Ingheritrd metabolic disorders of liver
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Now I have comprehensive information from the textbooks. Let me compile the full, detailed answer.
Inherited Metabolic Disorders of the Liver
Inherited metabolic liver diseases are genetic conditions where enzyme or transporter defects cause hepatotoxic substrate accumulation, deficiency of essential products, or protein misfolding. They account for approximately 13% of all liver transplants in the USA and ~22% of pediatric liver transplants. They may present acutely as neonatal liver failure or chronically as cirrhosis/HCC in adulthood.
Clinical Features: When to Suspect
Any of the following should raise suspicion (from the Box 77.1 of Sleisenger & Fordtran's):
| Symptoms | Signs |
|---|---|
| Coma, seizures | Ascites, jaundice |
| Developmental delay / regression | Hepatomegaly, splenomegaly |
| Growth failure | Kayser-Fleischer rings (eyes) |
| Hyperammonemia, hypoglycemia | Rickets |
| Recurrent vomiting | Chronic liver disease features |
Key history clues: consanguinity, multiple miscarriages, early infant deaths, food-related symptom onset (urea cycle defects, galactosemia, fructosemia), dietary aversions.
Major Disorders
1. Alpha-1-Antitrypsin (α1-AT) Deficiency
- Genetics: Autosomal recessive; most common: PiZZ phenotype (homozygous for Z allele)
- Mechanism: α1-AT Z protein misfolds and polymerizes inside hepatocytes (gain-of-function hepatotoxicity) - the misfolded protein cannot be secreted, so it accumulates. Simultaneously, lack of circulating α1-AT causes uninhibited neutrophil elastase activity, leading to emphysema (especially in smokers).
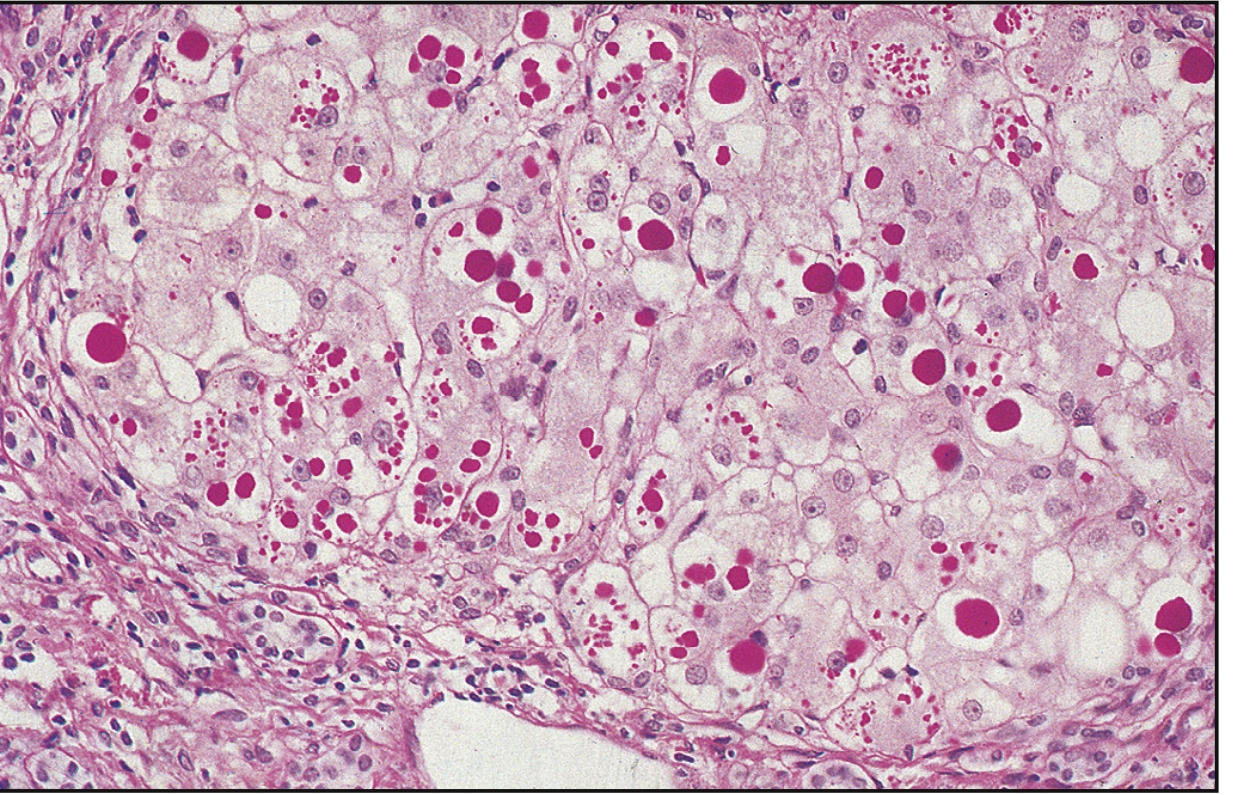
- Liver pathology: PAS-positive, diastase-resistant globules in periportal hepatocytes - the hallmark finding. May progress from neonatal cholestasis → chronic hepatitis → cirrhosis → HCC.
- Diagnosis: Serum α1-AT phenotype analysis (not just level, since it is an acute-phase reactant). PCR for common alleles. Liver biopsy confirms PAS+ globules.
- Histology image (PAS stain):
- Treatment:
- No disease-specific therapy for liver disease exists; management is supportive
- Avoid alcohol, smoking, obesity, ensure fat-soluble vitamin supplementation
- Emerging: RNA interference (siRNA to block Z-variant mRNA), CRISPR-based gene editing, autophagy-enhancing drugs (carbamazepine, rapamycin) to clear misfolded protein
- Lung disease only: FDA-approved augmentation therapy with purified α1-AT (IV infusion) - does NOT benefit liver disease
- Liver transplantation: Most common genetic liver disease requiring LT. Corrects both the liver damage and the metabolic defect. 5-year survival: 83-90%
- HCC surveillance: liver US every 6 months in cirrhotics (AASLD guidelines)
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter 77)
2. Hereditary Hemochromatosis (HH)
- Genetics: Most commonly mutations in the HFE gene (C282Y homozygosity most pathogenic; C282Y/H63D compound heterozygous less so); also mutations in hepcidin, hemojuvelin, ferroportin genes
- Mechanism: Decreased hepcidin levels or function → unregulated intestinal iron absorption → progressive iron accumulation in liver, pancreas, heart, pituitary, joints
- Liver manifestations: Hepatomegaly → cirrhosis → HCC (major cause of death; risk increases 200-fold with cirrhosis)
- Classic pentad: Cirrhosis + diabetes mellitus ("bronze diabetes") + skin bronzing + cardiac disease + hypogonadism
- Key lab: Elevated serum ferritin, elevated transferrin saturation (>45% screening threshold); HFE genotyping confirms
- Hepatic iron index (HII): >1.9 distinguishes HH from secondary iron overload (e.g., alcoholic liver disease - where few patients are C282Y homozygous)
- Diagnosis: HFE mutation testing + HII on liver biopsy; Prussian blue stain shows iron deposits
- Treatment:
- Phlebotomy - weekly until ferritin <50 µg/L, then maintenance every 3-4 months
- Chelation (desferrioxamine) if phlebotomy not feasible
- Avoid alcohol, vitamin C supplements (increases iron absorption)
- Liver transplantation for end-stage disease (outcomes poorer than other etiologies due to cardiac involvement)
(Sleisenger & Fordtran's, Chapter 75; Robbins & Kumar Basic Pathology)
3. Wilson Disease
- Genetics: Autosomal recessive; loss-of-function mutations in ATP7B gene (chromosome 13) encoding a copper-transporting P-type ATPase
- Mechanism: Defective hepatic copper excretion into bile → copper accumulates in liver first, then overflows to brain (basal ganglia), eyes, kidneys, red blood cells
- Liver manifestations: Protean - ranging from:
- Asymptomatic elevated LFTs
- Fatty liver disease
- Chronic hepatitis
- Acute liver failure (ALF) - characteristic presentation in 2nd decade; unique clue: ALP:bilirubin ratio <4 and AST:ALT ratio >2.2 in ALF distinguish Wilson's from other causes
- Cirrhosis (macronodular)
- Extra-hepatic:
- Kayser-Fleischer (KF) rings - copper deposits in Descemet's membrane of cornea; slit-lamp examination (usually present in ALF and neurological disease)
- Neuropsychiatric: dysarthria, tremor, personality change, psychosis
- Hemolytic anemia (Coombs-negative - from copper-induced RBC oxidative injury)
- Renal tubular acidosis (Fanconi syndrome)
- Diagnosis: Slit-lamp for KF rings + serum ceruloplasmin (low, <20 mg/dL) + 24-hr urinary copper (elevated >100 µg/day) + liver biopsy with copper quantification. Leipzig scoring system used.
- Treatment:
- Chelation: D-penicillamine (1st line historically; side effects: rash, nephropathy, neurological worsening initially) or Trientine (better tolerated)
- Zinc: Blocks intestinal copper absorption (maintenance therapy; safe in pregnancy)
- Tetrathiomolybdate: Investigational; fast-acting for neurological disease
- ALF from Wilson's: emergency liver transplantation (corrects the metabolic defect permanently)
- Note: patients who discontinue chelation can re-present with ALF years later
(Sleisenger & Fordtran's, Chapter 75 & Chapter 95; Robbins & Kumar)
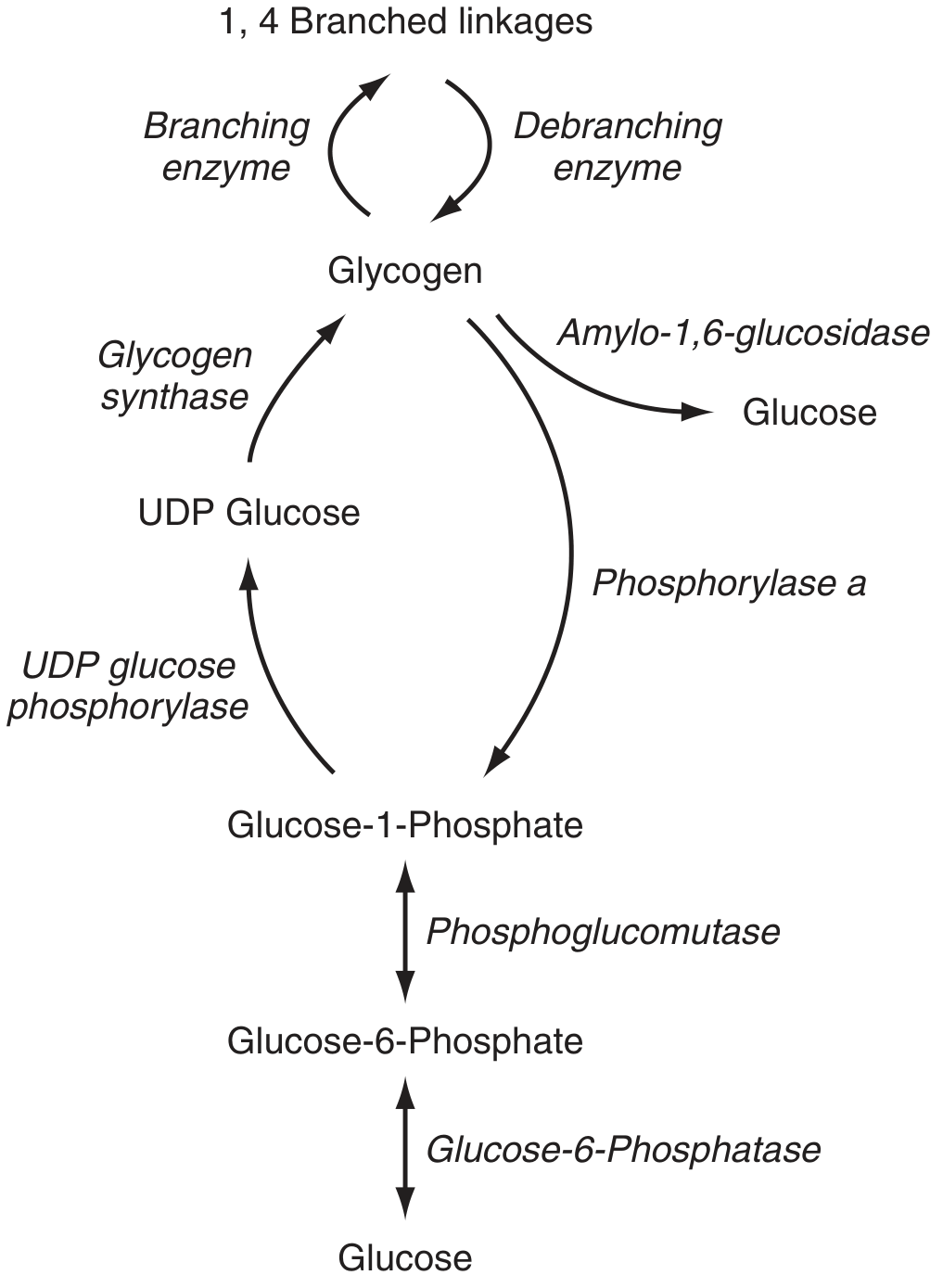
4. Glycogen Storage Diseases (GSDs)
Over 12 inborn errors of glycogen metabolism exist; 3 cause serious liver disease:
| Type | Enzyme Defect | Gene | Key Features |
|---|---|---|---|
| GSD Type I (von Gierke) | Glucose-6-phosphatase | G6PC | Severe hypoglycemia, hepatomegaly, lactic acidosis, hyperuricemia, hyperlipidemia; risk of hepatic adenomas → HCC |
| GSD Type III (Cori/Forbes) | Debranching enzyme | AGL | Moderate hypoglycemia, hepatomegaly, myopathy; liver disease often improves with age |
| GSD Type IV (Andersen) | Branching enzyme | GBE1 | Accumulation of amylopectin in hepatocytes (PAS-positive inclusions); macronodular cirrhosis; most die within 3 years without treatment; LT corrects metabolic error but amylopectin may persist in heart (cardiomyopathy) |
- Glycogen metabolism pathway diagram:
- Diagnosis: Enzyme assay in liver/fibroblasts + molecular genetic testing
- Treatment (Type I): Frequent feeds/uncooked cornstarch to prevent hypoglycemia; raw cornstarch is the mainstay. Avoid fructose and galactose.
(Sleisenger & Fordtran's Chapter 77)
5. Hereditary Tyrosinemia Type 1 (HT-1)
- Genetics: AR; deficiency of fumarylacetoacetate hydrolase (FAH), the final enzyme of tyrosine catabolism
- Mechanism: Toxic metabolites succinylacetone (SA) and succinylacetoacetate (SAA) accumulate - directly injure liver cells, kidneys, and nerves; SA is a potent inhibitor of heme synthesis (delta-ALA dehydratase → porphyria-like crises)
- Presentation:
- Acute form (onset <6 months): liver failure with coagulopathy, hypoglycemia, ascites, jaundice; serum AFP markedly elevated; 77% present before 6 months
- Chronic form (onset >1 year): hepatomegaly, rickets, nephromegaly, hypertension, growth retardation; ~30% develop HCC (even before cirrhosis)
- Neurologic crises mimicking acute porphyria
- Diagnosis: Elevated urinary succinylacetone (pathognomonic), elevated plasma tyrosine/methionine, elevated AFP; FAH enzyme assay in liver/fibroblasts
- Treatment:
- Nitisinone (NTBC): 2-(2-nitro-4-trifluoromethylbenzoyl)-1,3-cyclohexanedione - blocks upstream enzyme (4-HPPD), preventing formation of SA/SAA; dramatically improves survival
- Low-tyrosine, low-phenylalanine diet
- LT: curative if NTBC fails or HCC develops
(Sleisenger & Fordtran's Chapter 77)
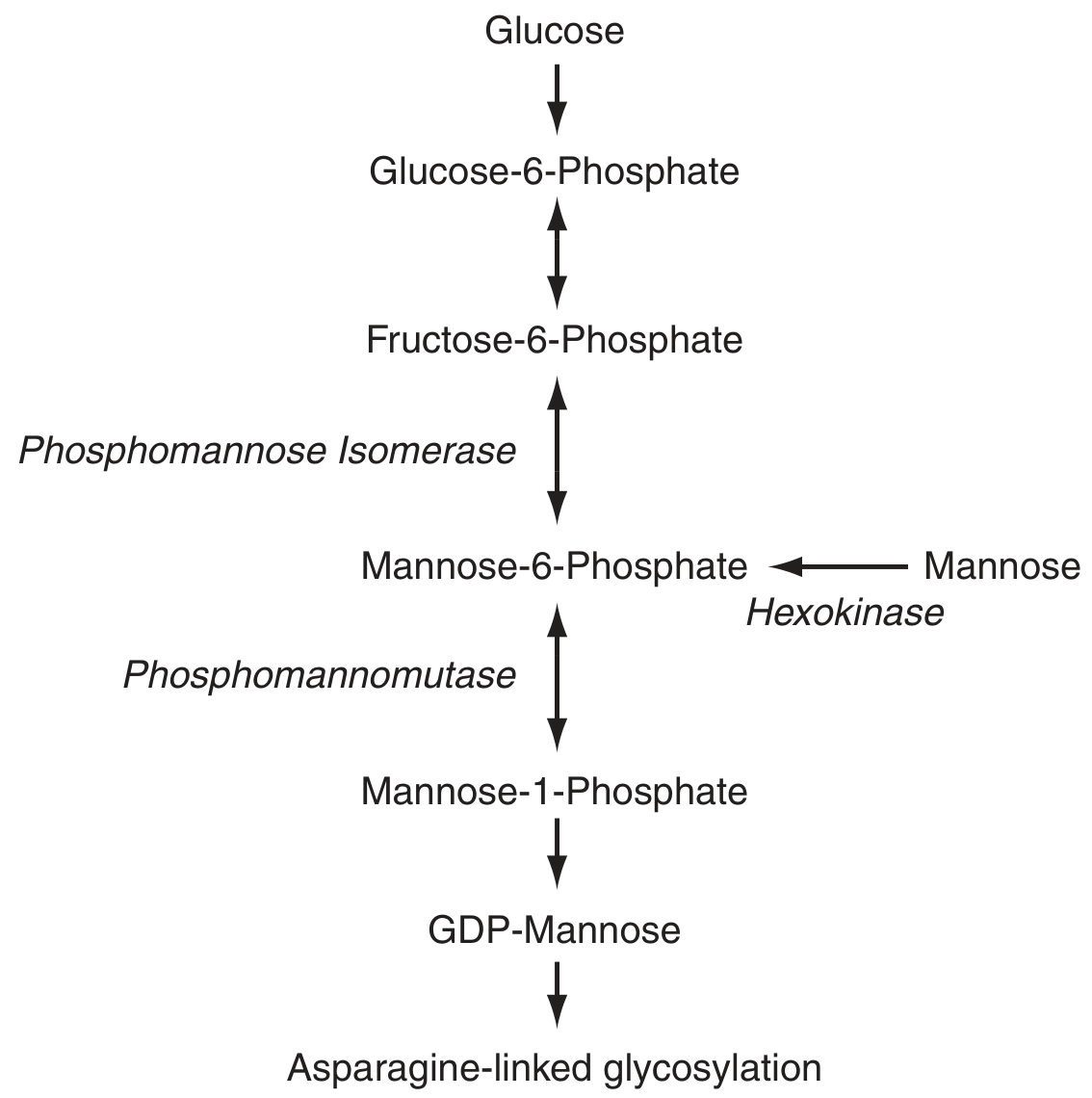
6. Congenital Disorders of Glycosylation (CDGs)
- A group of >130 inherited defects in glycoprotein synthesis
- Hepatic dysfunction in ~22% of patients; usually mild (steatosis, fibrosis); rarely cirrhosis
- Electron microscopy: myelosomes (lysosomal vacuoles with concentric electron-dense membranes)
- Key lab: serum transferrin isoelectric focusing (best marker for N-glycosylation defects)
- CDG Type Ib (MPI-CDG): Defect in phosphomannose isomerase; presents with intractable diarrhea, protein-losing enteropathy, congenital hepatic fibrosis, hyperinsulinemic hypoglycemia; only specifically treatable CDG - oral mannose supplementation
- Any unexplained congenital hepatic fibrosis or protein-losing enteropathy should prompt CDG screen
(Sleisenger & Fordtran's Chapter 77)
7. Porphyrias
- Defects in the heme synthesis pathway; 8 types depending on which enzyme is defective
- Hepatic porphyrias cause liver disease; Acute intermittent porphyria (AIP) - most common acute type - presents with abdominal pain, autonomic instability, neuropsychiatric symptoms triggered by drugs/fasting/hormones
- Porphyria cutanea tarda (PCT): Accumulation of uroporphyrin in skin; associated with HCV, alcohol, HFE mutations, estrogens; blistering photosensitivity; treatment: phlebotomy or hydroxychloroquine
- HCC risk is elevated in some hepatic porphyrias
Diagnostic Approach
| Step | Action |
|---|---|
| 1 | Detailed history: family history of consanguinity, infant deaths, food triggers |
| 2 | Initial labs: LFTs, coagulation, glucose, ammonia, lactate, amino acids (plasma and urine), organic acids (urine) |
| 3 | Obtain samples during acute episode - many abnormalities normalize between episodes; freeze samples |
| 4 | Liver biopsy: standard histology + frozen sample for biochemical assay + EM for organelle changes |
| 5 | Molecular genetic testing for specific genotypic confirmation |
Summary Table
| Disease | Defect | Inheritance | Key Liver Feature | Hallmark Finding | Treatment |
|---|---|---|---|---|---|
| α1-AT Deficiency | α1-AT misfolding | AR | Neonatal cholestasis → cirrhosis | PAS+ diastase-resistant globules | Supportive; LT |
| Hemochromatosis | HFE / hepcidin pathway | AR | Cirrhosis, HCC | Prussian blue iron staining | Phlebotomy |
| Wilson Disease | ATP7B (copper ATPase) | AR | Fatty liver → ALF → cirrhosis | KF rings; low ceruloplasmin; high 24h urinary Cu | Penicillamine / Trientine / Zinc; LT for ALF |
| GSD Type I | Glucose-6-phosphatase | AR | Hepatomegaly, adenomas → HCC | Hypoglycemia + lactic acidosis | Cornstarch diet |
| GSD Type IV | Branching enzyme | AR | Macronodular cirrhosis | Amylopectin deposits (PAS+) | LT |
| Tyrosinemia Type 1 | FAH | AR | ALF / cirrhosis / HCC | Elevated succinylacetone (urine) | Nitisinone (NTBC) + diet |
| CDG Type Ib | Phosphomannose isomerase | AR | Congenital hepatic fibrosis | Abnormal transferrin IEF | Oral mannose |
| PCT (porphyria) | Uroporphyrinogen decarboxylase | Variable | HCC risk | Photosensitive blisters | Phlebotomy / hydroxychloroquine |
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 77 (Inherited Metabolic Liver Disease), Chapter 75 (Hemochromatosis), Chapter 95 (Acute Liver Failure)
- Robbins & Kumar Basic Pathology - Inherited Metabolic Liver Disease section
Create a presentatmake a presentation max 30 slides with all the interited metabolic disorders of liver except wilson and hemochromatosis
Reading File
Reading File
Running Command
mkdir -p /tmp/workspace/metabolic-liver-pptx && ls /tmp/workspace/
Writing File
~/metabolic-liver-pptx/create_pptx.py
from pptx import Presentation
from pptx.util import Inches, Pt, Emu
from pptx.dml.color import RGBColor
from pptx.enum.text import PP_ALIGN, MSO_ANCHOR
from pptx.util import Inches, Pt
import copy
prs = Presentation()
prs.slide_width = Inches(13.333)
prs.slide_height = Inches(7.5)
blank_layout = prs.slide_layouts[6]
# ─────────────── COLOUR PALETTE ───────────────
DARK_TEAL = RGBColor(0x00, 0x5C, 0x6A) # header background
MID_TEAL = RGBColor(0x00, 0x7D, 0x8E) # accent bar
LIGHT_TEAL = RGBColor(0xE0, 0xF5, 0xF7) # body background
AMBER = RGBColor(0xF5, 0xA6, 0x23) # highlight accent
WHITE = RGBColor(0xFF, 0xFF, 0xFF)
DARK_TEXT = RGBColor(0x1A, 0x1A, 0x2E)
MID_GREY = RGBColor(0x55, 0x65, 0x75)
RED_ACCENT = RGBColor(0xC0, 0x39, 0x2B)
GREEN_ACC = RGBColor(0x1E, 0x87, 0x5E)
# ─────────────── HELPER FUNCTIONS ───────────────
def add_rect(slide, x, y, w, h, fill_rgb, transparency=0):
shape = slide.shapes.add_shape(1, Inches(x), Inches(y), Inches(w), Inches(h))
shape.fill.solid()
shape.fill.fore_color.rgb = fill_rgb
shape.line.fill.background()
return shape
def add_textbox(slide, text, x, y, w, h,
font_size=18, bold=False, color=DARK_TEXT,
align=PP_ALIGN.LEFT, italic=False, wrap=True, v_anchor=MSO_ANCHOR.TOP):
tb = slide.shapes.add_textbox(Inches(x), Inches(y), Inches(w), Inches(h))
tf = tb.text_frame
tf.word_wrap = wrap
tf.vertical_anchor = v_anchor
tf.margin_left = Pt(2)
tf.margin_right = Pt(2)
tf.margin_top = Pt(2)
tf.margin_bottom = Pt(2)
p = tf.paragraphs[0]
p.alignment = align
run = p.add_run()
run.text = text
run.font.size = Pt(font_size)
run.font.bold = bold
run.font.italic = italic
run.font.color.rgb = color
run.font.name = "Calibri"
return tb, tf
def add_bullet_slide(slide, title, bullets, sub_col2=None):
"""Standard content slide with header bar and bullet list (optionally 2-col)."""
# BG
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_TEAL)
# Top header bar
add_rect(slide, 0, 0, 13.333, 1.1, DARK_TEAL)
# Accent stripe
add_rect(slide, 0, 1.1, 13.333, 0.06, AMBER)
# Title text
add_textbox(slide, title, 0.35, 0.1, 12.5, 0.95,
font_size=30, bold=True, color=WHITE,
align=PP_ALIGN.LEFT, v_anchor=MSO_ANCHOR.MIDDLE)
# Slide number box (bottom right)
# Body
if sub_col2 is None:
tf_body = slide.shapes.add_textbox(Inches(0.5), Inches(1.25), Inches(12.3), Inches(5.9))
tf = tf_body.text_frame
tf.word_wrap = True
tf.margin_left = Pt(4)
tf.margin_right = Pt(4)
tf.margin_top = Pt(4)
_fill_bullets(tf, bullets)
else:
# Two columns
half = 6.1
tf_body1 = slide.shapes.add_textbox(Inches(0.5), Inches(1.25), Inches(half), Inches(5.9))
tf1 = tf_body1.text_frame
tf1.word_wrap = True
_fill_bullets(tf1, bullets)
tf_body2 = slide.shapes.add_textbox(Inches(6.8), Inches(1.25), Inches(half), Inches(5.9))
tf2 = tf_body2.text_frame
tf2.word_wrap = True
_fill_bullets(tf2, sub_col2)
# divider
add_rect(slide, 6.65, 1.3, 0.04, 5.8, MID_TEAL)
def _fill_bullets(tf, bullets):
"""bullets = list of (level, text, bold_flag, color_override)"""
from pptx.oxml.ns import qn
from lxml import etree
first = True
for item in bullets:
if isinstance(item, str):
level, text, bold, col = 0, item, False, DARK_TEXT
elif len(item) == 2:
level, text = item; bold = False; col = DARK_TEXT
elif len(item) == 3:
level, text, bold = item; col = DARK_TEXT
else:
level, text, bold, col = item
if first:
p = tf.paragraphs[0]
first = False
else:
p = tf.add_paragraph()
p.level = level
indent_map = {0: Pt(0), 1: Pt(18), 2: Pt(34)}
p.space_before = Pt(3 if level == 0 else 1)
p.space_after = Pt(1)
run = p.add_run()
run.text = text
size_map = {0: 18, 1: 16, 2: 14}
run.font.size = Pt(size_map.get(level, 16))
run.font.bold = bold
run.font.color.rgb = col
run.font.name = "Calibri"
# bullet symbol
pPr = p._pPr
if pPr is None:
pPr = p._p.get_or_add_pPr()
buChar = etree.SubElement(pPr, qn('a:buChar'))
if level == 0:
buChar.set('char', '▶')
elif level == 1:
buChar.set('char', '•')
else:
buChar.set('char', '–')
buFont = etree.SubElement(pPr, qn('a:buFont'))
buFont.set('typeface', 'Arial')
buSzPct = etree.SubElement(pPr, qn('a:buSzPct'))
buSzPct.set('val', '80000')
buClr = etree.SubElement(pPr, qn('a:buClr'))
srgbClr = etree.SubElement(buClr, qn('a:srgbClr'))
srgbClr.set('val', f'{MID_TEAL.rgb:06X}')
def section_divider(slide, section_name, subtitle=""):
"""Full-bleed section divider slide."""
add_rect(slide, 0, 0, 13.333, 7.5, DARK_TEAL)
add_rect(slide, 0, 3.2, 13.333, 0.1, AMBER)
add_textbox(slide, section_name, 1, 1.8, 11.333, 1.8,
font_size=46, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
if subtitle:
add_textbox(slide, subtitle, 1, 3.5, 11.333, 1.2,
font_size=22, bold=False, color=AMBER,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# ══════════════════════════════════════════════
# SLIDE 1 — TITLE
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_rect(slide, 0, 0, 13.333, 7.5, DARK_TEAL)
add_rect(slide, 0, 5.6, 13.333, 1.9, MID_TEAL)
add_rect(slide, 0, 2.85, 13.333, 0.12, AMBER)
add_textbox(slide, "INHERITED METABOLIC", 0.5, 0.8, 12.333, 1.1,
font_size=44, bold=True, color=WHITE, align=PP_ALIGN.CENTER)
add_textbox(slide, "DISORDERS OF THE LIVER", 0.5, 1.85, 12.333, 1.0,
font_size=44, bold=True, color=AMBER, align=PP_ALIGN.CENTER)
add_textbox(slide, "(Excluding Wilson Disease & Hemochromatosis)", 0.5, 3.1, 12.333, 0.7,
font_size=20, bold=False, color=RGBColor(0xC8,0xE8,0xEC), align=PP_ALIGN.CENTER)
add_textbox(slide, "A Comprehensive Clinical Review", 0.5, 5.8, 12.333, 0.6,
font_size=18, bold=False, color=WHITE, align=PP_ALIGN.CENTER)
add_textbox(slide, "Sources: Sleisenger & Fordtran's GI & Liver Disease | Robbins & Kumar Basic Pathology",
0.5, 6.5, 12.333, 0.6,
font_size=12, bold=False, color=RGBColor(0xAA,0xCC,0xCC), align=PP_ALIGN.CENTER)
# ══════════════════════════════════════════════
# SLIDE 2 — OVERVIEW / TABLE OF CONTENTS
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "Topics Covered", [
(0, "1. Overview & Clinical Approach to Inherited Metabolic Liver Disease", True, DARK_TEXT),
(0, "2. α1-Antitrypsin (α1-AT) Deficiency", False, DARK_TEXT),
(0, "3. Glycogen Storage Diseases (GSD Types I, III, IV)", False, DARK_TEXT),
(0, "4. Hereditary Tyrosinemia Type 1 (HT-1)", False, DARK_TEXT),
(0, "5. Congenital Disorders of Glycosylation (CDG)", False, DARK_TEXT),
(0, "6. Porphyrias & Hepatic Involvement", False, DARK_TEXT),
(0, "7. Other Metabolic Liver Disorders (Galactosemia, Fructosemia, Niemann-Pick, Gaucher)", False, DARK_TEXT),
(0, "8. Diagnostic Approach", False, DARK_TEXT),
(0, "9. Role of Liver Transplantation", False, DARK_TEXT),
(0, "10. Summary Table & Key Takeaways", False, DARK_TEXT),
])
# ══════════════════════════════════════════════
# SLIDE 3 — SECTION: OVERVIEW
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
section_divider(slide, "Overview & Clinical Approach",
"Inherited Metabolic Liver Disease — The Big Picture")
# ══════════════════════════════════════════════
# SLIDE 4 — EPIDEMIOLOGY & BURDEN
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "Why It Matters: Epidemiology & Burden", [
(0, "Definition", True, DARK_TEAL),
(1, "Genetic conditions where enzyme/transporter defects cause accumulation of toxic substrates or absence of essential products", False, DARK_TEXT),
(1, "Result: hepatocyte injury → inflammation → cirrhosis → HCC or liver failure", False, DARK_TEXT),
(0, "Transplant Burden", True, DARK_TEAL),
(1, "13% of all liver transplants in the USA are due to metabolic liver disease", False, DARK_TEXT),
(1, "~22% of pediatric liver transplants (2011–2013) were for metabolic/genetic liver disease", False, DARK_TEXT),
(0, "Onset", True, DARK_TEAL),
(1, "Neonatal/infantile: acute liver failure (tyrosinemia, GSD, urea cycle defects)", False, DARK_TEXT),
(1, "Childhood to adulthood: chronic hepatitis, cirrhosis, HCC (α1-AT, GSD III/IV)", False, DARK_TEXT),
(0, "Key principle: Disorders can mimic infection, intoxication, or other liver diseases — high index of suspicion required", True, RED_ACCENT),
])
# ══════════════════════════════════════════════
# SLIDE 5 — CLINICAL FEATURES (WHEN TO SUSPECT)
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "When to Suspect: Clinical Clues",
bullets=[
(0, "SYMPTOMS (Box 77.1 — Sleisenger & Fordtran's)", True, DARK_TEAL),
(1, "Coma, seizures, developmental delay, regression of milestones", False, DARK_TEXT),
(1, "Growth failure, recurrent vomiting", False, DARK_TEXT),
(1, "Hyperammonemic symptoms, hypoglycemic symptoms", False, DARK_TEXT),
],
sub_col2=[
(0, "SIGNS", True, DARK_TEAL),
(1, "Ascites, jaundice, hepatomegaly, splenomegaly", False, DARK_TEXT),
(1, "Kayser-Fleischer rings (Wilson – excluded here)", False, MID_GREY),
(1, "Rickets, dysmorphic features, cataracts", False, DARK_TEXT),
(0, "HISTORY CLUES", True, DARK_TEAL),
(1, "Consanguinity, multiple miscarriages, early infant deaths", False, DARK_TEXT),
(1, "Food-related symptom onset (galactosemia, fructosemia, UCD)", False, DARK_TEXT),
(1, "Dietary aversions", False, DARK_TEXT),
(0, "Elevated aminotransferases + any of above → immediate metabolic work-up", True, RED_ACCENT),
]
)
# ══════════════════════════════════════════════
# SLIDE 6 — SECTION: α1-AT DEFICIENCY
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
section_divider(slide, "α1-Antitrypsin (α1-AT) Deficiency",
"Most Common Genetic Liver Disease Requiring Liver Transplantation")
# ══════════════════════════════════════════════
# SLIDE 7 — α1-AT: GENETICS & MECHANISM
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "α1-AT Deficiency — Genetics & Pathophysiology", [
(0, "Genetics", True, DARK_TEAL),
(1, "Autosomal recessive; SERPINA1 gene (chromosome 14)", False, DARK_TEXT),
(1, "Most pathogenic allele: Z (Glu342Lys substitution) — PiZZ homozygotes most affected", False, DARK_TEXT),
(1, "2nd most common metabolic liver disease worldwide (after hemochromatosis)", False, DARK_TEXT),
(0, "Mechanism — Gain of Toxic Function (Liver)", True, DARK_TEAL),
(1, "Z-protein misfolds → forms intracellular polymers inside hepatocytes", False, DARK_TEXT),
(1, "Retention of misfolded protein → ER stress → hepatocyte injury → inflammation → fibrosis", False, DARK_TEXT),
(1, "NOT a deficiency disease for the liver — it is a TOXIC GAIN-OF-FUNCTION", False, DARK_TEXT),
(0, "Mechanism — Loss of Function (Lungs)", True, DARK_TEAL),
(1, "Reduced circulating α1-AT → uninhibited neutrophil elastase activity", False, DARK_TEXT),
(1, "Result: progressive pan-acinar emphysema, especially in smokers", False, DARK_TEXT),
(0, "α1-AT is an acute-phase reactant — levels can be NORMAL during inflammation/pregnancy in PiZZ!", True, RED_ACCENT),
])
# ══════════════════════════════════════════════
# SLIDE 8 — α1-AT: CLINICAL FEATURES & HISTOLOGY
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "α1-AT Deficiency — Clinical Features & Histology",
bullets=[
(0, "Liver Presentations (by age)", True, DARK_TEAL),
(1, "Neonatal: cholestasis, bile duct paucity, giant cell hepatitis", False, DARK_TEXT),
(1, "Child/adolescent: chronic hepatitis, hepatomegaly", False, DARK_TEXT),
(1, "Adult: cirrhosis, HCC (especially adult males)", False, DARK_TEXT),
(1, "Severe progressive liver disease more common in adult males", False, DARK_TEXT),
],
sub_col2=[
(0, "Histology — Key Feature", True, DARK_TEAL),
(1, "PAS-positive, diastase-RESISTANT globules in periportal hepatocytes", True, RED_ACCENT),
(1, "Most prominent in zone 1 (periportal) hepatocytes", False, DARK_TEXT),
(1, "Can also be seen in Kupffer cells", False, DARK_TEXT),
(1, "Confirmed with immunohistochemistry using anti-α1-AT Z monoclonal antibody", False, DARK_TEXT),
(0, "Other Features", True, DARK_TEAL),
(1, "Lung: emphysema (pan-acinar) — avoid smoking!", False, DARK_TEXT),
(1, "HCC surveillance: US every 6 months in cirrhotics (AASLD)", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 9 — α1-AT: DIAGNOSIS & TREATMENT
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "α1-AT Deficiency — Diagnosis & Treatment",
bullets=[
(0, "Diagnosis", True, DARK_TEAL),
(1, "Serum α1-AT PHENOTYPE analysis (not just level!) — PiZZ confirms", True, RED_ACCENT),
(1, "PCR for common alleles (Z, S)", False, DARK_TEXT),
(1, "Liver biopsy: PAS+ diastase-resistant globules", False, DARK_TEXT),
(1, "Molecular/sequence analysis for rare variants", False, DARK_TEXT),
(0, "Treatment — Liver Disease", True, DARK_TEAL),
(1, "NO approved disease-specific therapy for liver disease", True, RED_ACCENT),
(1, "Supportive: fat-soluble vitamins, adequate nutrition", False, DARK_TEXT),
(1, "Avoid alcohol, smoking, obesity, second-hand smoke", False, DARK_TEXT),
],
sub_col2=[
(0, "Emerging Therapies", True, DARK_TEAL),
(1, "siRNA: targets Z-variant mRNA, reduces intracellular accumulation", False, DARK_TEXT),
(1, "Autophagy enhancers: carbamazepine, rapamycin (clear misfolded protein)", False, DARK_TEXT),
(1, "CRISPR gene-editing strategies (preclinical)", False, DARK_TEXT),
(1, "Monoclonal antibodies to block Z-protein polymerization", False, DARK_TEXT),
(0, "Lung Disease Only", True, DARK_TEAL),
(1, "IV α1-AT augmentation therapy (FDA-approved for lung)", False, DARK_TEXT),
(1, "Does NOT help liver disease", True, RED_ACCENT),
(0, "Liver Transplantation", True, DARK_TEAL),
(1, "Most common genetic disease requiring LT", False, DARK_TEXT),
(1, "5-year survival: 83–90% (children & adults)", False, DARK_TEXT),
(1, "LT corrects both liver injury AND metabolic defect", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 10 — SECTION: GSDs
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
section_divider(slide, "Glycogen Storage Diseases (GSD)",
"Types I, III, and IV — The Three That Cause Serious Liver Disease")
# ══════════════════════════════════════════════
# SLIDE 11 — GSD: Overview
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "Glycogen Storage Diseases — Overview", [
(0, "More than 12 distinct inborn errors of glycogen metabolism exist", False, DARK_TEXT),
(0, "Only 3 cause clinically serious liver disease: GSD Types I, III, and IV", True, RED_ACCENT),
(0, "Incidence: 1 in 50,000–100,000 (combined types I, III, IV)", False, DARK_TEXT),
(0, "Glycogen Metabolism Essentials", True, DARK_TEAL),
(1, "Glycogen stores glucose in liver & muscle as energy reserve", False, DARK_TEXT),
(1, "Linear backbone: α-1,4 glycosidic bonds", False, DARK_TEXT),
(1, "Branching: 8–10% of glucose in α-1,6 linkage (branches every 8–10 residues)", False, DARK_TEXT),
(1, "Substrates: glucose-6-phosphate, glucose-1-phosphate", False, DARK_TEXT),
(0, "Tissues involved: liver (glucose homeostasis), muscle (energy), PMNs", False, DARK_TEXT),
(0, "Other GSDs may cause hepatomegaly or mild histologic changes but not clinically significant liver disease", False, MID_GREY),
])
# ══════════════════════════════════════════════
# SLIDE 12 — GSD TYPE I (von Gierke)
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "GSD Type I — Von Gierke Disease",
bullets=[
(0, "Enzyme Defect", True, DARK_TEAL),
(1, "Glucose-6-phosphatase (Type Ia) or translocase (Type Ib)", False, DARK_TEXT),
(1, "Gene: G6PC (Type Ia) or SLC37A4 (Type Ib)", False, DARK_TEXT),
(0, "Mechanism", True, DARK_TEAL),
(1, "Cannot release free glucose from liver → profound fasting hypoglycemia", False, DARK_TEXT),
(1, "Glucose-6-P accumulates → glycogen + fat build up in liver", False, DARK_TEXT),
(1, "Type Ib additionally: neutropenia + recurrent infections", False, DARK_TEXT),
(0, "Clinical Features", True, DARK_TEAL),
(1, "Massive hepatomegaly (glycogen + fat accumulation)", False, DARK_TEXT),
(1, "Severe fasting hypoglycemia (present in infancy)", False, DARK_TEXT),
(1, "Lactic acidosis, hyperuricemia, hyperlipidemia", False, DARK_TEXT),
],
sub_col2=[
(0, "Complications", True, DARK_TEAL),
(1, "Hepatic adenomas develop in 2nd–3rd decade → risk of HCC", True, RED_ACCENT),
(1, "Growth retardation, short stature", False, DARK_TEXT),
(1, "Renal enlargement, focal segmental glomerulosclerosis", False, DARK_TEXT),
(0, "Diagnosis", True, DARK_TEAL),
(1, "Fasting hypoglycemia + lactic acidosis + hepatomegaly → gene testing", False, DARK_TEXT),
(1, "Enzyme assay in liver biopsy or fibroblasts", False, DARK_TEXT),
(0, "Treatment", True, DARK_TEAL),
(1, "Frequent feeds; uncooked cornstarch (slow-release glucose)", True, GREEN_ACC),
(1, "Avoid fructose and galactose (converted to glucose-6-P)", False, DARK_TEXT),
(1, "Nocturnal nasogastric glucose infusion in infants", False, DARK_TEXT),
(1, "LT considered for uncontrolled metabolic disease or HCC", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 13 — GSD TYPE III (Cori / Forbes)
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "GSD Type III — Cori / Forbes Disease",
bullets=[
(0, "Enzyme Defect", True, DARK_TEAL),
(1, "Debranching enzyme (amylo-1,6-glucosidase)", False, DARK_TEXT),
(1, "Gene: AGL", False, DARK_TEXT),
(1, "AR inheritance", False, DARK_TEXT),
(0, "Mechanism", True, DARK_TEAL),
(1, "Cannot remove branch-point glucose → abnormal ('limit dextrin') glycogen accumulates", False, DARK_TEXT),
(1, "Glycogenolysis only partially effective", False, DARK_TEXT),
(0, "Clinical Features", True, DARK_TEAL),
(1, "Hepatomegaly (prominent in childhood)", False, DARK_TEXT),
(1, "Fasting hypoglycemia — milder than Type I", False, DARK_TEXT),
(1, "Myopathy (weakness, muscle cramps) — skeletal and cardiac", False, DARK_TEXT),
],
sub_col2=[
(0, "Prognosis", True, DARK_TEAL),
(1, "Liver disease often IMPROVES with age (unlike GSD IV)", True, GREEN_ACC),
(1, "Muscle involvement may persist and worsen", False, DARK_TEXT),
(1, "Rarely develops cirrhosis", False, DARK_TEXT),
(0, "Diagnosis", True, DARK_TEAL),
(1, "Enzyme assay (leucocytes or liver)", False, DARK_TEXT),
(1, "Molecular testing of AGL gene", False, DARK_TEXT),
(0, "Treatment", True, DARK_TEAL),
(1, "High-protein, frequent-feed diet", False, DARK_TEXT),
(1, "Protein intake helps via gluconeogenesis", False, DARK_TEXT),
(1, "Avoid prolonged fasting", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 14 — GSD TYPE IV (Andersen)
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "GSD Type IV — Andersen Disease",
bullets=[
(0, "Enzyme Defect", True, DARK_TEAL),
(1, "Branching enzyme (α-1,4-glucan:α-1,4-glucan 6-glucosyltransferase)", False, DARK_TEXT),
(1, "Gene: GBE1", False, DARK_TEXT),
(0, "Mechanism", True, DARK_TEAL),
(1, "Cannot form normal branch points → AMYLOPECTIN accumulates", False, DARK_TEXT),
(1, "Amylopectin = long, poorly branched glycogen — resembles plant starch", False, DARK_TEXT),
(1, "PAS-positive inclusions in hepatocytes", False, DARK_TEXT),
(0, "Clinical Features", True, DARK_TEAL),
(1, "Macronodular cirrhosis with amylopectin deposits", True, RED_ACCENT),
(1, "May progress to liver failure and rarely adenoma/HCC", False, DARK_TEXT),
(1, "Cardiomyopathy (amylopectin in heart)", False, DARK_TEXT),
],
sub_col2=[
(0, "Prognosis", True, DARK_TEAL),
(1, "Most die within first 3 years if untreated", True, RED_ACCENT),
(1, "High diet (protein, low carb) → improved growth but limited liver benefit", False, DARK_TEXT),
(0, "Treatment", True, DARK_TEAL),
(1, "Liver Transplantation: corrects metabolic error, normal growth in most", True, GREEN_ACC),
(1, "Caveat: Amylopectin may PERSIST in heart (progressive cardiomyopathy) after LT", True, RED_ACCENT),
(1, "Amylopectin also persists in leukocytes post-LT", False, DARK_TEXT),
(0, "Research", True, DARK_TEAL),
(1, "Adenoviral-mediated gene therapy: systemic correction achieved in mouse model", False, DARK_TEXT),
(1, "Human trials awaited", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 15 — SECTION: TYROSINEMIA
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
section_divider(slide, "Hereditary Tyrosinemia Type 1 (HT-1)",
"The Disease That Kills Fast — But Can Be Treated")
# ══════════════════════════════════════════════
# SLIDE 16 — HT-1: Genetics & Mechanism
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "Hereditary Tyrosinemia Type 1 — Genetics & Mechanism", [
(0, "Genetics", True, DARK_TEAL),
(1, "Autosomal recessive; deficiency of fumarylacetoacetate hydrolase (FAH)", False, DARK_TEXT),
(1, "FAH is the LAST enzyme in tyrosine catabolism", False, DARK_TEXT),
(0, "Toxic Metabolites", True, DARK_TEAL),
(1, "Fumarylacetoacetate (FAA) and maleylacetoacetate accumulate upstream", False, DARK_TEXT),
(1, "Converted to SUCCINYLACETONE (SA) and succinylacetoacetate (SAA)", False, DARK_TEXT),
(1, "SA + SAA directly injure hepatocytes and renal tubules", True, RED_ACCENT),
(1, "SA is a potent inhibitor of δ-aminolevulinic acid (ALA) dehydratase → blocks heme synthesis → porphyria-like neurologic crises", True, RED_ACCENT),
(0, "Secondary effects", True, DARK_TEAL),
(1, "Plasma tyrosine and methionine elevated (non-specific)", False, DARK_TEXT),
(1, "AFP markedly elevated (even before HCC develops — not useful for HCC diagnosis)", False, DARK_TEXT),
])
# ══════════════════════════════════════════════
# SLIDE 17 — HT-1: Clinical Features
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "HT-1 — Clinical Presentations",
bullets=[
(0, "ACUTE FORM (onset < 6 months)", True, RED_ACCENT),
(1, "Acute liver failure: coagulopathy, hypoglycemia, jaundice, ascites", False, DARK_TEXT),
(1, "Anorexia, vomiting, irritability", False, DARK_TEXT),
(1, "Elevated aminotransferases, GGTP, bilirubin, AFP", False, DARK_TEXT),
(1, "Urine: SA, SAA, ALA, phosphaturia, glucosuria, aminoaciduria", False, DARK_TEXT),
(1, "77% present before 6 months of age", True, RED_ACCENT),
(1, "1-yr survival (0–2 months): 38% | (2–6 months): 74% | (>6 months): 96%", True, RED_ACCENT),
],
sub_col2=[
(0, "CHRONIC FORM (onset > 1 year)", True, DARK_TEAL),
(1, "Hepatomegaly, milder hepatic dysfunction", False, DARK_TEXT),
(1, "Rickets (phosphaturia → hypophosphatemia)", False, DARK_TEXT),
(1, "Nephromegaly, hypertension, growth retardation", False, DARK_TEXT),
(1, "Fanconi syndrome (proximal RTA)", False, DARK_TEXT),
(0, "Complications", True, DARK_TEAL),
(1, "HCC: high risk even before cirrhosis (large/small cell dysplasia)", True, RED_ACCENT),
(1, "Cardiomyopathy (septal hypertrophy) in ~1/3 — reversible with treatment", False, DARK_TEXT),
(1, "Neurologic crises: porphyria-like, autonomic + motor neuropathy", True, RED_ACCENT),
(1, "Developmental delay, attention deficit disorders", False, DARK_TEXT),
(1, "Renal failure → may need renal transplantation", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 18 — HT-1: Diagnosis & Treatment
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "HT-1 — Diagnosis & Treatment",
bullets=[
(0, "Diagnosis", True, DARK_TEAL),
(1, "Urine succinylacetone (SA) — PATHOGNOMONIC", True, RED_ACCENT),
(1, "Elevated plasma tyrosine, methionine, AFP", False, DARK_TEXT),
(1, "FAH enzyme assay: liver, fibroblasts, or erythrocytes", False, DARK_TEXT),
(1, "Molecular testing: FAH gene mutations", False, DARK_TEXT),
(1, "Newborn screening: SA detectable on dried blood spot (tandem MS)", False, DARK_TEXT),
(0, "Histopathology", True, DARK_TEAL),
(1, "Acute: enlarged pale nodular liver or shrunken brown liver", False, DARK_TEXT),
(1, "Micronodular cirrhosis, steatosis, bile duct proliferation", False, DARK_TEXT),
(1, "Chronic: macronodular cirrhosis, large/small cell dysplasia", False, DARK_TEXT),
],
sub_col2=[
(0, "Treatment — NITISINONE (NTBC)", True, GREEN_ACC),
(1, "Mechanism: inhibits 4-hydroxyphenylpyruvate dioxygenase (4-HPPD) — upstream of FAH", False, DARK_TEXT),
(1, "Prevents formation of toxic SA and SAA", False, DARK_TEXT),
(1, "Dramatically improves survival — standard of care", True, GREEN_ACC),
(1, "Side effects: elevated plasma tyrosine → diet restriction required", False, DARK_TEXT),
(0, "Diet", True, DARK_TEAL),
(1, "Low-tyrosine, low-phenylalanine diet", False, DARK_TEXT),
(1, "Prevents tyrosine crystalline deposits in cornea/skin", False, DARK_TEXT),
(0, "Liver Transplantation", True, DARK_TEAL),
(1, "Curative — if NTBC fails, HCC develops, or end-stage disease", False, DARK_TEXT),
(1, "Corrects metabolic defect and prevents further SA production", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 19 — SECTION: CDG
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
section_divider(slide, "Congenital Disorders of Glycosylation (CDG)",
"Over 130 Disorders — Hepatic Involvement in ~22%")
# ══════════════════════════════════════════════
# SLIDE 20 — CDG: Overview & Liver
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "CDG — Overview & Hepatic Involvement",
bullets=[
(0, "Definition", True, DARK_TEAL),
(1, "Inherited defects in glycan synthesis on glycoproteins — affects all organ systems", False, DARK_TEXT),
(1, ">130 CDG types involving N-linked and O-linked protein glycosylation", False, DARK_TEXT),
(0, "Classification", True, DARK_TEAL),
(1, "Group I: disorders of lipid-linked oligosaccharide assembly (before transfer to protein)", False, DARK_TEXT),
(1, "Group II: disorders of protein-bound oligosaccharide processing", False, DARK_TEXT),
(0, "Liver Involvement", True, DARK_TEAL),
(1, "Present in ~22% of CDG patients", False, DARK_TEXT),
(1, "Usually mild: steatosis + fibrosis on light microscopy", False, DARK_TEXT),
(1, "Electron microscopy: MYELOSOMES — lysosomal vacuoles with concentric electron-dense membranes", True, RED_ACCENT),
(1, "Uncommonly progresses to cirrhosis and liver failure", False, DARK_TEXT),
],
sub_col2=[
(0, "Affected Glycoproteins (clinical relevance)", True, DARK_TEAL),
(1, "Coagulation factors → coagulopathy (both pro- and anti-coagulant)", True, RED_ACCENT),
(1, "Albumin, apolipoproteins, growth hormone, insulin, thyroxine-binding globulin", False, DARK_TEXT),
(0, "Key Screening Test", True, DARK_TEAL),
(1, "Serum TRANSFERRIN isoelectric focusing — detects N-glycosylation defects", True, GREEN_ACC),
(1, "Advanced mass spectrometry for confirmation", False, DARK_TEXT),
(0, "When to Screen for CDG", True, DARK_TEAL),
(1, "Unexplained congenital hepatic fibrosis", False, DARK_TEXT),
(1, "Protein-losing enteropathy", False, DARK_TEXT),
(1, "Pro-coagulant or anticoagulant tendency without clear cause", False, DARK_TEXT),
(1, "Multisystem disease dominated by CNS features", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 21 — CDG TYPES Ia, Ib, Ic
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "CDG — Key Types with Liver Involvement",
bullets=[
(0, "CDG Type Ia — PMM2-CDG (most common CDG)", True, DARK_TEAL),
(1, "Enzyme: phosphomannomutase 2 (PMM2)", False, DARK_TEXT),
(1, "Features: psychomotor retardation, cerebellar hypoplasia, hepatomegaly, coagulopathy, protein-losing enteropathy", False, DARK_TEXT),
(1, "No specific treatment; supportive care", False, DARK_TEXT),
(0, "CDG Type Ib — MPI-CDG (ONLY TREATABLE FORM)", True, GREEN_ACC),
(1, "Enzyme: phosphomannose isomerase (MPI)", False, DARK_TEXT),
(1, "Features: intractable diarrhea, protein-losing enteropathy, congenital hepatic fibrosis, hyperinsulinemic hypoglycemia, cyclic vomiting", False, DARK_TEXT),
(1, "Usually NO neurological features (key differentiator from Type Ia)", True, GREEN_ACC),
(1, "Treatment: ORAL MANNOSE supplementation — effective; liver fibrosis may persist", True, GREEN_ACC),
],
sub_col2=[
(0, "CDG Type Ic — ALG6-CDG", True, DARK_TEAL),
(1, "Transient hepatomegaly without congenital hepatic fibrosis", False, DARK_TEXT),
(1, "Otherwise milder than Type Ia", False, DARK_TEXT),
(0, "CDG Type Ih — ALG8-CDG", True, DARK_TEAL),
(1, "Protein-losing enteropathy with chronic diarrhea", False, DARK_TEXT),
(1, "Hepatic fibrosis, variable hepatic dysfunction", False, DARK_TEXT),
(0, "Group II CDGs", True, DARK_TEAL),
(1, "Marked dysmorphic features, severe developmental delay", False, DARK_TEXT),
(1, "Hepatosplenomegaly, progressive jaundice, epilepsy in some", False, DARK_TEXT),
(1, "Progressive cirrhosis reported with normal hepatic excretory/synthetic function", False, DARK_TEXT),
(0, "LT has been beneficial in select CDG Ib patients with full clinical recovery", False, GREEN_ACC),
]
)
# ══════════════════════════════════════════════
# SLIDE 22 — SECTION: PORPHYRIAS
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
section_divider(slide, "Porphyrias",
"Heme Synthesis Defects — Hepatic Involvement")
# ══════════════════════════════════════════════
# SLIDE 23 — PORPHYRIAS: Overview & Classification
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "Porphyrias — Overview & Classification",
bullets=[
(0, "Definition", True, DARK_TEAL),
(1, "Defects in enzymes of the heme biosynthesis pathway (8 steps, 8 types)", False, DARK_TEXT),
(1, "Each porphyria corresponds to a specific enzyme deficiency", False, DARK_TEXT),
(0, "Classification", True, DARK_TEAL),
(1, "HEPATIC porphyrias: precursors accumulate in liver → liver disease + systemic symptoms", False, DARK_TEXT),
(1, "ERYTHROPOIETIC porphyrias: accumulation in bone marrow → photosensitivity", False, DARK_TEXT),
(0, "ACUTE porphyrias (neurovisceral symptoms)", True, RED_ACCENT),
(1, "Acute Intermittent Porphyria (AIP) — most common acute type", False, DARK_TEXT),
(1, "ALA dehydratase deficiency porphyria (ADD) — rare", False, DARK_TEXT),
(1, "Hereditary coproporphyria (HCP), Variegate porphyria (VP)", False, DARK_TEXT),
],
sub_col2=[
(0, "CUTANEOUS porphyrias", True, DARK_TEAL),
(1, "Porphyria cutanea tarda (PCT) — most common overall", False, DARK_TEXT),
(1, "Congenital erythropoietic porphyria (CEP)", False, DARK_TEXT),
(1, "Erythropoietic protoporphyria (EPP)", False, DARK_TEXT),
(0, "Triggers for Acute Attacks", True, RED_ACCENT),
(1, "Drugs (barbiturates, sulfonamides, estrogens, rifampicin, griseofulvin)", False, DARK_TEXT),
(1, "Fasting / low-carbohydrate diets", False, DARK_TEXT),
(1, "Hormonal changes (luteal phase, pregnancy)", False, DARK_TEXT),
(1, "Infections, stress", False, DARK_TEXT),
(0, "Hepatic risk in porphyrias: elevated HCC risk (particularly in AIP and PCT)", True, RED_ACCENT),
]
)
# ══════════════════════════════════════════════
# SLIDE 24 — AIP & PCT
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "AIP & Porphyria Cutanea Tarda — Key Points",
bullets=[
(0, "Acute Intermittent Porphyria (AIP)", True, DARK_TEAL),
(1, "Enzyme: porphobilinogen deaminase (PBGD) — haploinsufficiency (AD)", False, DARK_TEXT),
(1, "ALA and porphobilinogen (PBG) accumulate", False, DARK_TEXT),
(1, "Triad: abdominal pain + autonomic instability + neuropsychiatric symptoms", True, RED_ACCENT),
(1, "Urine turns red/brown on standing (porphyrins)", False, DARK_TEXT),
(1, "Diagnosis: elevated urinary ALA and PBG during attack", False, DARK_TEXT),
(1, "Treatment: IV glucose (suppress ALA synthase) + IV hemin (givosiran for prevention)", False, DARK_TEXT),
(1, "LT cures the metabolic defect in severe refractory AIP", False, DARK_TEXT),
],
sub_col2=[
(0, "Porphyria Cutanea Tarda (PCT)", True, DARK_TEAL),
(1, "Enzyme: uroporphyrinogen decarboxylase (UROD)", False, DARK_TEXT),
(1, "Most common porphyria overall", False, DARK_TEXT),
(1, "ASSOCIATED WITH: HCV infection, alcohol, HFE mutations, estrogens, HIV", True, RED_ACCENT),
(1, "Uroporphyrin accumulates → excreted in urine (fluorescent pink)", False, DARK_TEXT),
(1, "Skin: blistering photosensitivity on sun-exposed areas, fragile skin, hyperpigmentation, hypertrichosis", False, DARK_TEXT),
(1, "HCC risk elevated in liver disease + PCT", False, DARK_TEXT),
(0, "PCT Treatment", True, GREEN_ACC),
(1, "Phlebotomy (remove iron; iron activates porphyria)", False, DARK_TEXT),
(1, "Hydroxychloroquine (chelates porphyrins; low-dose)", False, DARK_TEXT),
(1, "Treat underlying HCV if present", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 25 — SECTION: OTHER DISORDERS
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
section_divider(slide, "Other Inherited Metabolic Liver Disorders",
"Galactosemia | Fructosemia | Niemann-Pick | Gaucher Disease")
# ══════════════════════════════════════════════
# SLIDE 26 — Galactosemia & Fructosemia
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "Galactosemia & Hereditary Fructose Intolerance",
bullets=[
(0, "GALACTOSEMIA (Classic)", True, DARK_TEAL),
(1, "Enzyme: GALT (galactose-1-phosphate uridylyltransferase) — AR", False, DARK_TEXT),
(1, "Galactose-1-phosphate accumulates → toxic to liver, brain, kidneys, ovaries", False, DARK_TEXT),
(1, "Presents with neonatal jaundice, liver failure, E. coli sepsis", True, RED_ACCENT),
(1, "Feature: cataracts (galactitol deposits in lens)", False, DARK_TEXT),
(1, "Diagnosis: GALT enzyme assay on RBCs; newborn screen (elevated galactose)", False, DARK_TEXT),
(1, "Treatment: eliminate lactose and galactose from diet immediately", True, GREEN_ACC),
(1, "Residual complications despite diet: ovarian failure (in females), developmental delay", False, DARK_TEXT),
],
sub_col2=[
(0, "HEREDITARY FRUCTOSE INTOLERANCE (HFI)", True, DARK_TEAL),
(1, "Enzyme: aldolase B (fructose-1-phosphate aldolase) — AR", False, DARK_TEXT),
(1, "Fructose-1-phosphate accumulates → sequesters inorganic phosphate → ATP depletion → hepatocyte necrosis", False, DARK_TEXT),
(1, "Presents when fructose/sucrose introduced into diet (infant formula, fruits)", False, DARK_TEXT),
(1, "Symptoms: vomiting, hypoglycemia, jaundice, liver failure after fructose ingestion", True, RED_ACCENT),
(1, "Key clue: strong aversion to sweets (instinctive avoidance)", True, RED_ACCENT),
(1, "Diagnosis: molecular testing (ALDOB gene); avoid fructose loading test (dangerous)", False, DARK_TEXT),
(1, "Treatment: eliminate fructose, sucrose, and sorbitol from diet", True, GREEN_ACC),
(1, "If diet maintained: excellent prognosis, liver recovers", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 27 — Niemann-Pick & Gaucher Disease
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "Niemann-Pick Disease & Gaucher Disease",
bullets=[
(0, "NIEMANN-PICK DISEASE", True, DARK_TEAL),
(1, "Type A & B: sphingomyelinase deficiency → sphingomyelin accumulates in lysosomes", False, DARK_TEXT),
(1, "Type C: NPC1/NPC2 protein defect → impaired cholesterol trafficking", False, DARK_TEXT),
(1, "Liver: hepatomegaly, 'foam cells' (lipid-laden macrophages/Kupffer cells) → fibrosis", False, DARK_TEXT),
(1, "Type A: severe neurodegeneration, death by age 3", False, DARK_TEXT),
(1, "Type B: hepatosplenomegaly, lung disease, NO neurological involvement → longer survival", False, DARK_TEXT),
(1, "Type C: progressive neurological disease + hepatosplenomegaly", False, DARK_TEXT),
(1, "Type B Treatment: IV enzyme replacement therapy (ERT) with olipudase alfa", True, GREEN_ACC),
(1, "Type C Treatment: miglustat (substrate reduction therapy)", False, DARK_TEXT),
],
sub_col2=[
(0, "GAUCHER DISEASE (Type 1 — Most Common)", True, DARK_TEAL),
(1, "Enzyme: β-glucocerebrosidase (glucosylceramidase) — AR; GBA gene", False, DARK_TEXT),
(1, "Glucocerebroside accumulates in macrophages (Gaucher cells — 'crumpled paper' cytoplasm)", False, DARK_TEXT),
(1, "Liver: hepatomegaly, Gaucher cells in sinusoids → fibrosis, portal hypertension", False, DARK_TEXT),
(1, "Splenomegaly (massive) + bone marrow infiltration → cytopenias", False, DARK_TEXT),
(1, "Type 1: NO neurological disease — most common, manageable", True, GREEN_ACC),
(1, "Type 2 & 3: neurological involvement (more severe)", False, DARK_TEXT),
(0, "Gaucher Treatment", True, GREEN_ACC),
(1, "ERT: imiglucerase / velaglucerase alfa / taliglucerase alfa (IV infusion)", True, GREEN_ACC),
(1, "SRT: miglustat or eliglustat (oral; substrate reduction)", False, DARK_TEXT),
(1, "ERT highly effective for liver/spleen/bone; does not cross BBB", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 28 — SECTION: DIAGNOSTIC APPROACH
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
section_divider(slide, "Diagnostic Approach",
"A Systematic Work-Up for Inherited Metabolic Liver Disease")
# ══════════════════════════════════════════════
# SLIDE 29 — DIAGNOSTIC APPROACH (full)
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_bullet_slide(slide, "Diagnostic Work-Up — Step by Step",
bullets=[
(0, "STEP 1 — History", True, DARK_TEAL),
(1, "Family history: consanguinity, unexplained infant deaths, miscarriages", False, DARK_TEXT),
(1, "Symptom onset related to food introduction (galactosemia, HFI, UCD)", False, DARK_TEXT),
(1, "Dietary aversions (instinctive avoidance of sweets in HFI)", False, DARK_TEXT),
(0, "STEP 2 — Initial Screening Labs", True, DARK_TEAL),
(1, "LFTs, coagulation, glucose, ammonia, lactate, uric acid", False, DARK_TEXT),
(1, "Plasma amino acids, urine organic acids, acylcarnitine profile", False, DARK_TEXT),
(1, "Serum iron studies (if hemochromatosis considered)", False, DARK_TEXT),
(1, "α1-AT phenotype, ceruloplasmin + urinary copper", False, DARK_TEXT),
(0, "KEY RULE: Obtain samples DURING the acute episode — many values normalize between attacks", True, RED_ACCENT),
],
sub_col2=[
(0, "STEP 3 — Specific Tests", True, DARK_TEAL),
(1, "Urine succinylacetone → tyrosinemia type 1", False, DARK_TEXT),
(1, "Serum transferrin IEF → CDG", False, DARK_TEXT),
(1, "Urine porphyrins / ALA / PBG → porphyria", False, DARK_TEXT),
(1, "GALT RBC enzyme assay → galactosemia", False, DARK_TEXT),
(1, "β-glucocerebrosidase assay → Gaucher", False, DARK_TEXT),
(1, "GBA / FAH / GBE1 / AGL / G6PC molecular testing", False, DARK_TEXT),
(0, "STEP 4 — Liver Biopsy", True, DARK_TEAL),
(1, "Standard histology + FROZEN specimen (biochemical assay)", True, RED_ACCENT),
(1, "Electron microscopy: organelle changes (myelosomes in CDG; mitochondrial changes)", False, DARK_TEXT),
(1, "PAS staining: glycogen (GSD), PAS+ globules (α1-AT)", False, DARK_TEXT),
(0, "STEP 5 — Molecular Genetic Testing", True, DARK_TEAL),
(1, "Provides genotypic confirmation; essential for family counseling", False, DARK_TEXT),
(1, "NGS panels now available for comprehensive metabolic liver disease", False, DARK_TEXT),
]
)
# ══════════════════════════════════════════════
# SLIDE 30 — SUMMARY TABLE & KEY TAKEAWAYS
# ══════════════════════════════════════════════
slide = prs.slides.add_slide(blank_layout)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_TEAL)
add_rect(slide, 0, 0, 13.333, 1.1, DARK_TEAL)
add_rect(slide, 0, 1.1, 13.333, 0.06, AMBER)
add_textbox(slide, "Summary — Key Takeaways", 0.35, 0.1, 12.5, 0.95,
font_size=30, bold=True, color=WHITE,
align=PP_ALIGN.LEFT, v_anchor=MSO_ANCHOR.MIDDLE)
# Table data
headers = ["Disease", "Defect", "Key Feature", "Hallmark Dx Test", "Treatment"]
rows = [
["α1-AT Def.", "SERPINA1 / Z-protein misfolding", "PAS+ periportal globules; cirrhosis/HCC", "Phenotype (PiZZ); liver biopsy", "Supportive; LT"],
["GSD Type I", "G6Pase (G6PC)", "Hypoglycemia + lactic acidosis; adenomas", "Enzyme assay; G6PC gene", "Cornstarch diet"],
["GSD Type III", "Debrancher (AGL)", "Hepatomegaly + myopathy; improves with age", "AGL enzyme / gene", "High protein diet"],
["GSD Type IV", "Brancher (GBE1)", "Amylopectin deposits; cirrhosis by age 3", "Liver biopsy (PAS+); GBE1 gene", "LT (cardiac risk)"],
["Tyrosinemia 1", "FAH", "ALF / HCC; porphyria-like crises", "Urine succinylacetone (patho)", "Nitisinone + low-Tyr diet; LT"],
["CDG Type Ib", "Phosphomannose isomerase", "Hepatic fibrosis; protein-losing enteropathy", "Transferrin IEF", "Oral mannose"],
["PCT", "UROD", "Blistering photosensitivity; HCV-related", "Urine/plasma porphyrins", "Phlebotomy / hydroxychloroquine"],
["Galactosemia", "GALT", "Neonatal ALF; cataracts; E. coli sepsis", "RBC GALT assay; newborn screen", "Lactose-free diet"],
["HFI", "Aldolase B", "Symptoms after fructose; sweet aversion", "ALDOB gene testing", "Fructose-free diet"],
["Gaucher (T1)", "β-glucocerebrosidase", "Hepatosplenomegaly; Gaucher cells", "Leukocyte enzyme assay; GBA gene", "ERT (imiglucerase)"],
]
col_widths = [1.5, 2.1, 3.0, 2.4, 2.1]
col_starts = [0.25]
for w in col_widths[:-1]:
col_starts.append(col_starts[-1] + w)
row_h = 0.52
table_top = 1.22
# Header row
for ci, (hdr, cw, cx) in enumerate(zip(headers, col_widths, col_starts)):
add_rect(slide, cx, table_top, cw - 0.05, row_h, MID_TEAL)
add_textbox(slide, hdr, cx + 0.05, table_top + 0.05, cw - 0.1, row_h - 0.1,
font_size=11, bold=True, color=WHITE, align=PP_ALIGN.CENTER,
v_anchor=MSO_ANCHOR.MIDDLE)
for ri, row in enumerate(rows):
y = table_top + row_h * (ri + 1)
bg = RGBColor(0xD4, 0xEE, 0xF1) if ri % 2 == 0 else WHITE
for ci, (cell, cw, cx) in enumerate(zip(row, col_widths, col_starts)):
add_rect(slide, cx, y, cw - 0.05, row_h, bg)
add_textbox(slide, cell, cx + 0.04, y + 0.02, cw - 0.1, row_h - 0.04,
font_size=9.5, bold=False, color=DARK_TEXT,
align=PP_ALIGN.LEFT, v_anchor=MSO_ANCHOR.MIDDLE)
# ─── Save ───
output_path = "/tmp/workspace/metabolic-liver-pptx/Inherited_Metabolic_Liver_Disorders.pptx"
prs.save(output_path)
print(f"Saved: {output_path}")
print(f"Total slides: {len(prs.slides)}")
Running Command
cd /tmp/workspace/metabolic-liver-pptx && python create_pptx.py 2>&1
Editing File
~/metabolic-liver-pptx/create_pptx.py
Successfully replaced 1 instance(s) of the string in '/tmp/workspace/metabolic-liver-pptx/create_pptx.py'
Running Command
cd /tmp/workspace/metabolic-liver-pptx && python create_pptx.py 2>&1
Your presentation is ready - exactly 30 slides, built from Sleisenger & Fordtran's and Robbins & Kumar content.
Inherited Metabolic Liver Disorders
Presentation · PPTX
Slide structure (30 slides):
| # | Slide |
|---|---|
| 1 | Title slide |
| 2 | Table of Contents |
| 3 | Section divider — Overview |
| 4 | Epidemiology & Burden |
| 5 | Clinical Clues — When to Suspect |
| 6 | Section divider — α1-AT Deficiency |
| 7 | α1-AT: Genetics & Pathophysiology |
| 8 | α1-AT: Clinical Features & Histology (PAS+ globules) |
| 9 | α1-AT: Diagnosis & Treatment (emerging siRNA/CRISPR) |
| 10 | Section divider — Glycogen Storage Diseases |
| 11 | GSD Overview |
| 12 | GSD Type I — Von Gierke (cornstarch diet) |
| 13 | GSD Type III — Cori/Forbes Disease |
| 14 | GSD Type IV — Andersen (amylopectin, LT caveat) |
| 15 | Section divider — Tyrosinemia Type 1 |
| 16 | HT-1: Genetics & Succinylacetone mechanism |
| 17 | HT-1: Acute vs Chronic presentations |
| 18 | HT-1: Nitisinone (NTBC) treatment |
| 19 | Section divider — CDG |
| 20 | CDG: Overview & Hepatic Involvement |
| 21 | CDG Types Ia, Ib (only treatable form - oral mannose), Ic |
| 22 | Section divider — Porphyrias |
| 23 | Porphyria Classification & Triggers |
| 24 | AIP & PCT (phlebotomy / hydroxychloroquine) |
| 25 | Section divider — Other Disorders |
| 26 | Galactosemia & Hereditary Fructose Intolerance |
| 27 | Niemann-Pick & Gaucher Disease (ERT) |
| 28 | Section divider — Diagnostic Approach |
| 29 | Step-by-step diagnostic work-up |
| 30 | Master Summary Table (all 10 disorders) |
Design uses a dark teal/amber medical colour scheme with 2-column layouts on complex slides.
This is a shared conversation. Sign in to Orris to start your own chat.