BRACHIAL PLEXUS FOR EMERGENCY MEDICINE DETAIL , AND BREAK
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data. Let me compile the full, detailed, well-organized answer.
🧠 BRACHIAL PLEXUS — Emergency Medicine Deep Dive
📍 OVERVIEW
The brachial plexus is a somatic nerve network formed from the anterior rami of C5–C8 and T1, occasionally with contributions from C4 (prefixed) or T2 (postfixed). It originates in the neck between the anterior and middle scalene muscles, crosses over the first rib, and enters the axilla — supplying all motor and most sensory innervation to the upper limb.
Gray's Anatomy for Students, p. 858–861
🏗️ STRUCTURE: The "RTDC" Memory System
The plexus has 4 sequential levels — Roots → Trunks → Divisions → Cords → Branches
Mnemonic: "Robert Taylor Drinks Cold Beer" (Roots, Trunks, Divisions, Cords, Branches)
LEVEL 1 — ROOTS (Anterior Rami)
| Root | Exits Between |
|---|---|
| C5 | Between anterior & middle scalene |
| C6 | Between anterior & middle scalene |
| C7 | Between anterior & middle scalene |
| C8 | Between anterior & middle scalene |
| T1 | Over rib I, posterior to subclavian artery |
Each root receives gray rami communicantes from the sympathetic trunk (carries postganglionic sympathetic fibers). This is clinically important — T1 root injury → Horner syndrome (ptosis, miosis, anhidrosis, enophthalmos).
LEVEL 2 — TRUNKS (3)
| Trunk | Formed By | Position |
|---|---|---|
| Superior (Upper) | C5 + C6 | Superior |
| Middle | C7 alone | Middle |
| Inferior (Lower) | C8 + T1 | Posterior to subclavian artery, on rib I |
The trunks cross the base of the posterior triangle of the neck.
Gray's Anatomy for Students, p. 858
LEVEL 3 — DIVISIONS (6 total)
Each trunk splits into anterior and posterior divisions.
- Anterior divisions → supply anterior (flexor) compartments
- Posterior divisions → supply posterior (extensor) compartments
- No named nerves arise directly from divisions
LEVEL 4 — CORDS (3)
Named by their position relative to the axillary artery (2nd part):
| Cord | Origin | Contributions | Position |
|---|---|---|---|
| Lateral cord | Anterior divisions of superior + middle trunks | C5, C6, C7 | Lateral to axillary artery |
| Medial cord | Anterior division of inferior trunk | C8, T1 | Medial to axillary artery |
| Posterior cord | All 3 posterior divisions | C5–T1 (all) | Posterior to axillary artery |
🔱 BRANCHES (The 5 Terminal Nerves + Pre-terminal Branches)
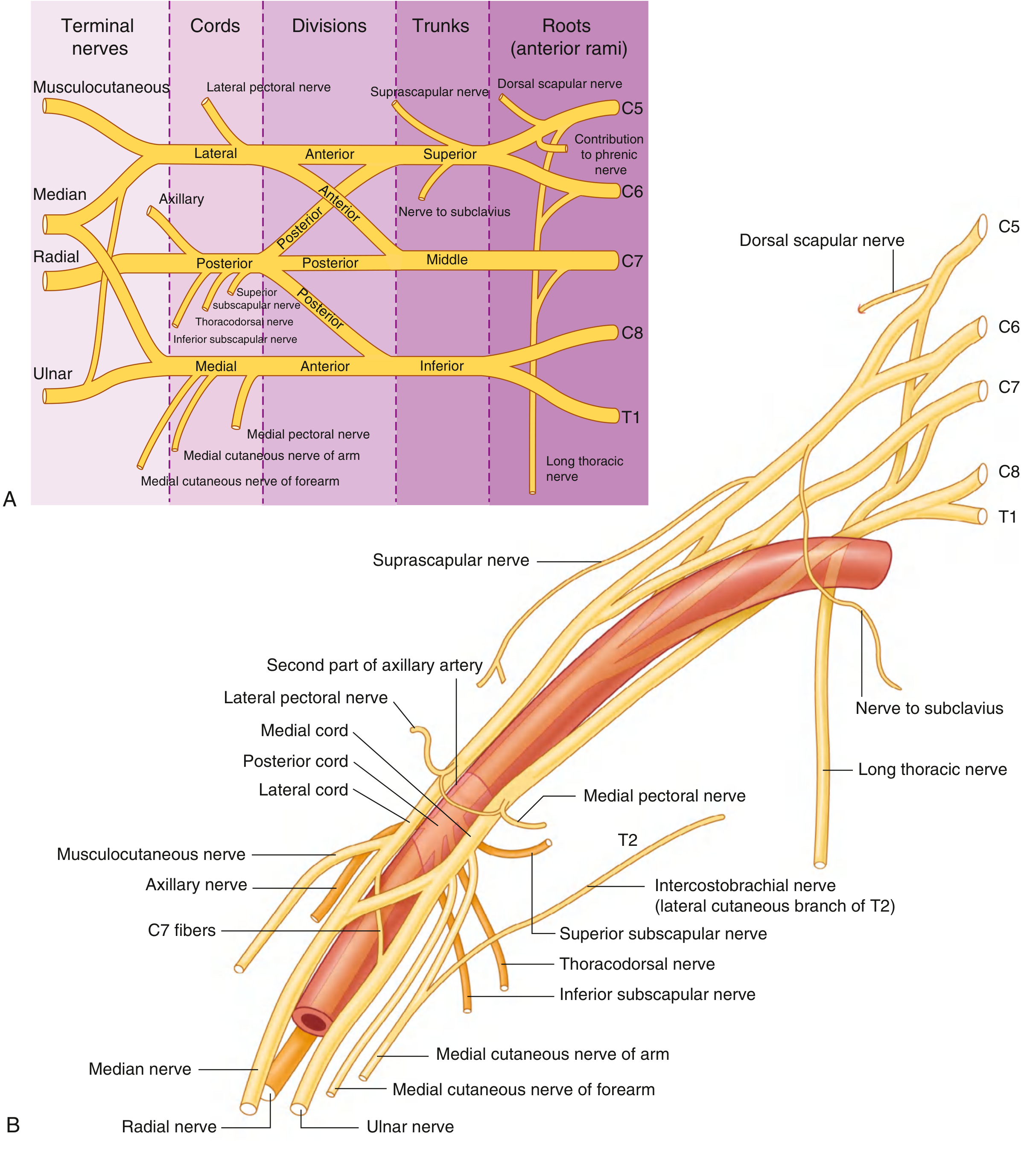
Fig. 7.53 Brachial Plexus — Schematic (A) and relationship to axillary artery (B). Gray's Anatomy for Students, p. 860
FROM THE ROOTS
| Nerve | Roots | Muscles |
|---|---|---|
| Dorsal scapular nerve | C5 | Rhomboid major & minor |
| Long thoracic nerve | C5, C6, C7 | Serratus anterior |
| Contribution to phrenic nerve | C5 | Diaphragm (partial) |
EM pearl: Long thoracic nerve injury → winged scapula (serratus anterior paralysis). Seen in blunt chest trauma, backpack compression, or radical neck dissection.
FROM THE TRUNKS (Superior trunk only)
| Nerve | Roots | Muscles |
|---|---|---|
| Suprascapular nerve | C5, C6 | Supraspinatus, Infraspinatus |
| Nerve to subclavius | C5, C6 | Subclavius |
FROM THE LATERAL CORD
| Nerve | Notes |
|---|---|
| Lateral pectoral nerve | Pectoralis major |
| Musculocutaneous nerve (C5–C7) | Coracobrachialis, biceps, brachialis → becomes lateral cutaneous nerve of forearm |
| Lateral root of median nerve | Joins medial root to form median nerve |
FROM THE MEDIAL CORD
| Nerve | Notes |
|---|---|
| Medial pectoral nerve | Pectoralis minor + major |
| Medial cutaneous nerve of arm | Skin, medial arm |
| Medial cutaneous nerve of forearm | Skin, medial forearm |
| Medial root of median nerve | Joins lateral root → median nerve |
| Ulnar nerve (C8, T1) | Terminal branch |
FROM THE POSTERIOR CORD
| Nerve | Roots | Key Targets |
|---|---|---|
| Upper subscapular nerve | C5, C6 | Subscapularis (upper) |
| Thoracodorsal nerve | C6–C8 | Latissimus dorsi |
| Lower subscapular nerve | C5, C6 | Subscapularis (lower), teres major |
| Axillary nerve | C5, C6 | Deltoid, teres minor, lateral cutaneous nerve of arm |
| Radial nerve | C5–T1 | All posterior compartment muscles of arm + forearm |
Gray's Anatomy for Students, p. 860–861
📊 COMPLETE PLEXUS DIAGRAM

Fig. 7.52 Brachial Plexus. Major components in neck and axilla. Gray's Anatomy for Students, p. 858
🚨 INJURIES — EMERGENCY MEDICINE BREAKDOWN
CLASSIFICATION: Seddon & Sunderland
| Seddon | Sunderland | Pathology | Prognosis |
|---|---|---|---|
| Neuropraxia | Grade I | Myelin injury only, axon intact, conduction block | Full spontaneous recovery (days–weeks) |
| Axonotmesis | Grade II | Axon + myelin disrupted, endoneurium intact | Recovery by regeneration (1 mm/day) |
| Axonotmesis | Grade III | Axon + endoneurium disrupted, perineurium intact | Incomplete recovery likely |
| Axonotmesis | Grade IV | All except epineurium disrupted | Poor recovery without surgery |
| Neurotmesis | Grade V | Complete nerve division | No recovery without surgical repair |
EM pearl: Grades III–V require surgical referral. Surgical repair ideally within 1–2 months to prevent irreversible denervation changes.
- Rockwood and Green's Fractures in Adults, 10th Ed., 2025
INJURY PATTERN 1 — ERB-DUCHENNE PALSY (Upper Trunk: C5–C6)
Mechanism:
- Adults: fall from motorcycle, weight on shoulder, shoulder-neck angle forcefully widened
- Neonates: shoulder dystocia, difficult delivery
Roots injured: C5, C6 (±C4)
Muscles paralyzed: Deltoid, biceps, brachialis, brachioradialis, supinator
Classic posture: "Waiter's tip" / "Policeman taking a tip"
- Arm: adducted + internally rotated
- Elbow: extended
- Forearm: pronated
- Wrist: flexed
Sensory loss: Lateral arm and upper lateral forearm (C5, C6 dermatomes)
Prognosis: Best prognosis of all brachial plexus injuries. Most common type (~90% of neonatal injuries).
S. Das Manual of Clinical Surgery, 13th Ed., p. 140; Miller's Review of Orthopaedics, 9th Ed., p. 260
INJURY PATTERN 2 — KLUMPKE'S PALSY (Lower Trunk: C8–T1)
Mechanism:
- Forceful hyperabduction of arm (grabbing overhead support during a fall, breech delivery with arms raised)
Roots injured: C8, T1
Muscles paralyzed: Intrinsic hand muscles (lumbricals, interossei, thenar, hypothenar)
Clinical finding: Claw hand — combined features of median + ulnar nerve palsy
Sensory loss: Medial forearm, hand, medial 1.5 fingers
Horner Syndrome (ptosis, miosis, enophthalmos, anhidrosis): Present when T1 root is involved — sympathetic fibers to face travel with T1
Prognosis: Poor; <2% of neonatal cases
S. Das Manual of Clinical Surgery, 13th Ed., p. 140
INJURY PATTERN 3 — TOTAL PLEXUS PALSY (C5–T1)
- Complete flaccid paralysis of the entire upper limb
- Anaesthesia of the whole upper limb (sparing upper arm skin via C3–4)
- Horner syndrome present (T1 involvement)
- Worst prognosis
- Occurs only in severe high-energy trauma
NERVE INJURY CLASSIFICATION TABLE (Emergency Quick Reference)
| Injury Type | Roots | Posture | Key Deficit | Horner? |
|---|---|---|---|---|
| Erb-Duchenne | C5–C6 | Waiter's tip | No shoulder abduction, no elbow flexion | No |
| Klumpke | C8–T1 | Claw hand | No intrinsic hand muscles | Yes (if T1) |
| Total plexus | C5–T1 | Flail arm | Complete paralysis + anaesthesia | Yes |
🏥 EMERGENCY MEDICINE CLINICAL SCENARIOS
1. Shoulder Dislocation (Infraclavicular Plexus Injury)
Anterior shoulder dislocation is the most common EM cause of brachial plexus injury in adults. The infraclavicular plexus (cords level) is at risk.
- Axillary nerve (C5–C6) most commonly injured: loss of deltoid function + patch of sensory loss over lateral arm ("regimental badge area")
- Test axillary nerve before and after reduction: sensation over lateral deltoid
- Musculocutaneous nerve may also be injured (loss of biceps)
- [Rockwood and Green's Fractures, 2025] documents this as the most common nerve injury with shoulder dislocation
EM Action: Always document distal neurovascular exam before and after reduction. Check deltoid sensation, grip, biceps function.
2. Clavicle Fractures (Supraclavicular Plexus)
- Displaced mid-shaft clavicle fractures can injure the supraclavicular plexus (trunks level)
- Usually neuropraxia/axonotmesis — most recover
- Check suprascapular nerve function (shoulder abduction + external rotation)
- Also risk of subclavian vessel injury — always palpate distal pulses
3. High-Energy Polytrauma (Root Avulsion)
- Common with motorcycle accidents (head forced away from shoulder during impact)
- Nerve roots can be avulsed from the spinal cord — these are preganglionic injuries (worst type, no spontaneous recovery)
- Associated with ipsilateral Horner syndrome, phrenic nerve palsy (C5 root), hemidiaphragm paralysis
- MRI cervical spine for pseudomeningoceles (indicative of root avulsion)
- [Grainger & Allison's Diagnostic Radiology] emphasizes avulsion occurs in polytrauma with traction force
4. Pancoast Tumor (Neoplastic Plexopathy)
- Apical lung tumor (superior sulcus) invades the lower trunk (C8–T1) from below
- Presents as:
- Progressive hand weakness and wasting
- Horner syndrome (sympathetic chain involvement)
- Severe shoulder and medial arm pain
- ± venous distension (SVC/subclavian vein compression)
- EM red flag: unilateral hand weakness + Horner + shoulder pain in a smoker = Pancoast until proven otherwise
- Confirmed with chest X-ray (apical mass) → CT chest
Harrison's Principles of Internal Medicine, 22nd Ed., 2025; S. Das Surgery, p. 140
5. Thoracic Outlet Syndrome (TOS)
- Compression of the brachial plexus (and/or subclavian vessels) between the clavicle and first rib
- Neurogenic TOS: lower trunk (C8–T1) most common → ulnar nerve-type pain, hand intrinsic wasting
- Vascular TOS: subclavian artery/vein compression → arm ischemia, Raynaud's
- EM presentation: effort thrombosis (Paget-Schroetter syndrome) — young athlete with arm swelling and pain
6. Parsonage-Turner Syndrome (Brachial Neuritis)
- Sudden severe shoulder/arm pain followed by rapid motor deficits
- Often post-viral, post-vaccination, or idiopathic
- Affects individual nerve components, especially suprascapular nerve (infraspinatus, supraspinatus)
- Mimics rotator cuff injury or cervical radiculopathy in the ED
- No sensory level; MRI of brachial plexus shows enhancement in acute phase
Neuroanatomy through Clinical Cases, 3rd Ed.
🔑 EMERGENCY EXAM QUICK GUIDE
| Nerve | Root | Test |
|---|---|---|
| Axillary | C5, C6 | Deltoid contraction + lateral arm sensation |
| Musculocutaneous | C5–C7 | Biceps contraction + lateral forearm sensation |
| Radial | C5–T1 | Wrist/finger extension; posterior forearm sensation |
| Median | C6–T1 | Thumb opposition ("OK sign"); thenar wasting; palmar sensation |
| Ulnar | C8, T1 | Finger abduction ("spread fingers"); hypothenar wasting; little finger sensation |
🔴 RED FLAGS IN THE ED
| Finding | Think |
|---|---|
| Flail arm + Horner after motorcycle crash | Root avulsion / total plexus injury |
| Waiter's tip after delivery/shoulder fall | Erb-Duchenne palsy (C5–C6) |
| Claw hand + Horner + medial arm pain | Klumpke's palsy / Pancoast tumor |
| Deltoid weakness after shoulder reduction | Axillary nerve injury |
| Sudden shoulder pain + weak arm, no trauma | Parsonage-Turner syndrome |
| Young athlete with arm swelling + subclavian vein | Effort thrombosis (TOS) |
| Winging of scapula after chest trauma | Long thoracic nerve injury |
📐 NERVE REGENERATION — EM PROGNOSTIC PEARLS
- Nerve regenerates at approximately 1 mm/day after axonotmesis
- Hofmann-Tinel sign (distal tingling on tapping) tracks regeneration front
- Surgical repair must ideally occur within 1–2 months to maximize functional recovery
- After brachial plexus injury: may take 12–18 months for axons to reinnervate distal targets
- Lack of biceps function at 6 months = poor prognosis marker in birth palsy
- Horner syndrome = T1 root involvement = poor prognosis
Rockwood and Green's Fractures in Adults, 10th Ed., 2025; Miller's Review of Orthopaedics, 9th Ed.
Sources:
- Gray's Anatomy for Students (4th Ed.), pp. 858–861
- S. Das — A Manual on Clinical Surgery (13th Ed.), p. 140
- Rockwood and Green's Fractures in Adults (10th Ed., 2025)
- Miller's Review of Orthopaedics (9th Ed.), p. 260
- Harrison's Principles of Internal Medicine (22nd Ed., 2025)
- Harriet Lane Handbook (23rd Ed.), p. 664
- Grainger & Allison's Diagnostic Radiology
- Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.