New guidelines for ppi and other anti acidity drugs
Reading File
Searching PubMed
proton pump inhibitor guidelines recommendations
Searching the Web
new guidelines PPI proton pump inhibitors antacids 2024 2025 2026
Reading Article
PMID: 39692638
Reading Article
PMID: 37698821
Reading Article
PMID: 39007578
Reading Article
PMID: 39626064
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12471631
Finding Sources
Searching PubMed
vonoprazan PCAB potassium competitive acid blocker
Searching PubMed
PPI deprescribing adverse effects long-term
Reading Article
PMID: 39269391
Finding Sources
Reading File
Reading File
I now have comprehensive material to write a detailed, well-structured answer. Here it is:
New Guidelines: PPIs and Anti-Acidity Drugs (2023-2025)
This is a fast-evolving area with several major guidelines published in the last two years. Below is an organized synthesis.
1. The Drug Classes at a Glance
| Class | Examples | Mechanism | Acid Suppression |
|---|---|---|---|
| PPIs | Omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole, dexlansoprazole | Irreversibly blocks H+/K+-ATPase (proton pump) | 80-95% of basal + stimulated acid |
| P-CABs (new) | Vonoprazan (Voquezna), tegoprazan | Competitively blocks K+ binding to proton pump | Faster onset, less pH-dependent |
| H2 Blockers | Famotidine, cimetidine | Block histamine H2 receptors on parietal cells | Moderate (~70%), tolerance develops |
| Antacids | Mg(OH)2, Al(OH)3, CaCO3 | Neutralize acid in lumen | Short-acting, symptomatic only |
| Alginates | Gaviscon | Form a raft above stomach contents | Primarily anti-reflux, not acid-reducing |
2. GERD - ASGE 2025 Guideline (PMID 39692638)
The American Society for Gastrointestinal Endoscopy released an updated GERD guideline in February 2025:
Key recommendations:
- Always start with lifestyle modifications (weight loss, head-of-bed elevation, dietary changes) before or alongside drug therapy.
- PPIs remain first-line medical management for symptomatic, confirmed GERD with predominant heartburn. Use at the lowest effective dose for the shortest duration possible.
- Upper endoscopy is indicated for alarm symptoms, multiple Barrett's esophagus risk factors, or history of sleeve gastrectomy.
- In patients with small hiatal hernias (≤2 cm, Hill grade I-II), transoral incisionless fundoplication (TIF) is suggested as an alternative to chronic PPI use.
- In patients with large hiatal hernias (>2 cm, Hill grade III-IV) and persistent GERD, surgical therapy or combined TIF (cTIF) is recommended over indefinite PPI continuation.
- The message is clear: PPIs should not default to lifelong therapy - the appropriateness of continued use must be re-evaluated regularly.
3. H. pylori Eradication - ACG 2024 Guideline (PMID 39626064)
The American College of Gastroenterology updated its H. pylori treatment guideline in 2024:
Key changes from prior guidance:
- Bismuth quadruple therapy (BQT) x 14 days is now the preferred empiric first-line regimen when antibiotic susceptibility is unknown (replaces the older clarithromycin triple therapy as first-line).
- Rifabutin triple therapy or P-CAB dual therapy (vonoprazan + amoxicillin) x 14 days are suitable alternatives in patients without penicillin allergy.
- Clarithromycin- and levofloxacin-based regimens should only be used with confirmed antibiotic susceptibility.
- Universal post-treatment test-of-cure is now recommended for all patients.
- PPIs remain integral to all eradication regimens, but P-CABs are increasingly preferred as the acid suppressant component (see Section 5 below).
4. Stress Ulcer Prophylaxis in ICU - SCCM/ASHP 2024 Guideline (PMID 39007578)
Key recommendations:
- Stress ulcer prophylaxis (SUP) is recommended only for critically ill adults with specific risk factors: coagulopathy, shock, or chronic liver disease. Mechanical ventilation alone is no longer considered sufficient indication.
- Either PPIs or H2 blockers at low doses are acceptable for SUP - there is no strong evidence favoring one over the other.
- Enteral nutrition likely reduces gastrointestinal bleeding risk and should be initiated when feasible.
- Prophylaxis must be discontinued when the critical illness resolves or the risk factor is no longer present, and certainly before ICU transfer. This addresses the major problem of inappropriate PPI continuation after discharge.
5. P-CABs (Vonoprazan) - AGA 2024 Clinical Practice Update (PMID 39269391)
Potassium-competitive acid blockers (P-CABs) are a major new drug class. Vonoprazan (FDA-approved 2023 for H. pylori and erosive esophagitis) is the only P-CAB currently available in the US. The AGA issued a clinical practice update in November 2024:
Why P-CABs are different from PPIs:
- Act faster (acid suppression within hours vs. days for PPIs)
- Not prodrugs - no need for acid activation, so food timing matters less
- Efficacy is less dependent on CYP2C19 genotype
- Potent, more consistent intragastric pH control
AGA Best Practice Advice (2024):
| Indication | P-CAB Recommendation |
|---|---|
| Uninvestigated heartburn / NERD | Do not use P-CABs first-line |
| Mild erosive esophagitis (LA A/B) | Do not use P-CABs first-line; use if failing twice-daily PPIs |
| Severe erosive esophagitis (LA C/D) | P-CABs are a reasonable option for healing and maintenance |
| H. pylori eradication | Use P-CABs in place of PPIs in eradication regimens |
| Peptic ulcer disease (treatment/prophylaxis) | Do not use P-CABs first-line |
| Bleeding gastroduodenal ulcers | Insufficient evidence; rapid acid suppression is theoretically useful |
- Cost caveat: Even modest clinical superiority of P-CABs over double-dose PPIs may not make them cost-effective as first-line therapy at current US pricing.
6. PPI Stewardship - Indian Society of Gastroenterology 2023 (PMID 37698821)
This guideline formalizes the concept of PPI stewardship, addressing widespread overuse:
Appropriate indications for PPI use:
- GERD and erosive esophagitis
- Peptic ulcer disease (H. pylori eradication; NSAID-related ulcers)
- Zollinger-Ellison syndrome
- Upper GI bleeding (acute and prevention in high-risk patients on antithrombotics)
- Eosinophilic esophagitis
- Stress ulcer prophylaxis (in high-risk ICU patients only)
- Barrett's esophagus chemoprevention
Inappropriate/questionable uses to avoid:
- Routine co-prescription with all antibiotics or corticosteroids (without GI risk factors)
- Non-specific abdominal pain without acid-peptic workup
- Nausea, vomiting without established acid-peptic etiology
- Prophylaxis in low-risk hospitalized patients
7. Long-Term PPI Safety Concerns and Deprescribing
Modern guidelines (NICE, ACG, STOPP/START criteria, Beers Criteria) now emphasize structured deprescribing:
Recognized risks with prolonged PPI use:
- Hypomagnesemia and hypokalemia (especially >1 year)
- Vitamin B12 and iron malabsorption
- Increased risk of Clostridioides difficile infection
- Community-acquired pneumonia (modest association)
- Osteoporosis/fracture risk (particularly hip fracture in older adults)
- Rebound acid hypersecrerity upon abrupt discontinuation (2-4 weeks)
- Potential increased risk of CKD (association data, causality debated)
Conditions where PPIs should NOT be deprescribed:
- Barrett's esophagus
- Severe erosive esophagitis (LA grade C/D)
- Zollinger-Ellison syndrome
- Documented recurrent GI ulcer/bleeding
- Eosinophilic esophagitis with confirmed PPI response
Deprescribing approach:
- Assess whether the original indication still applies
- If it does not, trial dose reduction or discontinuation
- Options: dose halving, on-demand therapy, or switch to H2 blocker/antacid
- Warn patients about rebound heartburn (2-4 weeks) and provide management strategies
- Follow up at 4-12 weeks and reassess
- Structured programmes achieve up to 86% discontinuation success vs. historical rates of 30-60%
8. Pharmacology Notes Relevant to Prescribing
- Take PPIs 30-60 min before the first meal of the day for optimal efficacy (H+/K+-ATPase is most active when parietal cells are stimulated) - Goodman & Gilman's, 15th Ed.
- CYP2C19 polymorphisms affect first-generation PPI efficacy (omeprazole, lansoprazole, pantoprazole). Rabeprazole and esomeprazole are less affected by CYP2C19 genotype. P-CABs sidestep this issue entirely. - Yamada's Textbook of Gastroenterology, 7th Ed.
- PPIs + clopidogrel: Use caution. Omeprazole (a CYP2C19 inhibitor) reduces clopidogrel antiplatelet efficacy. Pantoprazole or rabeprazole are preferred if a PPI is needed alongside clopidogrel. - Goodman & Gilman's
- Rebound hypersecretion after PPI withdrawal is mediated by upregulation of H+/K+-ATPase during therapy. Gradual tapering is preferred over abrupt cessation.
Summary Table: When to Use What
| Condition | First-Line Drug | Alternative / Notes |
|---|---|---|
| GERD (symptomatic) | PPI (lowest dose, shortest duration) | Lifestyle changes first; TIF if eligible |
| Erosive esophagitis (LA A/B) | PPI | P-CAB if PPI-refractory |
| Erosive esophagitis (LA C/D) | PPI or P-CAB | P-CAB preferred for maintenance |
| H. pylori (treatment-naive) | Bismuth quadruple therapy x14d (PPI or P-CAB) | P-CAB dual therapy alternative |
| NSAID-related ulcer prevention | PPI | Misoprostol alternative |
| Stress ulcer prophylaxis (ICU, high-risk only) | PPI or H2 blocker (low dose) | Discontinue when risk resolved |
| Zollinger-Ellison | High-dose PPI | Titrate to achieve acid control |
| Functional dyspepsia | PPI (short course only) | H2 blockers; reassess if no response |
| Non-specific indigestion/antacid use | Antacid or alginate (OTC) | Do not initiate PPI empirically |
Key references:
- ASGE GERD Guideline 2025 - PMID 39692638
- ACG H. pylori Guideline 2024 - PMID 39626064
- SCCM/ASHP Stress Ulcer Prophylaxis Guideline 2024 - PMID 39007578
- AGA P-CAB Clinical Practice Update 2024 - PMID 39269391
- ISG PPI Stewardship Guidelines 2023 - PMID 37698821
- Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed. - Chapter 53
- Yamada's Textbook of Gastroenterology, 7th Ed. - PPI pharmacology
Dopamine-prolactin interaction and regulation
Reading File
Searching PubMed
dopamine prolactin regulation tuberoinfundibular
Searching the Web
dopamine prolactin interaction regulation tuberoinfundibular neurons D2 receptor 2024
Finding Sources
Finding Sources
Reading Article
PMID: 38203281
Reading Article
PMID: 38396659
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here it is:
Dopamine-Prolactin Interaction and Regulation
1. The Core Concept: Dopamine as the Prolactin Inhibitory Factor (PIF)
Prolactin is unique among pituitary hormones in that it is under tonic inhibitory control rather than stimulatory control from the hypothalamus. Dopamine - acting as the Prolactin Inhibitory Factor (PIF) - continuously suppresses prolactin secretion. Remove the dopamine signal and prolactin rises. This is the opposite of all other anterior pituitary hormones, which require a releasing hormone from the hypothalamus.
"Unlike other hormones secreted by the hypothalamus, which stimulate the release of pituitary hormones, dopamine released from the hypothalamus actually inhibits the release of prolactin from lactotrophic cells of the anterior pituitary." - Adams and Victor's Principles of Neurology, 12th Ed.
2. Anatomy of the Pathway: Tuberoinfundibular Dopaminergic (TIDA) Neurons
The pathway has three anatomical segments:
Arcuate nucleus (mediobasal hypothalamus)
|
↓ (axon projection)
External zone of the MEDIAN EMINENCE
|
↓ (dopamine secreted into portal blood)
HYPOPHYSEAL PORTAL VASCULATURE
|
↓ (carried to anterior pituitary)
D2 RECEPTORS on LACTOTROPHS (anterior pituitary)
|
↓ (inhibition of prolactin synthesis + secretion)
↓ PROLACTIN RELEASE
TIDA neurons (Tuberoinfundibular Dopaminergic neurons):
- Cell bodies in the arcuate nucleus of the mediobasal hypothalamus
- Project to the external zone of the median eminence (NOT the posterior pituitary)
- Dopamine released there enters the hypophyseal portal capillaries - a short, specialized portal blood system connecting hypothalamus to anterior pituitary
- Dopamine binds D2 receptors on lactotrophs → inhibits prolactin release
This pathway is distinct from the nigrostriatal (movement), mesolimbic (reward), and mesocortical (cognition) dopamine pathways. - Stahl's Essential Psychopharmacology, Neuroscientific Basis
Tuberoinfundibular dopamine pathway: hypothalamus → median eminence → portal blood → anterior pituitary D2 receptors. (Stahl's Essential Psychopharmacology)
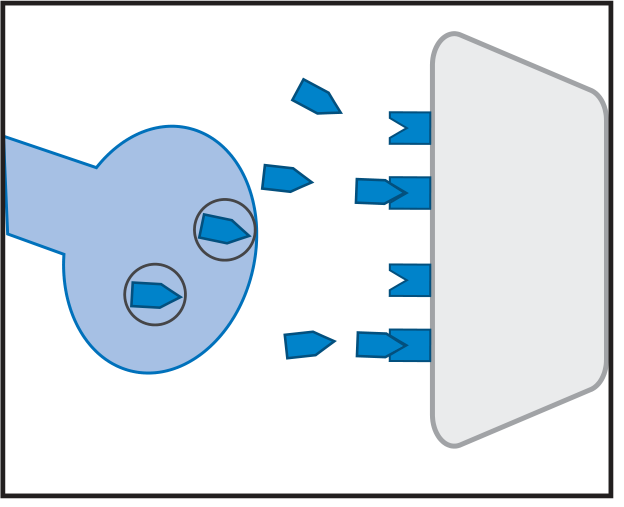
3. Molecular Mechanism at the Lactotroph
The lactotroph membrane carries both D2 receptors (inhibitory) and 5-HT2A receptors (stimulatory):
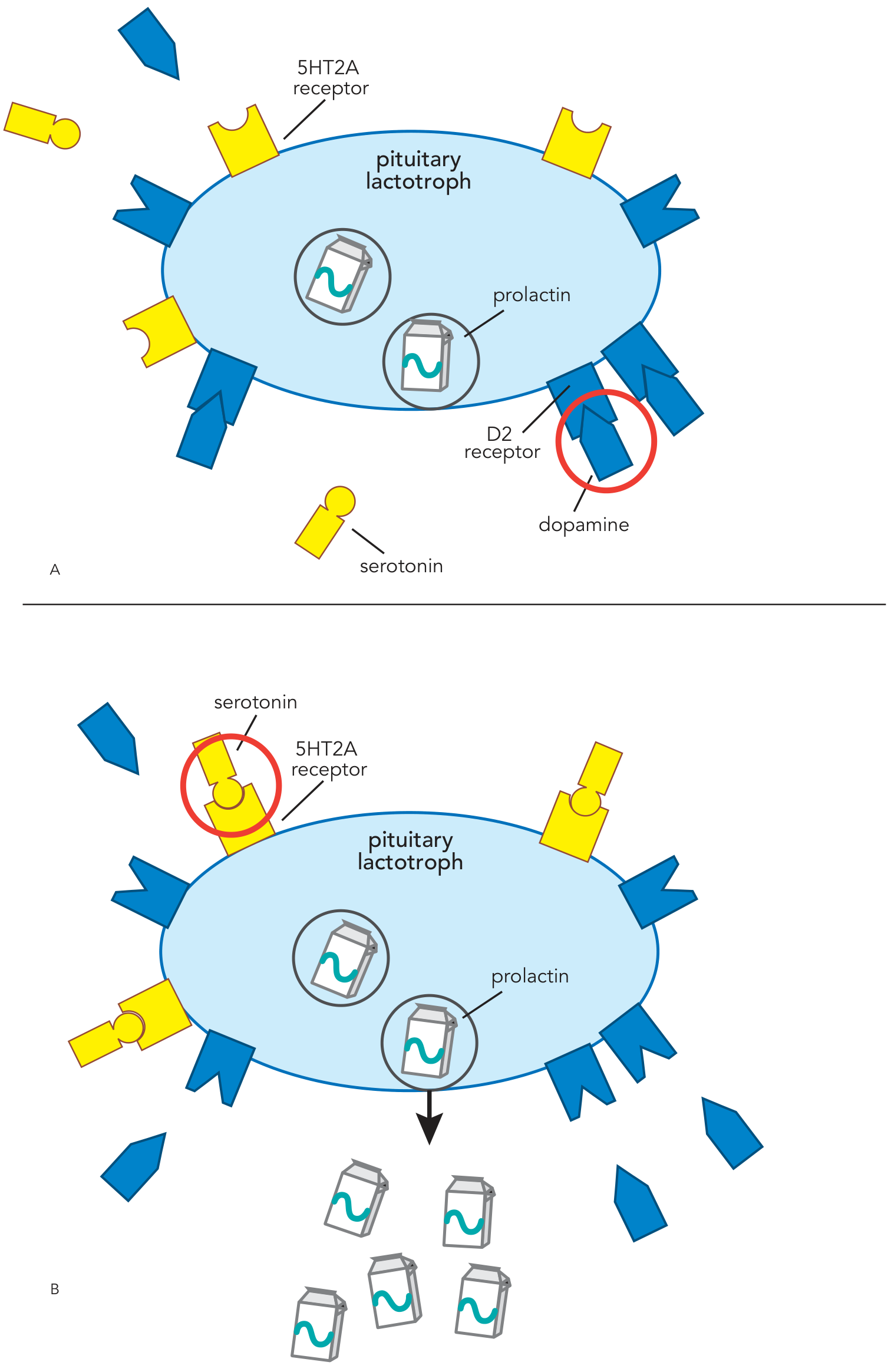
Panel A: Dopamine binding D2 receptors (red circle) suppresses prolactin release. Panel B: Serotonin binding 5-HT2A receptors stimulates prolactin release - the two systems are reciprocal. (Stahl's Essential Psychopharmacology)
At the D2 receptor:
- D2 receptor is a Gi-coupled GPCR
- Activation → inhibition of adenylyl cyclase → ↓cAMP → ↓protein kinase A activity → reduced prolactin gene transcription and exocytosis
- Both D2L (long isoform) and D2S (short isoform) are expressed on lactotrophs
4. Prolactin's Feedback Loop on Dopamine
Prolactin exerts a short-loop negative feedback on its own secretion by acting back on TIDA neurons:
- Elevated prolactin → stimulates TIDA neurons in the arcuate nucleus → more dopamine released → suppresses its own secretion
- This is mediated through prolactin receptors (PRL-R) expressed on TIDA neurons
- It explains why prolactin levels are normally tightly regulated
"Prolactin also inhibits its secretion using a short-loop feedback circuit to the hypothalamus." - Kaplan & Sadock's Synopsis of Psychiatry
A 2025 study showed that prolactin regulates TIDA neurons through distinct time-course mechanisms - early effects via rapid phosphorylation of tyrosine hydroxylase (TH, the rate-limiting enzyme in dopamine synthesis) and delayed effects through upregulation of TH gene expression. (PMID: 38203281)
5. Factors That Regulate Prolactin Secretion
Inhibitors of Prolactin (reduce prolactin)
| Factor | Mechanism |
|---|---|
| Dopamine | D2 receptor activation on lactotrophs (main inhibitor) |
| Dopamine agonists (bromocriptine, cabergoline) | Mimic dopamine at D2 receptors |
Stimulators of Prolactin (raise prolactin)
| Factor | Mechanism |
|---|---|
| Suckling / nipple stimulation | Sensory signals via spinal cord → inhibit TIDA neurons |
| Estrogen | Stimulates PRL transcription directly; also promotes serotonin-mediated PRL release; causes lactotroph proliferation |
| TRH (Thyrotropin-Releasing Hormone) | Directly stimulates lactotrophs |
| VIP (Vasoactive Intestinal Peptide) | Directly stimulates prolactin release |
| Serotonin (5-HT) | Via 5-HT2A and 5-HT3 receptors on lactotrophs |
| Opioids | Indirect - suppress dopamine release from TIDA neurons |
| Stress | Via hypothalamic mechanisms |
| Sleep | Prolactin secretion is highest in early morning (nocturnal rise) |
| Pregnancy | Rising estrogen drives massive lactotroph proliferation; PRL peaks at delivery (20-500 pg/mL) |
| Oxytocin | Contributes to suckling-stimulated release |
| Norepinephrine, histamine, glutamate, CRH | Modulating roles |
From Goldman-Cecil Medicine, 26th Ed: "Thyrotropin-releasing hormone (TRH) and vasoactive intestinal peptide (VIP) also stimulate the release of prolactin, so when hypothyroidism increases TRH release, it causes hyperprolactinemia."
6. Normal Prolactin Values and Physiological Range
| State | PRL Level |
|---|---|
| Normal (women) | 5-25 ng/mL (or pg/mL) |
| Normal (men) | 10-15 ng/mL |
| Pregnancy | Up to 500 ng/mL |
| Microprolactinoma | 20-250 ng/mL |
| Macroprolactinoma | >200 ng/mL (often >1000) |
Values >250 µg/L almost always indicate a macroprolactinoma - Harrison's Principles of Internal Medicine, 22nd Ed (2025)
7. Causes of Hyperprolactinemia: The "Dopamine Disruption" Framework
All causes of hyperprolactinemia can be understood as either:
- Blocking dopamine's action on the lactotroph
- Reducing dopamine delivery to the pituitary
- Autonomous prolactin production by a tumor
| Category | Examples | Mechanism | PRL Range |
|---|---|---|---|
| Antipsychotics (1st gen) | Haloperidol, fluphenazine | D2 receptor blockade | 20-70 ng/mL |
| Antipsychotics (2nd gen) | Risperidone, paliperidone | D2 blockade | 20-70 ng/mL |
| Antiemetics | Metoclopramide, domperidone, prochlorperazine | D2 blockade | Elevated |
| Antidepressants | Clomipramine | Uncertain | 20-70 |
| Opioids | Methadone, morphine | Inhibit TIDA neurons | 20-70 |
| Estrogens | OCP | Transcriptional stimulation | 20-70 |
| Stalk compression | Non-secreting pituitary adenoma, meningioma | Prevents dopamine from reaching pituitary | <100 |
| Hypothyroidism | Primary hypothyroidism | ↑TRH stimulates lactotrophs | <100 |
| Chronic renal failure/cirrhosis | Reduced PRL clearance | <100 | |
| Prolactinoma | Microadenoma / Macroadenoma | Autonomous secretion | 20 - >10,000 |
| Chest wall injury | Surgery, herpes zoster | Mimics suckling pathway | 20-70 |
| Stress, exercise | Hypothalamic | 20-70 |
From Goldman-Cecil Medicine, Table 205-8
Key clinical pearl on stalk compression ("stalk effect"): When a non-prolactin-secreting mass compresses the pituitary stalk, dopamine cannot travel down to the pituitary. The lactotrophs, deprived of their tonic inhibition, release prolactin freely. PRL levels are typically <100-150 ng/mL in stalk-compression hyperprolactinemia - a useful distinguisher from macroprolactinoma (typically >200-250 ng/mL).
8. Clinical Consequences of Disrupting Dopamine-Prolactin Balance
Hyperprolactinemia Effects
- Galactorrhea - inappropriate lactation (men and women)
- Amenorrhea / oligomenorrhea - PRL suppresses GnRH pulsatility → ↓LH/FSH → anovulation
- Infertility (women and men)
- Hypogonadism - ↓testosterone in men → loss of libido, erectile dysfunction
- Osteoporosis - via hypogonadism, especially in postmenopausal women not on estrogen
- Gynecomastia (men)
- Psychiatric symptoms - depression, anxiety, decreased libido, stress intolerance (PMID: 38396659)
Connection to Antipsychotic Side Effects
When D2-blocking antipsychotics (e.g., haloperidol, risperidone) are used, they block D2 receptors in the TIDA pathway just as in the mesolimbic pathway, causing drug-induced hyperprolactinemia. Second-generation ("atypical") antipsychotics that combine D2 blockade with 5-HT2A blockade (e.g., quetiapine, clozapine, olanzapine) cause less hyperprolactinemia because blocking 5-HT2A prevents serotonin from stimulating prolactin release - partially compensating for the loss of dopaminergic inhibition. - Stahl's Essential Psychopharmacology
9. Therapeutic Applications: Restoring Dopamine Inhibition
Dopamine Agonists (D2 agonists)
| Drug | Dose | Notes |
|---|---|---|
| Cabergoline | 0.5-1.0 mg twice weekly | Long-acting, high D2 affinity, >14-day effect; normalizes PRL in ~80% of patients; preferred agent |
| Bromocriptine | 2.5-7.5 mg/day in divided doses | Semisynthetic ergot alkaloid; older agent; shorter half-life; reference standard |
Mechanism: Both act as D2 agonists on lactotrophs → mimic dopamine → suppress PRL synthesis, secretion, and lactotroph/prolactinoma cell proliferation (tumor shrinkage)
Clinical use:
- Microprolactinomas: first-line treatment; drug may be withdrawn after 2 years if normoprolactinemia achieved and tumor significantly reduced
- Macroprolactinomas: first-line even for large tumors; cabergoline can achieve substantial tumor shrinkage
- Drug-induced hyperprolactinemia: discontinue offending drug if possible; if antipsychotic cannot be stopped, add cabergoline with caution (may worsen psychosis)
- Hypothyroid-induced: thyroid hormone replacement resolves hyperprolactinemia
10. Summary Diagram (Conceptual)
STRESS / SUCKLING / ESTROGEN / TRH / VIP / SEROTONIN
↓ (stimulate)
HYPOTHALAMUS
- TIDA neurons (arcuate nucleus)
- Release DOPAMINE into portal blood
↓ (inhibit) ← PRL short-loop feedback also stimulates TIDA
ANTERIOR PITUITARY LACTOTROPH
- D2 receptor (Gi) → ↓ cAMP → ↓ PRL
- 5HT2A receptor → ↑ PRL (reciprocal)
↓
PROLACTIN secreted into circulation
↓
TARGET ORGANS: Mammary glands, gonads, behavior, immune cells
Disruption points:
- D2 blockers (antipsychotics, antiemetics) → ↑ PRL
- Stalk compression → ↑ PRL (dopamine can't reach pituitary)
- Prolactinoma → autonomous ↑↑ PRL
- Treatment: D2 agonists (cabergoline/bromocriptine) → ↓ PRL
Key Sources:
- Adams and Victor's Principles of Neurology, 12th Ed. - Prolactin Inhibition chapter
- Stahl's Essential Psychopharmacology, Neuroscientific Basis - TIDA pathway and D2 pharmacology
- Kaplan & Sadock's Synopsis of Psychiatry - Prolactin as index of dopamine activity
- Harrison's Principles of Internal Medicine, 22nd Ed (2025) - Hyperprolactinemia and Prolactinoma
- Goldman-Cecil Medicine, 26th Ed. - Causes table and regulation
- Qi-Lytle X et al. "Current Review of the Function and Regulation of Tuberoinfundibular Dopamine Neurons." IJMS 2024 (PMID: 38203281)
- Szukiewicz D. "Current Insights in Prolactin Signaling and Ovulatory Function." IJMS 2024 (PMID: 38396659)
This is a shared conversation. Sign in to Orris to start your own chat.