
IMG_2617.jpg
Analysis and told me
analyse_media
Reading File
Here is a full analysis of this hospital admission document:
Hospital Admission Sheet - Analysis
Patient & Ward Details
| Field | Value |
|---|---|
| Ward | Male Ward |
| Unit | U-2 |
| Bed/Cabin | B-14 |
| Contact | 01851707327 |
| Date Signed | 05.7.4 (likely 05/07/2024 or 05/07/2025) |
Clinical History (সংক্ষিপ্ত ইতিহাস)
- C/C (Chief Complaint): Not explicitly written, but implied from diagnosis
- Old Stroke - the patient has a known prior history of stroke
Working Diagnosis
D: CVD - this stands for Cerebrovascular Disease (given the context of "old stroke"), not cardiovascular disease. The patient is being admitted likely for a new or recurrent cerebrovascular event.
Treatment Orders (Rx)
| Order | Meaning |
|---|---|
| Diet - N | Normal diet |
| Inf N/S 1L IV @ 30 d/min | Intravenous Normal Saline (0.9% NaCl), 1 Liter, given at 30 drops per minute - for hydration/IV access |
| Inj PPI 40mg, 1 vial IV BD | Proton Pump Inhibitor (e.g., Pantoprazole/Omeprazole) 40mg IV, twice daily - gastroprotection, common in stroke patients on medications |
| Tab Tiginon 10mg, 0+0+1 | Timonium Methylsulfate (Tiginon) 10mg tablet, once at night only - an antispasmodic agent, often used for abdominal cramps/smooth muscle spasm |
Investigations Advised (Adv)
- CT Scan of Brain - to assess the brain for new or old infarct, hemorrhage, or other structural changes related to the stroke history
- ECG (Electrocardiogram) - to check for atrial fibrillation or other arrhythmias that are common causes/complications of stroke
Summary
This is a Bangladeshi government hospital admission sheet (note Bangladesh Security Printing Press details at bottom). The patient is a male admitted to Ward U-2, Bed B-14 with a background history of old stroke, now admitted under a diagnosis of Cerebrovascular Disease (CVD).
The management plan is conservative and supportive:
- IV fluids (Normal Saline) for hydration
- IV PPI for stomach protection
- An antispasmodic (Tiginon) at night, possibly for associated GI complaints
- CT brain and ECG ordered as urgent investigations to guide further management
The overall clinical picture is consistent with a post-stroke or recurrent stroke workup in a resource-limited hospital setting in Bangladesh.
What are the typical causes of stroke that appear on CT scans?
Finding Sources
Finding Sources
Searching the Web
stroke types CT scan findings ischemic hemorrhagic causes radiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have rich textbook content and real CT images. Here is a thorough answer:
Stroke: Causes and CT Scan Findings
The first and most important role of a CT scan in stroke is to separate ischemic stroke from hemorrhagic stroke, since CT findings alone can dictate whether a patient gets thrombolytics (which would be dangerous in hemorrhage). As Harrison's states: "there are no reliable clinical findings that conclusively separate ischemia from hemorrhage" - CT is what makes the distinction. - Harrison's Principles of Internal Medicine 22E, p. 3483
The Two Main Types and Their CT Appearances
1. Ischemic Stroke (~85% of all strokes)
Cause: Blockage of a blood-supplying artery to the brain, starving brain tissue of oxygen and glucose.
CT findings:
- Early (0-6 hrs): CT is often normal or shows subtle signs. The key early finding is a hypodense (dark) area in the territory of the affected artery, representing cytotoxic edema and cell death
- Hyperdense artery sign: A clot sitting in the middle cerebral artery (MCA) appears as a bright white dot/stripe - this is an early, specific sign of large vessel occlusion
- Loss of grey-white differentiation in the insular cortex or basal ganglia
- Established infarct (>24 hrs): A clearly demarcated, wedge-shaped hypodense (dark) region following a vascular territory
The three major underlying causes are:
| Cause | Mechanism | Key Risk Factors |
|---|---|---|
| Atherothrombosis (large artery) | Atherosclerotic plaque in carotid/cerebral artery causes stenosis or local clot | Hypertension, diabetes, smoking, high LDL |
| Cardioembolic | Clot from the heart travels to the brain | Atrial fibrillation (most common single cause), mechanical valves, infective endocarditis, myocardial infarction, cardiomyopathy, patent foramen ovale |
| Small vessel (lacunar) | Occlusion of tiny penetrating arteries deep in the brain | Chronic hypertension, diabetes |
Other less common ischemic causes include: arterial dissection, fibromuscular dysplasia, aortic arch atherosclerosis, sickle cell disease, vasculitis, hypercoagulable states, and elevated homocysteine. - Goldman-Cecil Medicine, Pathobiology section
2. Hemorrhagic Stroke (~15-20% of all strokes)
This is further divided into:
A. Intracerebral Hemorrhage (ICH) - ~10-15% of all strokes
CT appearance: A round or oval hyperdense (bright white) lesion within the brain parenchyma. This is the hallmark finding - blood absorbs X-rays strongly and appears very bright.
- Early: 40-60 Hounsfield Units (HU), may look heterogeneous
- Hours to days: 60-80 HU, becomes more homogenously hyperdense
- Later: 80-100 HU as the clot fully organizes
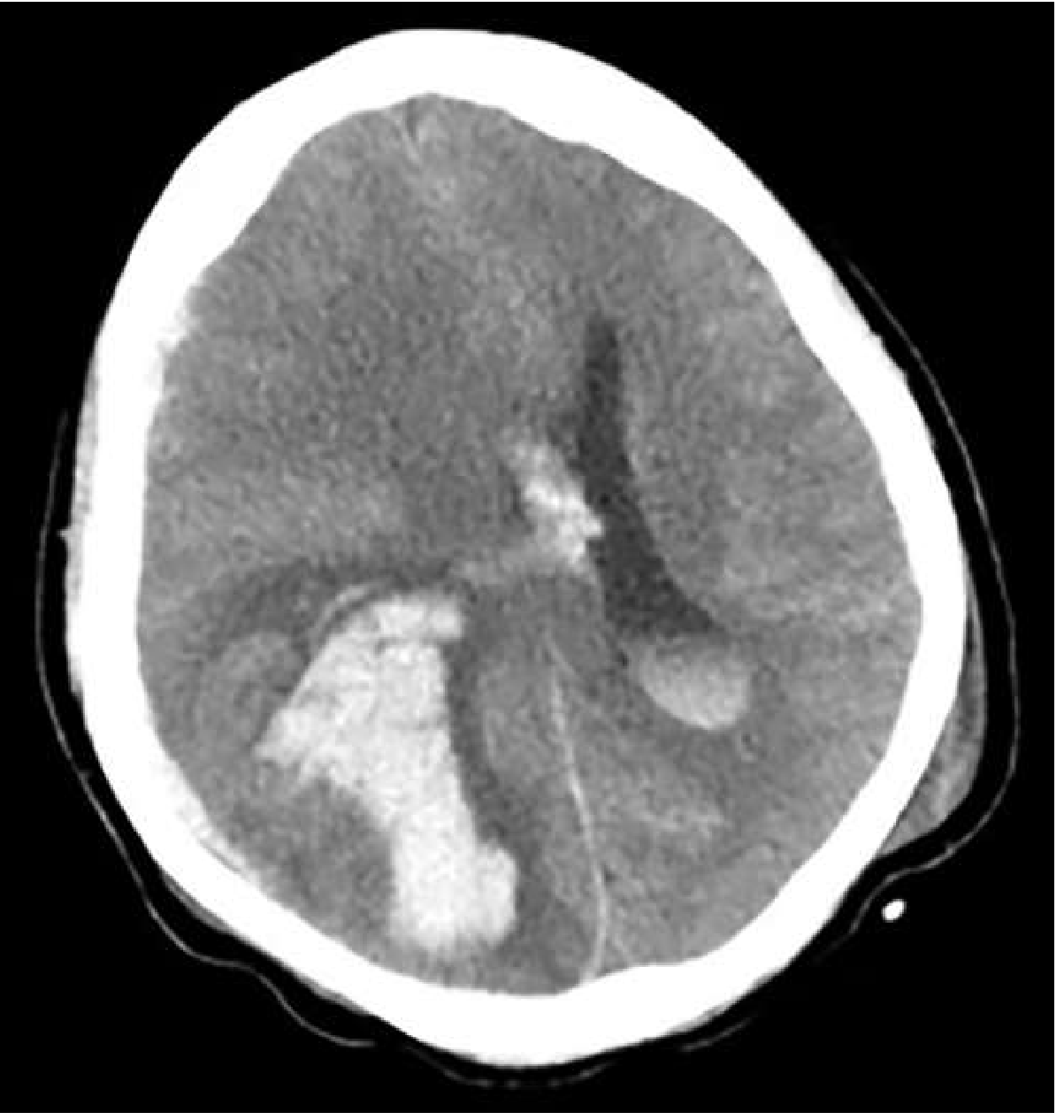
CT scan showing intracerebral hemorrhage - the large bright white area is fresh blood within brain tissue - Goldman-Cecil Medicine, Fig. 377-5
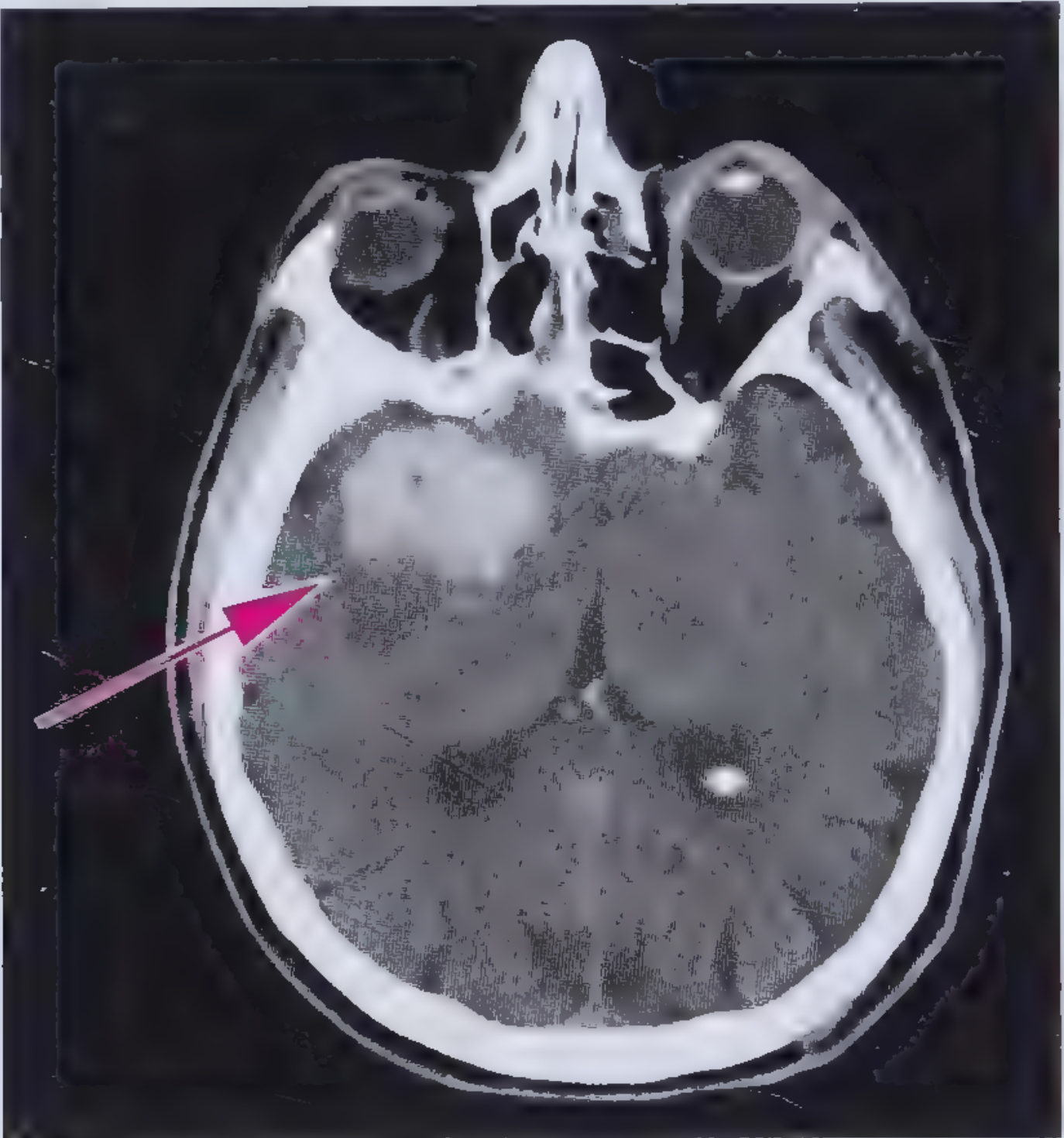
CT showing hyperdense bleed (arrow) in the right temporal lobe - Frameworks for Internal Medicine, Fig. 43-5
Causes of ICH:
- Hypertension - single most common cause; causes rupture of small deep penetrating vessels; typical locations: basal ganglia, thalamus, pons, cerebellum
- Cerebral amyloid angiopathy - common in elderly; causes lobar (cortical) hemorrhages
- Anticoagulation / coagulopathy (e.g., warfarin, heparin, thrombolytics)
- AVM (arteriovenous malformation)
- Brain tumors (primary or metastatic)
- Cocaine and sympathomimetic drug use
- Alcohol (risk factor)
B. Subarachnoid Hemorrhage (SAH) - ~5% of all strokes
CT appearance: Blood in the subarachnoid space (between brain and inner covering), classically appearing as bright white star/clover pattern filling the sulci and basal cisterns
Cause: Rupture of a cerebral aneurysm (berry aneurysm) in ~80% of cases. The sudden severe "thunderclap headache" - the worst headache of one's life - is the classic presentation.
Summary Table
| Stroke Type | CT Appearance | Main Causes |
|---|---|---|
| Ischemic (acute) | Normal or subtle hypodensity; hyperdense artery sign | Atherosclerosis, AF, small vessel disease |
| Ischemic (established) | Wedge-shaped dark (hypodense) area | Same as above |
| ICH | Bright white (hyperdense) round mass | Hypertension #1, amyloid angiopathy, anticoagulants |
| SAH | Bright white blood in subarachnoid spaces/cisterns | Aneurysm rupture #1 |
Why CT Matters in This Patient
For the patient in the admission sheet with "old stroke" and working diagnosis of CVD, the CT brain ordered will:
- Rule out new hemorrhage
- Identify if there is a new ischemic infarct
- Show the location and extent of the old stroke
- Guide whether anticoagulation (for cardioembolic causes like AF) or antiplatelets are appropriate
The ECG ordered alongside it is specifically looking for atrial fibrillation, which is the most common single cause of cardioembolic (ischemic) stroke.
This is a shared conversation. Sign in to Orris to start your own chat.