Thyroiditis clinical features, management
Reading File
Finding Sources
Searching PubMed
thyroiditis management clinical features
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compose the full answer.
Thyroiditis: Clinical Features and Management
Thyroiditis encompasses a diverse group of disorders characterized by thyroid inflammation. They are best classified by onset/duration (acute, subacute, chronic) and by pain (painful vs. painless).
Classification Overview
| Type | Also Known As | Cause | Pain |
|---|---|---|---|
| Acute suppurative | Bacterial thyroiditis | Staph, Strep, Enterobacter | Yes |
| Subacute granulomatous | De Quervain's, viral thyroiditis | Viral (mumps, coxsackie, COVID-19) | Yes |
| Subacute lymphocytic | Silent / painless thyroiditis | Autoimmune | No |
| Postpartum thyroiditis | - | Autoimmune | No |
| Hashimoto's | Chronic autoimmune / chronic lymphocytic | Autoimmune | Rarely |
| Riedel's | Fibrous thyroiditis | Unknown (IgG4-related?) | No |
| Drug-induced | - | IFN, amiodarone, checkpoint inhibitors | Variable |
- Harrison's Principles of Internal Medicine 22E, p. 3081 (Table 396-3)
1. Acute (Suppurative) Thyroiditis
Clinical Features
- Rare; caused by bacterial infection (Staphylococcus, Streptococcus, Enterobacter) or fungal organisms in immunocompromised patients
- In children/young adults: often due to a piriform sinus (4th branchial pouch remnant, predominantly left-sided)
- Thyroid pain, often referred to the throat or ears
- Small, tender, asymmetric goiter; fever, dysphagia, erythema over thyroid, lymphadenopathy
- ESR and WBC elevated; thyroid function usually normal
- FNA shows PMN infiltration; culture identifies organism
Management
-
Antibiotics guided by Gram stain and FNA cultures
-
Surgery to drain abscess (localized by CT/ultrasound) if needed
-
Complications if untreated: tracheal obstruction, septicemia, mediastinitis, jugular venous thrombosis
-
Harrison's, p. 3081
2. Subacute Granulomatous Thyroiditis (De Quervain's)
Epidemiology
- Most common cause of a painful thyroid gland
- Accounts for ~5% of clinical thyroid disorders
- Peak incidence 30-50 years; women affected 3-5x more than men
- Often follows viral prodrome (mumps, coxsackie, influenza, adenovirus, echovirus, SARS-CoV-2)
Pathophysiology
Follicular disruption → release of stored T4/T3 → thyrotoxicosis → hormone depletion → hypothyroidism → recovery (see diagram below)
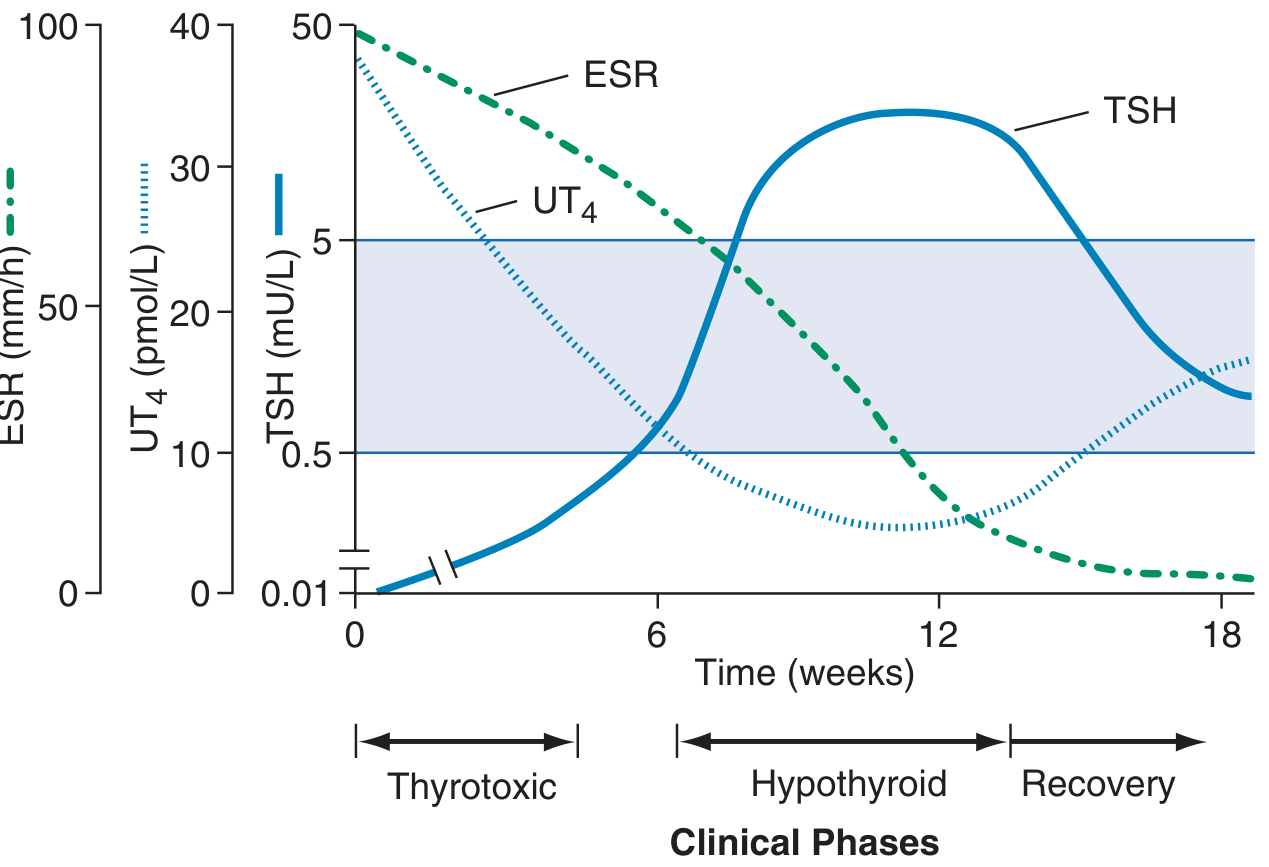
Figure: Clinical course of subacute thyroiditis (Harrison's 22E, Fig. 396-3). ESR peaks early; free T4 rises then falls; TSH is suppressed initially then rises during the hypothyroid phase before recovering.
Clinical Features
- Painful, enlarged thyroid (often exquisitely tender), sometimes asymmetric
- Pain referred to jaw or ear
- Malaise, low-grade fever, sore throat (may mimic pharyngitis)
- Symptoms of thyrotoxicosis or hypothyroidism depending on phase
- In 10%: acute, severe onset with marked hyperthyroid symptoms
- In 33%: asymptomatic except for goiter
Three clinical phases:
- Thyrotoxic phase (weeks 1-6): raised T4/T3, suppressed TSH, low radioiodine uptake (<5%)
- Hypothyroid phase (weeks 6-12): low T4, elevated TSH
- Recovery phase (weeks 12-18+): normalization of all tests
Investigations
- ESR markedly elevated (often >50 mm/h)
- Low radioiodine uptake or 99mTc pertechnetate uptake (distinguishes from Graves' disease)
- T4:T3 ratio lower than in Graves' (stored hormone release rather than de novo synthesis)
- Thyroid antibodies negative
- FNA (if needed): giant cells, granulomas
Management
| Phase | Treatment |
|---|---|
| Pain / inflammation | NSAIDs (aspirin, ibuprofen) for mild cases |
| Severe pain | Prednisolone 10-20 mg/day x 7 days, then taper over 4 weeks |
| Thyrotoxic phase | Beta-blockers (propranolol, atenolol) - NOT antithyroid drugs (no new hormone synthesis) |
| Hypothyroid phase | Levothyroxine if symptomatic or prolonged |
-
Most patients recover fully within 6 months
-
Permanent hypothyroidism in ~15% (especially if coincident thyroid autoimmunity)
-
Recurrence uncommon but possible
-
Harrison's, p. 3082; Goldman-Cecil Medicine, p. 2440; Bailey and Love's Surgery 28e, p. 893
3. Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis)
Epidemiology
- Most common cause of hypothyroidism in iodine-sufficient regions
- Peak age 45-65 years; female predominance 10:1 to 20:1
- Strong genetic component: CTLA4, PTPN22, IL2RA polymorphisms
Pathogenesis
Breakdown of self-tolerance to thyroid antigens (thyroglobulin, thyroid peroxidase) → CD8+ cytotoxic T-cell mediated destruction + CD4+ Th1 cytokine-mediated apoptosis + antibody-dependent cytotoxicity → progressive follicular destruction and fibrosis
Histology
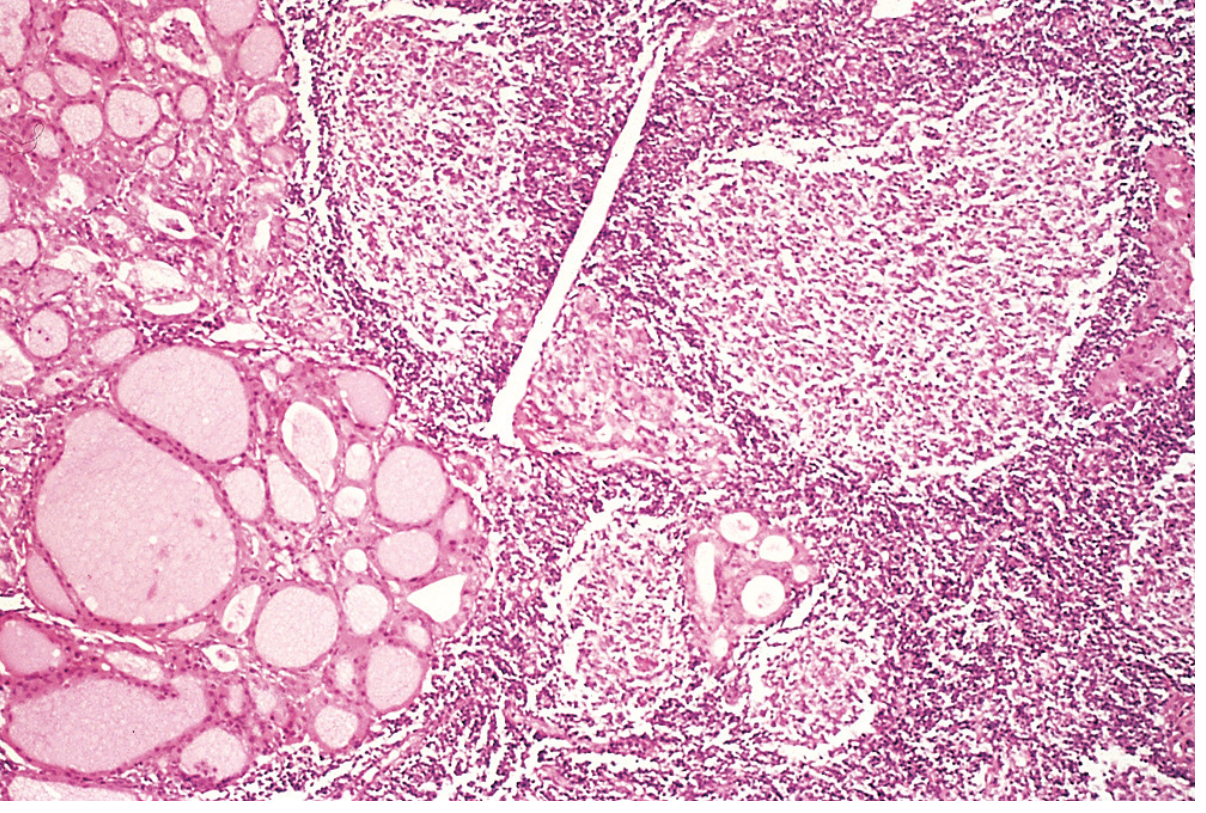
Fig. 24.11: Hashimoto thyroiditis - dense lymphocytic infiltrate with germinal centers; residual follicles lined by oncocytic (Hürthle) cells. (Robbins & Cotran Pathologic Basis of Disease)
Gross: diffusely enlarged, firm, pale yellow-tan gland, well-demarcated. Microscopy: lymphocytes + plasma cells, lymphoid follicles with germinal centers, oncocytic (Hürthle cell) metaplasia, fibrosis (does NOT extend beyond the gland - differentiates from Riedel's).
Clinical Features
- Painless goiter - diffuse, symmetric, firm, "bosselated" texture
- Gradual onset of hypothyroid symptoms: fatigue, weight gain, cold intolerance, constipation, impaired concentration, dry skin, hair loss
- Early phase: sometimes hashitoxicosis (transient thyrotoxicosis from follicular disruption)
- Eventually: primary myxoedema (end stage, no goiter)
- Associated autoimmune diseases: T1DM, Addison's disease, SLE, myasthenia gravis, Sjögren's syndrome
- Increased risk of thyroid lymphoma (most lymphomas arise on a background of lymphocytic thyroiditis)
Investigations
- TSH elevated; free T4 low (or normal in subclinical hypothyroidism)
- Anti-TPO antibodies positive in >90% (anti-thyroglobulin also elevated)
- Ultrasound: heterogeneous, hypoechoic gland
- FNA: oncocytes + heterogeneous lymphocytes (characteristic)
Management
-
Levothyroxine replacement for overt hypothyroidism (titrate to normalize TSH)
-
Subclinical hypothyroidism (elevated TSH, normal T4): treat if TSH >10 mIU/L, or if symptomatic, pregnant, or planning pregnancy
-
Monitor thyroid function annually if not on replacement
-
Goiter causing compressive symptoms: levothyroxine may reduce size; surgery rarely needed
-
Robbins & Cotran, p. 998-999; Bailey and Love's, p. 893
4. Postpartum / Sporadic Silent (Painless) Thyroiditis
Epidemiology
- Postpartum thyroiditis: up to 10% of pregnancies; 20x more common postpartum than Graves' disease
- More frequent with positive anti-TPO antibodies in 1st trimester or personal/family history of autoimmunity
- Sporadic (non-postpartum) silent thyroiditis: age 30-60, female > male (1.5:1)
- Both are variants of the same autoimmune destruction-induced thyroiditis
Clinical Features
- Painless goiter (nontender)
- Classic sequence: thyrotoxic phase (1-3 months) → euthyroid (1-2 months) → hypothyroid phase (up to 12 months)
- Not all patients complete the full sequence: ~25% experience only thyrotoxicosis; ~50% only hypothyroidism
- Thyrotoxic phase: tachycardia, palpitations, heat intolerance (milder than Graves')
- Hypothyroid phase: fatigue, constipation, cold intolerance, impaired concentration
Diagnosis
- Toxic phase: raised free T4/T3, suppressed TSH; T3:T4 ratio <20 (distinguishes from Graves')
- Anti-TPO antibodies positive; TSH-receptor antibodies negative (key distinction from Graves')
- Low/absent radioiodine uptake; ultrasound: heterogeneous, hypoechoic; Doppler flow markedly decreased (vs. increased in Graves')
Management
-
Self-limiting course
-
Thyrotoxic phase: beta-blockers (atenolol 25-50 mg/day) for moderate/severe symptoms; antithyroid drugs NOT effective
-
Hypothyroid phase: levothyroxine if symptomatic or severe; taper after 6-12 months to reassess recovery
-
Pregnancy: continue levothyroxine throughout pregnancy if initiated
-
Prognosis: up to 50% remain chronically hypothyroid; recurs after 70% of subsequent pregnancies; higher risk with high anti-TPO titers
-
Goldman-Cecil Medicine, p. 2439-2440
5. Riedel's Thyroiditis
-
Very rare (0.5% of goiters)
-
Thyroid replaced by cellular fibrous tissue that infiltrates surrounding structures (trachea, muscles, parathyroids, recurrent laryngeal nerve)
-
Presents as a rock-hard, fixed goiter with compressive symptoms (dysphagia, stridor, hypothyroidism)
-
Associated with IgG4-related systemic disease and other fibrosclerotic conditions
-
Management: surgery to relieve compression; corticosteroids; tamoxifen (antifibrotic); levothyroxine for hypothyroidism
-
Bailey and Love's, p. 893
Drug-Induced Thyroiditis
Common culprits and their patterns:
| Drug | Pattern |
|---|---|
| Amiodarone | Type 1 (iodine-excess Graves'-like) or Type 2 (destructive thyroiditis) |
| Interferon-alpha | Hashimoto-like or Graves'-like |
| Immune checkpoint inhibitors (anti-PD-1/CTLA-4) | Destructive thyroiditis (painless) |
| Tyrosine kinase inhibitors | Hypothyroidism or thyroiditis |
| Lithium | Hypothyroidism / goiter |
Summary Table: Key Distinguishing Features
| Feature | Acute Suppurative | Subacute (De Quervain's) | Hashimoto's | Postpartum/Silent |
|---|---|---|---|---|
| Pain | Severe | Moderate-severe | None | None |
| Fever | Yes | Yes (low-grade) | No | No |
| Goiter | Asymmetric, tender | Tender, firm | Firm, bosselated | Soft, nontender |
| ESR | Elevated | Markedly elevated | Normal | Normal |
| RAI uptake | Normal | Very low (<5%) | Normal/low | Very low |
| TPO antibodies | Negative | Negative | Positive (>90%) | Positive |
| TSH-RAb | Negative | Negative | Negative | Negative |
| Self-limiting? | With antibiotics | Yes (~6 months) | No (chronic) | Usually (may persist) |
This is a shared conversation. Sign in to Orris to start your own chat.