- Vitamin K is not present in standard IV vitamin preparations; supplement weekly in PN patients
10. Glycemic Control and Nutrition
Hyperglycemia is common in critically ill patients as a result of the stress response, insulin resistance, and carbohydrate loading from nutritional support.
Historical Context
- Van den Berghe's landmark 2001 RCT showed intensive insulin therapy (glucose target <110 mg/dL) reduced ICU mortality by ~50% in surgical ICU patients.
- This led to widespread adoption of "tight glycemic control" protocols.
Current Practice
- Multiple subsequent trials failed to reproduce these benefits. The NICE-SUGAR trial (large multicenter RCT) showed increased mortality with tight glucose control (80-110 mg/dL) due to severe hypoglycemia.
- Tight glucose control (80-110 mg/dL) was widely abandoned.
Barash Clinical Anesthesia, 9e, p. 4850: "After an additional large, multicenter, multinational randomized controlled trial of intensive insulin therapy showed increased mortality in the tight glucose control group, the practice of maintaining blood glucose between 80 and 110 mg/dL was widely abandoned. Current serum glucose targets are somewhat variable, but most agree that 140 to 180 mg/dL is an acceptable goal in most patients."
Current target: 140-180 mg/dL in most critically ill patients - avoiding both hyperglycemia and dangerous hypoglycemia.
11. Refeeding Syndrome
A serious, potentially fatal complication of resuming caloric intake in malnourished patients.
Pathophysiology
Malnourished patients have depleted intracellular phosphate, potassium, and magnesium stores, with relative preservation of serum levels. On refeeding (EN or PN):
- Insulin release drives glucose, phosphate, potassium, and magnesium intracellularly
- Rapid drop in serum phosphate (hypophosphatemia), hypokalemia, hypomagnesemia
- Thiamine depletion may also occur (thiamine is required for glucose metabolism)
- The resultant electrolyte shifts can cause: fatal cardiac dysrhythmias, respiratory failure, seizures, hemolytic anemia, and encephalopathy
Risk Identification
A 2024 systematic review (PMID 39317131) noted that refeeding syndrome was observed in up to 52.5% of at-risk ICU patients, with related mortality ranging 15.6-83.3%. Critically ill patients are at particularly high risk due to baseline organ dysfunction.
Prevention
- Identify at-risk patients before initiating nutrition (prolonged starvation >5-7 days, low BMI, chronic alcohol use, long-term diuretics, etc.)
- Start feeding at low rates (10-20 kcal/kg/day) and escalate slowly over 4-7 days
- Supplement phosphate, potassium, magnesium, and thiamine proactively before and during early refeeding
- Monitor electrolytes closely (daily in the first week)
12. Feeding During Vasopressor Support
A frequently asked clinical question in anaesthesiology and critical care: is it safe to enterally feed hemodynamically unstable patients on vasopressors?
- A randomized trial comparing EN to PN in patients requiring vasoactive support showed EN was not associated with significantly worse outcomes.
- Cautious early EN can be attempted once vasopressors are stable or being weaned, but should be withheld in patients with signs of bowel ischemia (abdominal distension, rising lactate, absent bowel sounds with clinical concern).
- In the shock setting, early EN was associated with increased risk of intestinal ischemia in one large trial (see Section 6.1).
13. Special Populations
Burns
- Among the highest caloric and protein requirements
- Protein targets up to 2.5 g/kg/day or more
- Immunonutrition (glutamine) has the strongest evidence base here
- Early EN within 6-12 hours of burn injury is recommended
Obese ICU Patients (BMI >30)
- Hypocaloric high-protein strategy: 11-14 kcal/kg actual body weight (or 22-25 kcal/kg ideal body weight)
- Protein: 2.0-2.5 g/kg ideal body weight/day
Renal Failure / CRRT
- Standard protein targets (1.5-2.5 g/kg/day) - CRRT removes amino acids, so protein requirements are higher
- Restrict potassium and phosphorus in formula selection
- Avoid excessive fluid from PN
Perioperative Nutrition (Anaesthesiology Context)
Preoperative: In malnourished patients undergoing elective surgery, preoperative nutritional support should begin as soon as possible. A minimum of 2-4 weeks is required to derive clinical benefit.
Postoperative - Early EN: A systematic review of early enteral feeding within 24 hours of gastrointestinal surgery showed no effect on anastomotic leak and a reduction in mortality. Early EN in open abdomen patients reduces fistula formation.
Low-risk elective surgery: Healthy patients without malnutrition undergoing uncomplicated elective surgery can tolerate 10 days of partial starvation (maintenance IV fluids) without significant nutritional intervention, particularly if the GI tract resumes function quickly.
Key anaesthesiology consideration: Fasting before general anaesthesia (traditional NPO after midnight) has evolved. Enhanced Recovery After Surgery (ERAS) protocols now permit clear liquids up to 2 hours and solid food up to 6 hours before elective surgery, with preoperative carbohydrate loading reducing postoperative insulin resistance and catabolism.
14. Overfeeding - A Significant Hazard
Overfeeding is common when actual body weight is used in obese or fluid-overloaded patients, or when indirect calorimetry overestimates needs. Consequences include:
- Increased CO2 production - prolonged need for ventilatory support
- Increased oxygen consumption
- Hepatic steatosis / fatty liver
- Suppression of leukocyte function
- Hyperglycemia and increased infection risk
Schwartz's Surgery, 11e, p. 95: "Overfeeding may contribute to clinical deterioration via increased oxygen consumption, increased carbon dioxide production and prolonged need for ventilatory support, fatty liver, suppression of leukocyte function, hyperglycemia, and increased risk of infection."
Avoiding overfeeding in the early acute phase of critical illness is a universal recommendation across all guidelines.
15. Prolonged Critical Illness - PICS
Some patients who survive the acute phase enter a state of Persistent Inflammatory, Immunosuppressed, and Catabolic Syndrome (PICS) - chronic critical illness with persistent inflammation, immune dysfunction, and ongoing catabolism. These patients require aggressive nutritional support with high protein and caloric targets, in addition to physical rehabilitation. As patients enter the recovery/rehabilitation phase, total protein and caloric requirements significantly increase and anabolic support is the priority.
Summary Table: Key Nutritional Parameters
| Parameter | Recommendation | Source |
|---|---|---|
| Caloric target (general ICU) | 12-25 kcal/kg/day | ASPEN 2021 |
| Caloric target (obese) | 11-14 kcal/kg ABW/day | ASPEN |
| Protein (general) | 1.2-2.0 g/kg/day | SCCM/ASPEN |
| Protein (burns/trauma) | Up to 2.5 g/kg/day | ASPEN |
| Protein (obese) | 2.0-2.5 g/kg IBW/day | ASPEN |
| EN timing | Within 24-48 h of ICU admission | SCCM/ASPEN |
| PN timing (low-risk) | Delay to Day 7-10 | SCCM/ASPEN |
| Glycemic target | 140-180 mg/dL | SCCM/ADA |
| Gastric residual monitoring | Not routinely recommended | SCCM/ASPEN 2016 |
| EN route | Gastric first; post-pyloric if intolerant | SCCM/ASPEN |
| Feeding mode | Continuous preferred over intermittent | 2026 meta-analysis |
Key References
- McClave SA et al. SCCM/ASPEN Guidelines. JPEN 2016;40(2):159-211
- ASPEN Critical Care Guidelines, 2021 update
- ESPEN Guideline on Clinical Nutrition in the ICU (Singer P et al.)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - "Nutrition in the Critically Ill Patient" (p. 4855-4856)
- Mulholland & Greenfield's Surgery, 7e - "Nutritional Support in Critical Care" (p. 133-135)
- Schwartz's Principles of Surgery, 11e - "Enteral Nutrition" (p. 94-101)
- Sabiston Textbook of Surgery - "Nutritional Requirements of the Critically Ill Patient"
- Qin Y et al. No benefit of higher protein dosing in critically ill patients: systematic review and meta-analysis. PeerJ 2024. PMID 38799065
- Alencar LO et al. Nutritional therapy in ICU inpatients at risk for refeeding syndrome: systematic review. Nutrition 2024 Dec. PMID 39317131
- Zhang S et al. Intermittent vs. continuous enteral nutrition in critically ill patients: updated systematic review and meta-analysis, 2026. Front Nutr 2026. PMID 42095216
This is a shared conversation. Sign in to Orris to start your own chat.