Preclamsia and eclampsia in detail and easy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed, easy-to-understand answer.
Preeclampsia and Eclampsia - Complete Guide
What Are They? (Simple Overview)
Preeclampsia is a pregnancy-specific disorder that develops after 20 weeks of gestation, characterized by high blood pressure + protein in urine (or signs of organ damage). It affects about 3-8% of pregnancies.
Eclampsia is preeclampsia that has progressed to seizures (grand mal convulsions) - it is the more dangerous, advanced form.
Think of it this way:
Preeclampsia = high BP + organ stress in pregnancy Eclampsia = preeclampsia + seizures
The Core Problem - What Goes Wrong?
The root cause starts in the placenta, specifically in how blood vessels form. Here is what happens step by step:
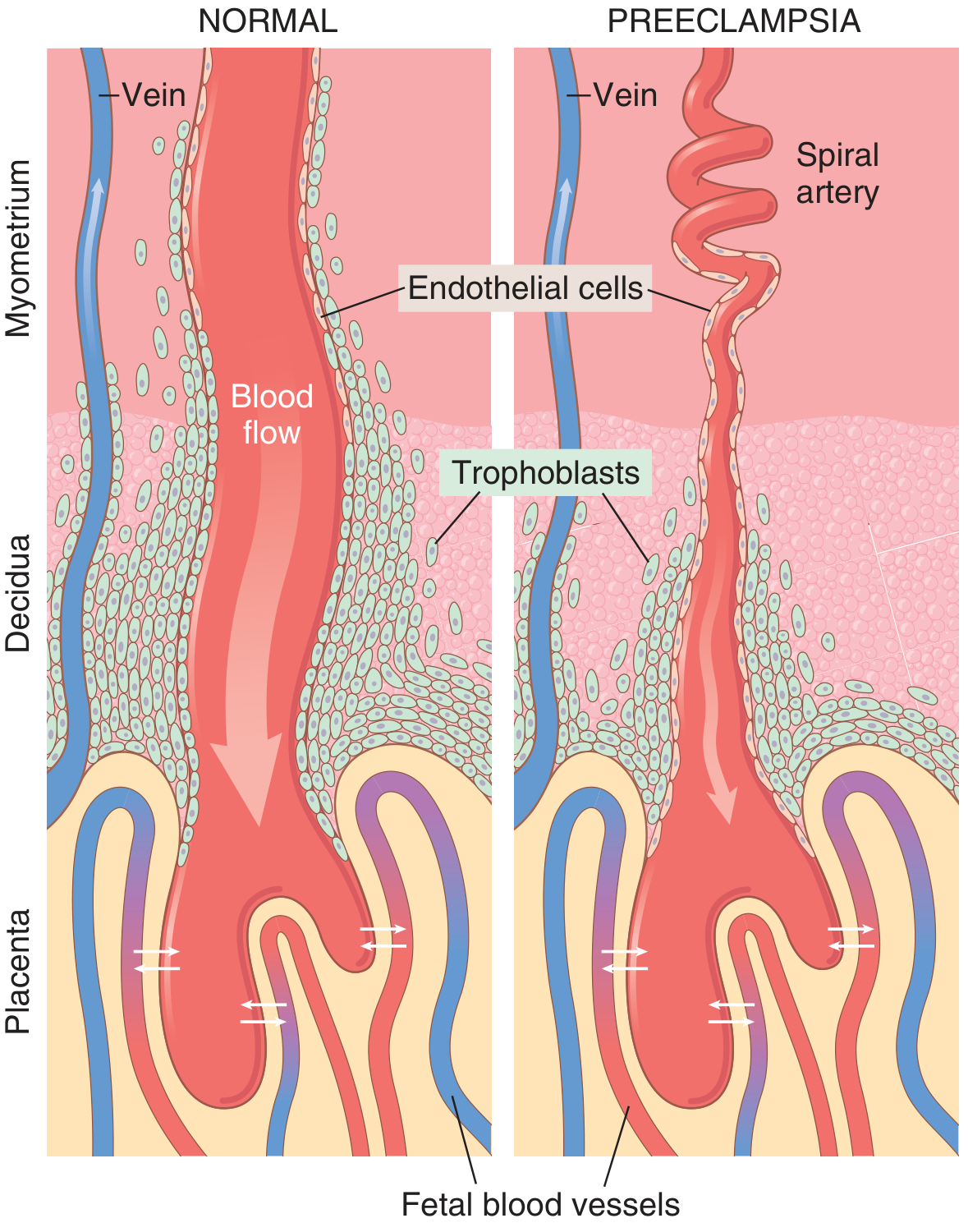
Left (Normal): Trophoblasts invade and widen the spiral arteries into low-resistance, high-flow channels. Right (Preeclampsia): Trophoblasts fail to invade - arteries stay narrow and coiled, causing placental ischemia.
Step-by-Step Pathophysiology
Normal pregnancy:
Trophoblasts (placental cells) invade spiral arteries
→ Arteries widen into large, low-resistance sinusoids
→ Plenty of blood to the placenta and baby
Preeclampsia:
Trophoblast invasion FAILS
→ Spiral arteries stay narrow and coiled
→ Placenta becomes ischemic (oxygen-starved)
→ Placenta releases dangerous factors into mother's blood
→ Widespread maternal endothelial dysfunction
→ High BP + Proteinuria + Organ damage
Key Molecules Released by the Ischemic Placenta
| Factor | Effect |
|---|---|
| sFlt-1 (soluble fms-like tyrosine kinase-1) | Blocks VEGF (vessel growth factor) - causes endothelial damage |
| Soluble endoglin | Blocks TGF-β - worsens endothelial dysfunction |
| ↓ Prostacyclin (PGI₂) | Less vasodilation |
| ↑ Thromboxane A₂ | More vasoconstriction - raises BP |
| Inflammatory cytokines (TNF-α, IL-6) | Systemic inflammation |
The result: blood vessels throughout the mother's body become dysfunctional - they constrict, leak protein, and form microclots.
- Creasy & Resnik's Maternal-Fetal Medicine
- Robbins & Kumar Basic Pathology, p. 702
- Guyton & Hall Textbook of Medical Physiology, p. 1041
Risk Factors
| Category | Examples |
|---|---|
| Obstetric | First pregnancy (nulliparity - accounts for 32% of cases), prior preeclampsia, multiple gestation (twins), molar pregnancy |
| Medical | Chronic hypertension (25% risk), diabetes mellitus (20% overall, up to 70% with severe diabetic disease), chronic renal failure, SLE, antiphospholipid syndrome |
| Demographic | Extremes of age, Black race (associated with more severe forms), IVF pregnancy |
| Family history | First-degree relative with preeclampsia |
Diagnosis - What to Look For
Preeclampsia Diagnostic Criteria
BP criterion:
- Systolic BP ≥ 140 mmHg OR Diastolic BP ≥ 90 mmHg
- Measured on two occasions at least 4 hours apart
- After 20 weeks of gestation
PLUS one of:
- Proteinuria > 300 mg in 24 hours (or urine protein:creatinine ratio ≥ 0.3)
- OR signs of end-organ damage (even without proteinuria):
- Thrombocytopenia (platelets < 100,000)
- Renal insufficiency (creatinine > 1.1 mg/dL)
- Impaired liver function (elevated transaminases)
- Pulmonary edema
- New-onset headache unresponsive to medication
- Visual disturbances
Preeclampsia WITH Severe Features
Any of the following upgrades the diagnosis:
- BP ≥ 160/110 mmHg (on two occasions 15 minutes apart)
- Platelet count < 100,000/µL
- Serum creatinine > 1.1 mg/dL
- Doubling of liver enzymes
- Pulmonary edema
- Severe headache, visual changes, or clonus
Eclampsia
-
New-onset grand mal (tonic-clonic) seizures in a woman with preeclampsia
-
No other neurological cause to explain the seizure
-
Can occur antepartum, intrapartum, or postpartum (up to 10 days after delivery)
-
Progression from preeclampsia to eclampsia is unpredictable and can be rapid
-
ROSEN's Emergency Medicine, p. 2668-2670
-
Tintinalli's Emergency Medicine, p. 443
Symptoms - What the Patient Feels
Early/Mild Preeclampsia
- High blood pressure (may be asymptomatic)
- Swelling (edema) - especially face and hands
- Rapid weight gain (fluid retention)
- Protein in urine (no symptoms, detected on testing)
Severe Preeclampsia / Warning Signs of Eclampsia
- Severe headache (frontal, persistent, not responding to paracetamol)
- Visual disturbances - blurred vision, flashing lights, scotomata (blind spots)
- Right upper quadrant / epigastric pain (liver capsule distension)
- Nausea and vomiting
- Decreased urine output
- Brisk reflexes, clonus
Eclampsia
- Seizures (tonic-clonic) - may occur without warning
- Confusion, altered consciousness post-seizure
- Can lead to coma
Organs Affected (End-Organ Damage)
| Organ | What Happens |
|---|---|
| Kidney | Glomerular endotheliosis - thickened basement membranes, decreased GFR, proteinuria |
| Brain | Vasospasm, cerebral edema, PRES (posterior reversible encephalopathy syndrome), seizures, hemorrhage |
| Liver | Periportal hemorrhage, elevated enzymes, capsular distension (pain), rupture in severe cases |
| Placenta | Infarcts, retroplacental hemorrhage, placental abruption, IUGR (intrauterine growth restriction) |
| Blood | Thrombocytopenia, DIC, microangiopathic hemolytic anemia |
| Eye | Retinal arteriolar spasm, retinal detachment, visual disturbances |
HELLP Syndrome
A severe complication occurring in ~10% of severe preeclampsia cases:
H - Hemolysis (microangiopathic hemolytic anemia) EL - Elevated Liver enzymes LP - Low Platelets
HELLP is a medical emergency. It carries risk for:
-
DIC (disseminated intravascular coagulation)
-
Liver rupture
-
Placental abruption
-
Maternal/fetal death
-
Robbins & Kumar Basic Pathology, p. 702
Pathology (What You See Under the Microscope)
Placenta
- Multiple infarcts (much more numerous than normal pregnancy)
- Retroplacental hemorrhage
- Syncytial knots (aggregates of syncytial nuclei on villi - sign of ischemia)
- Acute atherosis in decidual vessels - fibrinoid necrosis + lipid-laden macrophages (resembles atherosclerosis)
Kidney
-
Glomerular endotheliosis - swollen endothelial cells, obliterated capillary lumens
-
Protein deposits in glomerular basement membranes
-
Decreased GFR (opposite to normal pregnancy where GFR increases)
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
Management
The Definitive Treatment: DELIVERY
The only cure is delivery of the placenta. All other treatments are supportive.
The timing decision balances:
- Maternal risk of continuing pregnancy vs.
- Fetal risk of preterm delivery
General rules:
- ≥ 37 weeks + preeclampsia → deliver
- ≥ 34 weeks + severe features → deliver
- < 34 weeks without severe features → expectant management with close monitoring
1. Antihypertensive Therapy
Threshold for treatment: BP ≥ 160/110 mmHg (must treat urgently - risk of intracranial hemorrhage)
| Drug | Dose | Notes |
|---|---|---|
| Labetalol (1st line) | 20 mg IV, then doubled doses up to 80 mg | Alpha + beta blocker; safe in pregnancy |
| Hydralazine | 10 mg IV bolus | Effective; may cause reflex tachycardia |
| Nifedipine (oral) | 10-20 mg orally | Good for outpatient/expectant management |
| Nicardipine | 5-15 mg/hour IV | Potent alternative |
| Methyldopa | Oral | Good for chronic management |
Avoid: ACE inhibitors, ARBs (harmful to fetus)
2. Seizure Prevention and Treatment: Magnesium Sulfate
Magnesium sulfate is the first-line drug for both seizure prophylaxis and treatment in preeclampsia/eclampsia.
Dose:
- Loading: 4 g IV over 15-20 minutes
- Maintenance: 1-2 g/hour IV infusion
How it works:
- Calcium antagonism → smooth muscle relaxation
- Reduces cerebral vasospasm
- Protects blood-brain barrier → limits cerebral edema
- Central anticonvulsant activity
Monitoring for toxicity:
- Respiratory rate (respiratory depression is the major risk)
- Oxygen saturation
- Deep tendon reflexes (loss of patellar reflex is early warning)
- Urine output (magnesium is renally cleared)
Antidote for magnesium toxicity: Calcium gluconate 1g IV
Who gets magnesium? Women with severe features, especially:
- Clonus
- Severe headache
- Visual disturbances (scotomata)
3. Fluid Management
Preeclampsia is a volume-contracted, NOT volume-depleted state. The key point:
- Capillary permeability is increased
- Do NOT give aggressive IV fluids - high risk of pulmonary edema
- Restrict IV fluids to ~85 mL/hour in severe cases
4. Management of Eclamptic Seizure
| Step | Action |
|---|---|
| Airway | Position, suction, oxygen |
| Stop the seizure | MgSO₄ 4g IV (if not already on it); diazepam as backup |
| Blood pressure | Treat if ≥ 160/110 mmHg |
| Fetal monitoring | Continuous CTG monitoring |
| Delivery | Plan after maternal stabilization |
- Comprehensive Clinical Nephrology, 7th Edition, p. 632
- ROSEN's Emergency Medicine, p. 2670
Prognosis and Recovery
- After delivery: Hypertension and proteinuria usually resolve within 1-2 weeks
- Most women have no lasting sequelae after uncomplicated preeclampsia
- Preeclampsia increases lifelong cardiovascular risk (hypertension, ischemic heart disease, stroke) in the mother
- Risk of recurrence in future pregnancies: ~15-25% (higher if early onset or severe)
Prevention
| Strategy | Benefit |
|---|---|
| Low-dose aspirin (75-150 mg/day) starting at 12-16 weeks | Reduces risk by ~10-20% in high-risk women (recommended by ACOG/NICE) |
| Calcium supplementation (in calcium-deficient populations) | Some protective effect |
| Early prenatal care | Early detection of risk factors |
Quick Summary Table
| Feature | Preeclampsia | Eclampsia |
|---|---|---|
| Definition | HTN + proteinuria/organ damage after 20 wks | Preeclampsia + seizures |
| BP | ≥ 140/90 mmHg | ≥ 140/90 mmHg (usually higher) |
| Seizures | No | Yes (grand mal) |
| Incidence | 3-8% of pregnancies | < 1% |
| Core treatment | Antihypertensives + MgSO₄ + delivery | MgSO₄ + BP control + urgent delivery |
| Definitive cure | Delivery | Delivery |
Sources: Creasy & Resnik's Maternal-Fetal Medicine | Robbins & Kumar Basic Pathology | Guyton & Hall Medical Physiology, p. 1041 | ROSEN's Emergency Medicine | Tintinalli's Emergency Medicine | Comprehensive Clinical Nephrology, 7th Ed.
Its for obgy
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
This is a real clinical photo from Creasy & Resnik showing a woman during and after an eclamptic seizure (A: during postictal state, B: after recovery with facial edema). I now have everything needed. Here is the full, OB/GYN-focused answer:
Preeclampsia & Eclampsia - OB/GYN Complete Notes
BASIC CONCEPT (Easy Understand)
| Term | Simple Definition |
|---|---|
| Preeclampsia | High BP + proteinuria (or organ damage) appearing after 20 weeks of pregnancy |
| Eclampsia | Preeclampsia that progresses to grand mal seizures |
| HELLP syndrome | Severe variant: Hemolysis + Elevated Liver enzymes + Low Platelets |
These are pregnancy-specific diseases. They completely reverse after delivery. The placenta is the cause, delivery is the cure.
PATHOPHYSIOLOGY (The "Why")
The Key Problem: Failure of Spiral Artery Remodeling
In normal pregnancy (left), trophoblasts invade and dilate spiral arteries into wide, low-resistance sinusoids. In preeclampsia (right), this invasion fails - arteries stay narrow and coiled, causing placental ischemia.
Step-by-step mechanism:
1. Trophoblast invasion of spiral arteries FAILS
↓
2. Spiral arteries remain narrow and coiled
↓
3. Placenta becomes ischemic (underperfused)
↓
4. Ischemic placenta releases antiangiogenic factors into maternal blood:
- sFlt-1 (soluble fms-like tyrosine kinase-1) → blocks VEGF and PIGF
- Soluble endoglin → blocks TGF-β
↓
5. Widespread MATERNAL ENDOTHELIAL DYSFUNCTION
↓
6. Signs and symptoms of preeclampsia:
- ↑ Vasoconstriction (↑ TXA₂, ↓ PGI₂) → Hypertension
- Endothelial leakage → Proteinuria, Edema
- Platelet activation → Thrombocytopenia, DIC
- Organ hypoperfusion → Liver, Kidney, Brain damage
Key mediators:
-
↓ Prostacyclin (PGI₂) and ↑ Thromboxane A₂ - imbalance causes vasoconstriction
-
sFlt-1 - the most studied marker; levels rise weeks before clinical disease
-
Increased angiotensin II sensitivity - preeclamptic women are hypersensitive to Ang II even from early pregnancy (as early as 10-14 weeks, before clinical signs!)
-
Creasy & Resnik's Maternal-Fetal Medicine
CLASSIFICATION (OB/GYN Standard)
1. Hypertensive Disorders of Pregnancy (Classification)
| Type | Definition |
|---|---|
| Chronic hypertension | HTN before 20 weeks or pre-existing |
| Gestational hypertension | New HTN ≥ 20 weeks, NO proteinuria/organ damage, resolves postpartum |
| Preeclampsia | HTN ≥ 20 weeks + proteinuria OR end-organ damage |
| Superimposed preeclampsia | Preeclampsia developing on top of chronic HTN |
| Eclampsia | Preeclampsia + seizures |
2. Preeclampsia: Without vs. With Severe Features
ACOG no longer uses the term "mild" - even without severe features, it carries risk.
Diagnostic Criteria for Preeclampsia:
BP (on 2 occasions ≥ 4 hours apart, after 20 weeks):
- Systolic ≥ 140 mmHg OR Diastolic ≥ 90 mmHg
PLUS at least ONE of:
- Proteinuria ≥ 300 mg/24 hr (or protein:creatinine ratio ≥ 0.3, or dipstick 2+)
- OR without proteinuria, any of:
- Platelets < 100,000/µL
- Creatinine > 1.1 mg/dL (new renal insufficiency)
- Liver enzymes > 2x upper limit of normal
- Pulmonary edema
- New-onset cerebral or visual disturbances
Criteria for SEVERE FEATURES:
| Feature | Threshold |
|---|---|
| Blood pressure | ≥ 160/110 mmHg on 2 occasions ≥ 4 hrs apart |
| Thrombocytopenia | Platelets < 100,000/µL |
| Liver | Enzymes > 2x normal + persistent RUQ/epigastric pain |
| Kidney | Creatinine > 1.1 mg/dL |
| Pulmonary edema | Any |
| Neurological | New headache, visual disturbances, clonus |
Note (OB exam important!): Proteinuria > 5g and fetal growth restriction are NO LONGER criteria for severe features (per current ACOG).
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1055
RISK FACTORS
| Category | Specific Risk Factors |
|---|---|
| Nulliparity | Biggest single risk - accounts for 32% of cases |
| Previous preeclampsia | 15-25% recurrence risk |
| Multiple gestation | Twins 6.7%, Triplets 12.7%, Quadruplets 20% |
| Chronic HTN | 25% risk of developing superimposed preeclampsia |
| Diabetes mellitus | ~20% overall; up to 70% with nephropathy (Class F/R) |
| Renal disease | High risk, especially with proteinuria |
| Antiphospholipid syndrome | Major risk - also causes recurrent loss |
| SLE | Increased risk; hard to distinguish from lupus flare |
| Age extremes | Very young (primigravidas) and older women |
| Black race | Associated with more severe forms |
| IVF pregnancy | Increased risk |
| Hydatidiform mole | Can present earlier than 20 weeks |
| Family history | First-degree relative with preeclampsia |
CLINICAL FEATURES
A. Symptoms (by system)
| System | Symptoms |
|---|---|
| CNS | Severe headache (frontal), dizziness, tinnitus, drowsiness, confusion |
| Visual | Blurred vision, scotomata, diplopia, photophobia, even amaurosis |
| GI/Liver | Epigastric pain, RUQ pain, nausea, vomiting, hematemesis |
| Renal | Oliguria, anuria, hematuria |
| Cardiovascular | Tachycardia, dyspnea |
Most women with early preeclampsia are asymptomatic - this is why frequent antenatal visits matter!
B. Signs
- Hypertension (hallmark)
- Edema - especially facial and hand edema (note: edema alone is NOT diagnostic; it occurs in normal pregnancy too)
- Proteinuria on urine dipstick or 24-hr collection
- Brisk deep tendon reflexes and clonus (warning sign of eclampsia)
- Papilledema (severe cases)
Eclampsia - Clinical Picture

A: Postictal state after eclamptic seizure. B: Same patient after recovery, showing classic facial edema.
-
Seizures are grand mal (tonic-clonic) type
-
Preceded by prodrome in 80%: headache, visual changes
-
30% of eclampsia occurs postpartum (90% within 7 days of delivery)
-
Can occur without warning in 20% of cases
-
Progression from preeclampsia to eclampsia is unpredictable
-
Creasy & Resnik's Maternal-Fetal Medicine, p. 1058
PATHOLOGY - ORGAN CHANGES
1. Kidney - "Glomerular Endotheliosis" (Pathognomonic Lesion)
- Swollen endothelial cells occlude capillary lumen
- Protrusion of glomerular tuft into proximal tubule
- Decreased GFR (opposite of normal pregnancy where GFR increases by 40-50%)
- Protein deposits in glomerular basement membrane
- Result: Proteinuria, oliguria, rising creatinine
2. Liver
- 60% of eclamptic women have gross hepatic lesions
- Early: Periportal hemorrhage - vasodilation → hepatocyte displacement
- Late: Hepatic infarction from intense vasospasm
- Hemorrhagic changes in 66%, necrotic changes in 40% of eclamptic women
- Severe: Subcapsular hemorrhage → risk of hepatic rupture (rare but fatal)
3. Brain
- Cerebral vasospasm + loss of autoregulation → cerebral edema
- PRES (Posterior Reversible Encephalopathy Syndrome) - vasogenic parietooccipital edema, typically reversible
- Petechial hemorrhages, white matter necrosis in severe/fatal cases
- Autopsy: white-matter predominant injury, ranging from mild edema to extensive necrosis
4. Placenta
- Multiple infarcts (from chronic hypoperfusion)
- Retroplacental hemorrhage → risk of abruption
- Syncytial knots (ischemic villi)
- Acute atherosis of decidual vessels (fibrinoid necrosis + lipid macrophages)
- Leads to: IUGR, oligohydramnios, fetal distress
5. Coagulation
- DIC in 10% of severe preeclampsia/eclampsia
- Platelet consumption → thrombocytopenia
- Elevated fibrin degradation products
- Microthrombi in liver, kidney
- Overt DIC → spontaneous hemorrhage
HELLP SYNDROME
H = Hemolysis (microangiopathic hemolytic anemia - schistocytes on smear) EL = Elevated Liver enzymes (AST, ALT > 2x normal) LP = Low Platelets (< 100,000/µL, often < 50,000)
Occurs in ~10% of severe preeclampsia cases
Clinical presentation:
- May present WITHOUT classic hypertension or proteinuria
- RUQ/epigastric pain + malaise + nausea + vomiting
- Often confused with cholecystitis, hepatitis, or gastritis
- Can present in emergency department
Complications:
- DIC
- Acute renal failure
- Pulmonary edema
- Placental abruption
- Hepatic rupture (rare, surgical emergency)
- Maternal and perinatal mortality
Management: Urgent delivery is the only definitive treatment
INVESTIGATIONS
| Investigation | What to Check | Significance |
|---|---|---|
| BP monitoring | Serial readings ≥ 4 hrs apart | Diagnosis |
| Urine protein | 24-hr urine or P:Cr ratio | Diagnosis |
| CBC + platelets | Platelet count, Hb, smear | Thrombocytopenia, hemolysis |
| LFTs | AST, ALT | HELLP, liver involvement |
| Renal | Creatinine, uric acid, BUN | Renal involvement |
| Uric acid | Often elevated early | Early marker (often precedes clinical disease) |
| Coagulation | PT, aPTT, fibrinogen | DIC screening |
| Fetal monitoring | CTG, BPP, Doppler | Fetal wellbeing |
| Ultrasound | Growth, AFI, Doppler | IUGR, oligohydramnios |
| MRI/CT head | If neurological signs | PRES, hemorrhage, edema |
MANAGEMENT
The Definitive Treatment = DELIVERY (delivery of the placenta)
All other treatment is supportive, not curative. The decision is always: maternal risk of continuing pregnancy vs. fetal risk of prematurity.
A. Antihypertensive Therapy
Threshold: BP ≥ 160/110 mmHg = EMERGENCY - must treat within 30-60 minutes
- Goal: SBP < 160 mmHg, DBP < 110 mmHg
- Do NOT lower BP too fast - risk of uteroplacental insufficiency
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Labetalol (1st line) | 10-20 mg IV; repeat 20-80 mg q10-30 min; max 300 mg | IV | Alpha + beta blocker; preserves uteroplacental flow; no neonatal sympathetic blockade |
| Hydralazine (1st line) | 5 mg IV; repeat 5-10 mg q20-40 min; max 20 mg | IV | ACOG endorsed; arteriolar vasodilator; increases uterine and renal blood flow; watch for reflex tachycardia |
| Nifedipine (oral, 1st line) | 10-20 mg orally; repeat in 20 min if needed | Oral | Given before IV access; calcium channel blocker; can cause uterine relaxation (risk of atony) |
| Nicardipine | 5-30 mg/hr infusion | IV | Smooth rapid BP fall; increases renal perfusion |
| Methyldopa | 250-500 mg TDS | Oral | For chronic/maintenance treatment |
| Nitroprusside | 0.3 µg/kg/min infusion | IV | Reserved for refractory cases; cyanide toxicity risk with prolonged use |
Avoid: ACE inhibitors, ARBs (contraindicated - fetal renal toxicity)
B. Seizure Prophylaxis & Treatment: Magnesium Sulfate
MgSO₄ is FIRST-LINE for both prevention and treatment of eclamptic seizures.
Loading dose: 4 g IV over 15-20 minutes
Maintenance: 1-2 g/hour IV infusion
How it works:
- Calcium antagonism → smooth muscle relaxation → peripheral and cerebral vasodilation
- Protects blood-brain barrier → limits cerebral edema
- Increases prostacyclin release from endothelium
- Decreases plasma renin activity
- Central anticonvulsant activity
- Note: Has only modest antihypertensive effect - additional drugs still needed for BP
Who gets prophylaxis?
- Preeclampsia WITH severe features (especially clonus, severe headache, visual scotomata)
- Does NOT need to be given for preeclampsia without severe features (seizure risk is extremely low and drug toxicity occurs in up to 25%)
Monitoring for toxicity:
| Sign | Serum Mg Level |
|---|---|
| Loss of patellar reflex | 7-10 mEq/L |
| Respiratory depression | 10-13 mEq/L |
| Respiratory arrest | > 15 mEq/L |
| Cardiac arrest | > 15 mEq/L |
Antidote: Calcium gluconate 1 g IV (10 mL of 10% solution) - keep at bedside!
C. Management of an Eclamptic Seizure
Step-by-step protocol:
1. AIRWAY - Position left lateral, suction airway, give O₂
2. SECURE IV ACCESS
3. MgSO₄ 4g IV bolus (if not already on it)
→ If already on MgSO₄: give extra 2g IV
→ If seizure persists: diazepam 5-10 mg IV
4. BLOOD PRESSURE CONTROL - if ≥ 160/110 mmHg
5. FETAL MONITORING - continuous CTG after stabilization
6. DO NOT rush to deliver during the seizure
7. PLAN DELIVERY after maternal stabilization
8. AIRWAY PROTECTION - intubation if needed
Important: 30% of eclampsia is postpartum - continue MgSO₄ for at least 24 hours after delivery.
D. Fluid Management
Key concept: Preeclampsia is a volume-CONTRACTED, NOT volume-depleted state.
- Capillary permeability is increased - IV fluids leak into interstitium
- Do NOT give aggressive IV fluids - risk of pulmonary edema
- Restrict IVF to ~85 mL/hour in severe cases
- Central venous pressure monitoring is NOT routinely indicated
E. Delivery Timing (OB Exam Favourite!)
| Clinical Situation | Gestational Age | Decision |
|---|---|---|
| Preeclampsia WITHOUT severe features | ≥ 37 weeks | Deliver |
| Preeclampsia WITHOUT severe features | 34-37 weeks | Expectant management with close monitoring acceptable |
| Preeclampsia WITH severe features | ≥ 34 weeks | Deliver |
| Preeclampsia WITH severe features | < 34 weeks | Individualize - may attempt corticosteroids for lung maturity then deliver |
| HELLP syndrome | Any gestational age | Deliver (emergency) |
| Eclampsia | Any gestational age | Deliver after maternal stabilization |
Mode of delivery: Vaginal delivery is preferred when feasible. Caesarean not mandatory for preeclampsia alone. Decision based on obstetric indications.
F. HELLP Syndrome Management
- Urgent delivery (regardless of gestational age)
- Correct coagulopathy (FFP, platelets if < 20,000-30,000)
- Platelet transfusion for platelets < 20,000-30,000/µL (for delivery)
- MgSO₄ for seizure prophylaxis
- Antihypertensives for severe BP
- No evidence for corticosteroids or plasma exchange improving outcomes
- Refer to tertiary center if local facilities inadequate
PREVENTION
| Intervention | Evidence | Recommendation |
|---|---|---|
| Low-dose aspirin (75-150 mg/day, start at 12-16 weeks) | Reduces risk by ~10-20% in high-risk women | ACOG recommended for high-risk women |
| Calcium supplementation | Beneficial in calcium-deficient populations | Recommended where dietary calcium is low |
| Weight loss before pregnancy | Reduces risk in obese women | Counselled pre-conception |
| Antioxidants (Vit C, Vit E) | NOT effective | Not recommended |
| Salt restriction | NOT effective | Not recommended |
Who qualifies for aspirin prophylaxis (ACOG)?
- Any 1 HIGH-risk factor: previous preeclampsia, multifetal gestation, CKD, autoimmune disease (APS, SLE), diabetes, chronic HTN
- Any 2+ MODERATE-risk factors: nulliparity, obesity, family history, Black race, low socioeconomic status, age ≥ 35, IVF
MATERNAL COMPLICATIONS SUMMARY
| Complication | Mechanism |
|---|---|
| Intracranial hemorrhage | Uncontrolled severe HTN (93% of strokes are hemorrhagic) |
| Stroke | Cerebral vasospasm, hemorrhage |
| Pulmonary edema | Endothelial leakage + iatrogenic fluid overload |
| Acute renal failure | Glomerular endotheliosis + renal vasospasm |
| Hepatic rupture | Subcapsular hematoma → rupture |
| DIC | Endothelial dysfunction → coagulation cascade activation |
| Placental abruption | Vasospasm → retroplacental hemorrhage |
| Maternal death | Intracranial bleed, liver failure, pulmonary complications |
FETAL COMPLICATIONS
| Complication | Cause |
|---|---|
| IUGR | Placental insufficiency |
| Prematurity | Medically indicated early delivery |
| Placental abruption | Retroplacental hemorrhage |
| Fetal distress/hypoxia | Chronic uteroplacental insufficiency |
| Oligohydramnios | Decreased renal perfusion (fetal) |
| Intrauterine fetal demise | Severe placental compromise |
PROGNOSIS & LONG-TERM EFFECTS
- HTN and proteinuria resolve within 1-2 weeks postpartum in most cases
- No lasting sequelae in uncomplicated cases
- Preeclampsia is a marker for future cardiovascular disease in the mother:
- 2x lifetime risk of hypertension
- 2x risk of ischemic heart disease
- 2x risk of stroke
- Recurrence risk: ~15-25% in future pregnancies; higher if early-onset or severe
QUICK EXAM SUMMARY BOX
PREECLAMPSIA = BP ≥ 140/90 after 20 wks + Proteinuria OR end-organ damage
SEVERE FEATURES = BP ≥ 160/110 OR platelets <100K OR creatinine >1.1
OR liver enzymes >2x OR pulmonary edema OR neuro symptoms
ECLAMPSIA = Preeclampsia + Grand mal seizures
HELLP = Hemolysis + Elevated Liver enzymes + Low Platelets (10% of severe PE)
TREATMENT:
- Definitive = DELIVERY
- Seizure = MgSO₄ (4g IV load → 1-2g/hr)
- BP ≥ 160/110 = Labetalol / Hydralazine / Nifedipine
- Antidote for Mg toxicity = Calcium gluconate 1g IV
DELIVER AT:
- ≥37 wks = any preeclampsia
- ≥34 wks = severe features
- Any gestation = eclampsia, HELLP
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice (primary OB/GYN reference used throughout)
This is a shared conversation. Sign in to Orris to start your own chat.