Heart failure
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"heart failure"[MeSH Terms] AND "guideline"[pt]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Heart Failure - Comprehensive Exam-Level Review
1. Definition
Heart failure (HF) is a clinical syndrome in which the heart cannot pump sufficient blood to meet the metabolic demands of the body, or can only do so at elevated filling pressures. It is a syndrome, not a single disease - cardiac output is typically below the normal ~5 L/min/70 kg, though "high-output" failure is a rare exception (see below).
- Braunwald's Heart Disease defines HF as a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood.
2. Classification
2a. By Ejection Fraction (EF)
| Type | EF | Key Feature |
|---|---|---|
| HFrEF (HF with reduced EF) | < 40% | Systolic dysfunction; impaired contraction |
| HFmrEF (mildly reduced EF) | 40-49% | Intermediate; often ischemic etiology |
| HFpEF (preserved EF) | ≥ 50% | Diastolic dysfunction; stiff ventricle |
HFpEF accounts for ~50% of all HF and does not respond well to positive inotropic drugs. Cardiac output may be reduced despite a normal EF due to impaired diastolic filling.
2b. ACC/AHA Stages vs. NYHA Functional Classification
(from Braunwald's Heart Disease, ACC/AHA table)
| ACC/AHA Stage | Description | NYHA Class |
|---|---|---|
| A | High risk, no structural disease, no symptoms | None |
| B | Structural heart disease, no symptoms | I |
| C | Structural disease + current or prior symptoms | I, II, III |
| D | Refractory HF requiring specialized intervention | IV |
NYHA Classes:
- I - No limitation; ordinary activity does not cause symptoms
- II - Slight limitation; ordinary activity causes dyspnea/fatigue
- III - Marked limitation; less-than-ordinary activity causes symptoms
- IV - Symptoms at rest; unable to carry on any activity without symptoms
Both systems are used together: ACC/AHA stages emphasize disease progression and prevention; NYHA class guides therapy eligibility (e.g., mineralocorticoid receptor antagonists require NYHA class II-IV; CRT requires class III-IV).
2c. High-Output Failure (rare)
Occurs when body demands exceed even a supranormal cardiac output. Causes: hyperthyroidism, beriberi (vitamin B1 deficiency), severe anemia, arteriovenous shunts. Treatment targets the underlying cause, not standard HF drugs. - Katzung's Basic and Clinical Pharmacology, 16th Edition
3. Pathophysiology
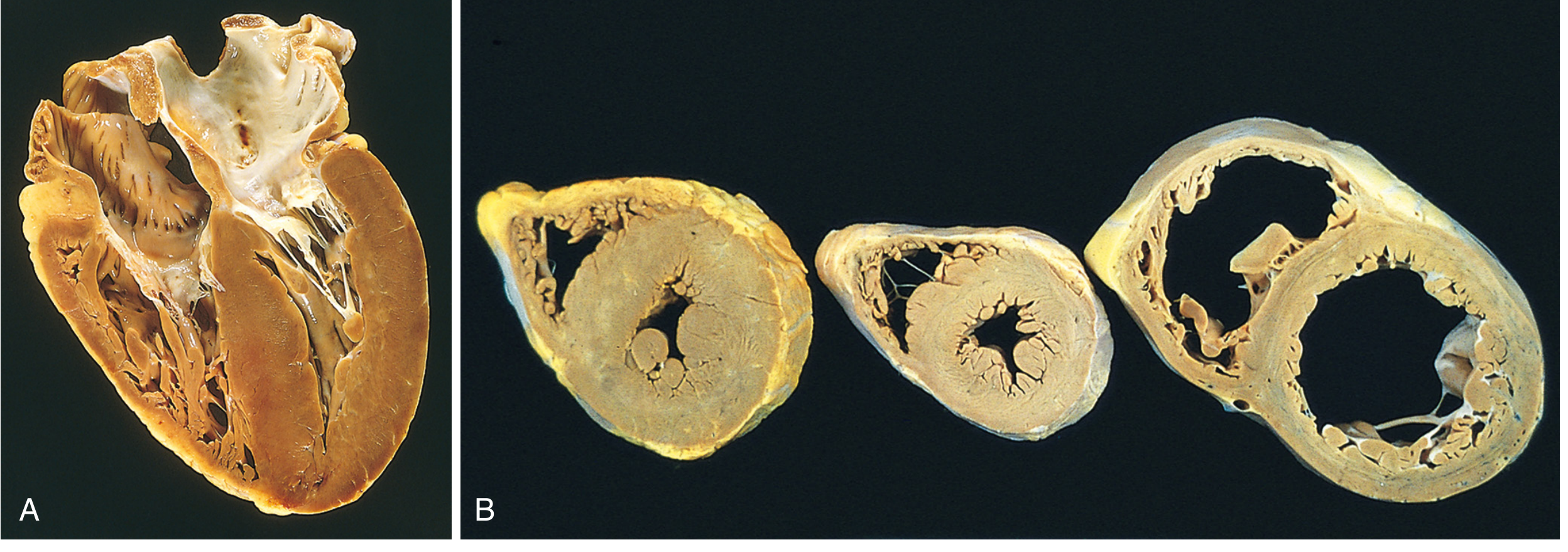
3a. Initiating Injury and Hypertrophy
Any sustained increase in mechanical work - pressure overload (e.g., hypertension, aortic stenosis) or volume overload (e.g., mitral/aortic regurgitation) - causes myocyte hypertrophy via increased protein synthesis and sarcomere assembly.
- Concentric hypertrophy (pressure overload): new sarcomeres assembled in parallel → increased wall thickness, normal/reduced cavity size
- Eccentric hypertrophy (volume overload): new sarcomeres assembled in series → ventricular dilation; wall thickness may be normal or reduced
Importantly, myocyte hypertrophy is NOT accompanied by a proportional increase in capillary density, creating a supply-demand mismatch, especially under pressure overload. - Robbins, Cotran & Kumar Pathologic Basis of Disease
3b. Cellular/Molecular Changes
With progressive failure, the following occur:
- Calcium handling abnormalities: Phosphorylation of RyR channels in SR enhances Ca²⁺ leak; SERCA activity is impaired (reduced Ca²⁺ reuptake) → reduced contractility + arrhythmias
- Beta-receptor downregulation: Prolonged sympathetic drive causes β1-receptor downregulation, reducing inotropic response; β3 receptors (not downregulated) may mediate negative inotropy
- Remodeling: Dilation beyond passive stretch, connective tissue proliferation, abnormal fetal-phenotype myocytes. Myocytes die by accelerated apoptosis (caspase activation by excessive β-stimulation), increasing stress on remaining cells
- Potassium channel changes: Facilitate arrhythmogenesis - a primary cause of death in HF
- Katzung's Basic and Clinical Pharmacology, 16th Edition
3c. Neurohumoral Compensation - The Vicious Cycle
This is the central mechanism driving HF progression:
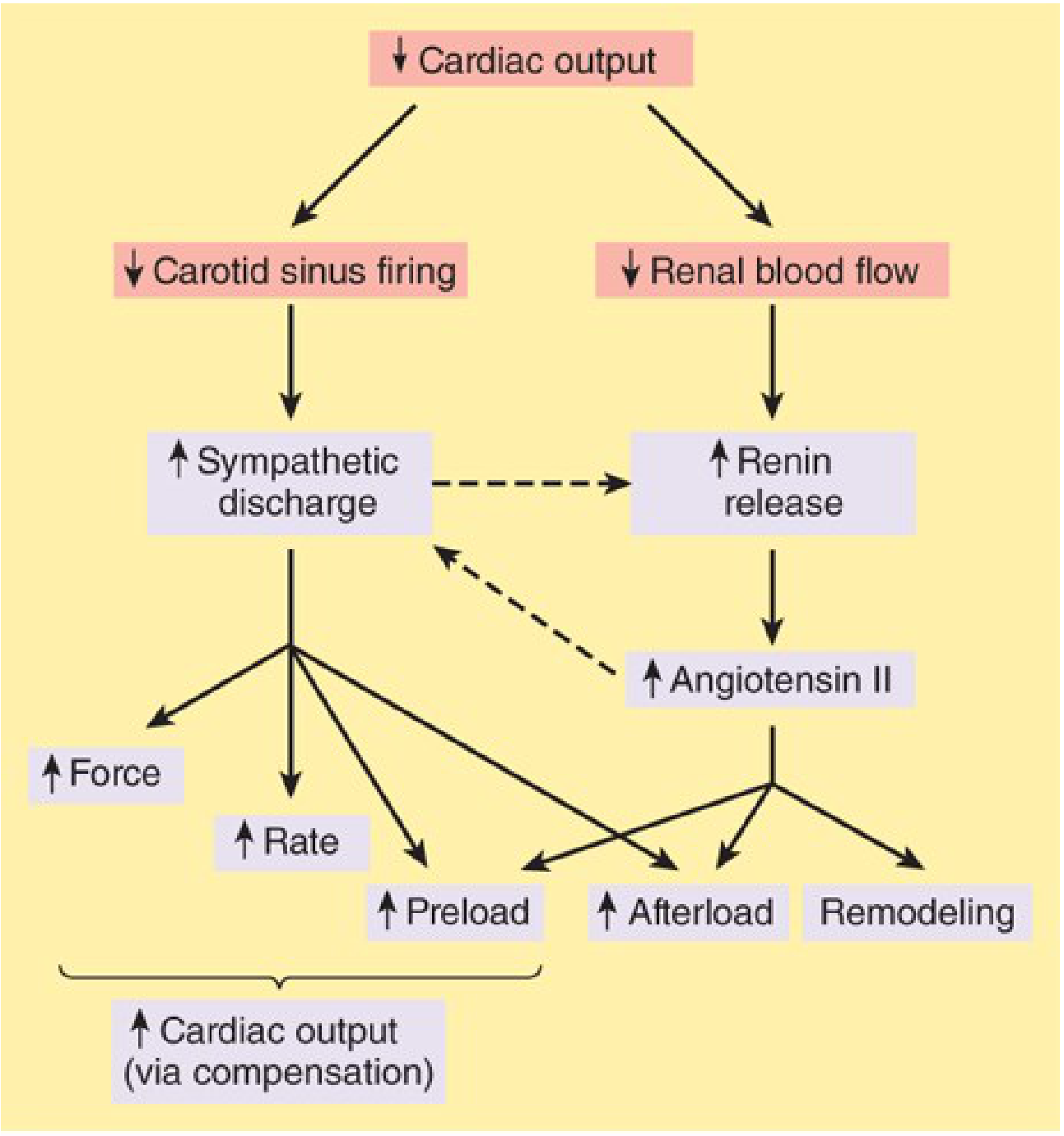
Key pathway:
- ↓ CO → ↓ carotid sinus firing → baroreceptor reflex reset → ↑ sympathetic outflow + ↓ parasympathetic outflow
- ↓ CO → ↓ renal blood flow → ↑ renin → ↑ angiotensin II → vasoconstriction + aldosterone secretion + NE release
- Angiotensin II causes: vasoconstriction (↑ afterload), myocyte + ECM hypertrophy (maladaptive remodeling), sodium/water retention (↑ preload), prothrombotic effects
- ↑ Afterload → ↓ EF → ↓ CO → cycle repeats (downward spiral)
- Endothelin, vasopressin, aldosterone further worsen congestion and remodeling
Counterregulatory hormones: Natriuretic peptides (BNP, NT-proBNP) released from overstretched ventricles attempt to promote natriuresis/vasodilation - and serve as important diagnostic biomarkers.
3d. Frank-Starling Mechanics
- In the normal heart, increasing preload (LVEDP <15 mmHg) increases stroke work (ascending limb of Starling curve)
- In HF, the curve is shifted downward and rightward - the same preload produces less stroke work
- At filling pressures >20-25 mmHg, pulmonary congestion occurs
- Increased preload in HF comes from increased blood volume and venous tone
3e. Four Determinants of Cardiac Performance
- Preload - ventricular filling pressure / end-diastolic fiber length
- Afterload - systemic vascular resistance opposing ejection
- Contractility (inotropy) - intrinsic myocardial contractile state (independent of load)
- Heart rate
In HF: contractility ↓ → compensatory ↑ preload (Starling) and ↑ HR and ↑ SVR (neurohumoral), but these compensations become maladaptive over time.
4. Etiology
Common causes:
- Ischemic heart disease (most common in developed world) - myocardial infarction, ischemic cardiomyopathy
- Hypertension - pressure overload → concentric LVH → diastolic HF or eventual systolic dysfunction
- Dilated cardiomyopathy - idiopathic, viral, alcoholic, peripartum, familial
- Valvular disease - aortic stenosis (pressure overload), mitral/aortic regurgitation (volume overload)
- Hypertrophic cardiomyopathy
- Other: diabetes, obesity, thyroid disease, amyloidosis, tachycardia-mediated, cardiotoxins (doxorubicin)
5. Clinical Features
Symptoms
| Left HF (pulmonary congestion) | Right HF (systemic venous congestion) |
|---|---|
| Dyspnea on exertion | Peripheral edema (dependent) |
| Orthopnea (dyspnea lying flat) | Ascites |
| Paroxysmal nocturnal dyspnea (PND) | Hepatomegaly / hepatojugular reflux |
| Fatigue, reduced exercise tolerance | Jugular venous distension (JVD) |
| Cough (cardiac asthma) | Anorexia, nausea (bowel edema) |
| Tachycardia |
Signs
- S3 gallop - best sign of elevated LVEDP; high specificity for systolic HF
- S4 gallop - stiff, non-compliant ventricle (diastolic dysfunction)
- Displaced apex (cardiomegaly)
- Bi-basal crackles (pulmonary edema)
- Pleural effusion (more common on right)
- Cheyne-Stokes respiration (in severe HF with low CO)
- Pulsus alternans (alternating strong/weak beats - severe LV dysfunction)
6. Diagnosis
Per Braunwald's Heart Disease, the goals of clinical assessment are to:
- Confirm HF is present
- Define the type (HFrEF vs HFpEF)
- Identify the underlying cause
- Assess severity
- Identify comorbidities
No single sign or symptom defines HF - a multi-modal approach is required.
Key Investigations
| Test | Finding/Use |
|---|---|
| Echocardiography | Gold standard - EF, wall motion, valve function, diastolic indices |
| BNP / NT-proBNP | ↑ in HF; useful for diagnosis and prognosis monitoring |
| Chest X-ray | Cardiomegaly, pulmonary vascular congestion, Kerley B lines, pleural effusion |
| ECG | LVH, prior MI (Q waves), arrhythmias, LBBB (indicates CRT candidacy) |
| Serum electrolytes + renal function | Baseline + monitoring (K⁺, Na⁺, creatinine) |
| CBC | Anemia as a precipitant/comorbidity |
| Thyroid function | Hypothyroidism or thyrotoxicosis as cause |
| Coronary angiography / stress testing | If ischemic etiology suspected |
| Cardiac MRI | Myocarditis, infiltrative disease, viability |
7. Management
7a. Non-Pharmacological
- Sodium restriction (<2 g/day in symptomatic HF)
- Fluid restriction in severe hyponatremia or refractory congestion
- Daily weight monitoring
- Smoking cessation, alcohol avoidance
- Cardiac rehabilitation (approved for HF)
- Vaccinations (influenza, pneumococcus)
- Patient and family education on symptoms and discharge instructions
7b. Pharmacological - Chronic HFrEF (EF <40%)
The "four pillars" of guideline-directed medical therapy (GDMT) reduce mortality:
1. ARNI (Angiotensin Receptor-Neprilysin Inhibitor)
- Sacubitril/valsartan (Entresto) - preferred over ACE inhibitor or ARB alone
- Mechanism: sacubitril inhibits neprilysin (↑ natriuretic peptides) + valsartan blocks AT1R
- Must wait 36 hours after stopping ACE inhibitor before starting (angioedema risk)
- Starting dose: 49/51 mg twice daily; target dose: 97/103 mg twice daily
- Do NOT combine ACE inhibitor + ARNI (high angioedema risk)
2. ACE Inhibitors / ARBs (if ARNI not tolerated)
- Mechanism: block renin-angiotensin-aldosterone cascade
- ↓ angiotensin II → vasodilation + ↓ remodeling + ↓ aldosterone + ↓ sympathetic activation
- ACE inhibitors also accumulate bradykinin → cough (10-15%) and rare angioedema
- ARBs block AT1R selectively - no bradykinin accumulation → no cough
- Benefits: reduce LV size, improve EF, reduce symptoms and hospitalizations, prolong survival
- Indicated for all patients with LVSD regardless of symptoms or etiology
- Contraindications: angioedema (ACE-I), symptomatic hypotension, bilateral renal artery stenosis, K⁺ >5.5 mmol/L
- Goldman-Cecil Medicine
3. Beta-Blockers
- Counteract the maladaptive chronic sympathetic activation that worsens remodeling
- Only carvedilol, metoprolol succinate (CR/XL), and bisoprolol have proven mortality benefit
- Start low, titrate up slowly; do not start during acute decompensation
- Add to ARNI (or ACE-I/ARB) as cornerstone of treatment
4. Mineralocorticoid Receptor Antagonists (MRAs)
- Spironolactone or eplerenone
- Block aldosterone → ↓ sodium retention, ↓ hypokalemia, ↓ myocardial fibrosis
- Spironolactone: RALES trial - reduces mortality in severe HF (NYHA class III-IV) added to ACE-I
- Eplerenone: EMPHASIS-HF - reduces mortality in mild HF (NYHA class II) added to ACE-I + β-blocker
- Recommended for NYHA class II-IV with EF ≤35%
- Contraindications: K⁺ >5.0 mmol/L, creatinine >2.5 mg/dL
- Goldman-Cecil Medicine
5. SGLT2 Inhibitors (recent addition to all 4 pillars)
- Empagliflozin (EMPEROR-Reduced) and dapagliflozin (DAPA-HF) reduce cardiovascular death and HF hospitalizations in HFrEF
- Now part of "4 pillars" alongside ARNI, β-blocker, and MRA per the 2024 ACC Expert Consensus on HFrEF treatment
- Mechanism in HF: osmotic diuresis, reduced cardiac preload/afterload, possible direct myocardial effects; benefits are independent of diabetic status
6. Diuretics (symptom relief, not mortality benefit)
- Loop diuretics (furosemide, bumetanide, torsemide) - mainstay of decongestion
- Reduce preload → relieve pulmonary and peripheral congestion
- Monitor electrolytes (K⁺, Mg²⁺), renal function, volume status
- Alone they are not sufficient - must be combined with disease-modifying therapy
- In resistant congestion: IV diuretics, combination diuretics, or ultrafiltration
7. Digoxin (adjunctive)
- Mechanism: inhibits Na⁺/K⁺-ATPase → ↑ intracellular Na⁺ → ↓ NCX activity → ↑ intracellular Ca²⁺ → positive inotropy
- Also has vagotonic effects → slows AV conduction (useful if AF coexists)
- Does NOT reduce mortality; reduces hospitalizations (DIG trial)
- Narrow therapeutic index; toxicity risk especially with hypokalemia
- Now used mainly for symptom control or rate control in concomitant AF
7c. Pharmacological - Acute Decompensated HF
| Drug | Role |
|---|---|
| IV loop diuretics | First-line decongestion |
| IV vasodilators (nitrates, nitroprusside) | ↓ preload/afterload if adequate BP |
| Dobutamine | Selective β1-agonist; ↑ CO, ↓ filling pressure; risk of arrhythmia/ischemia |
| Dopamine | Useful if BP support needed |
| Milrinone | PDE3 inhibitor; ↑ cAMP → ↑ contractility + vasodilation; IV only; risk of arrhythmias |
| Levosimendan | Ca²⁺ sensitizer; approved in some countries; not in USA |
Positive inotropes (dobutamine, milrinone) are used only for acute HF or severe exacerbation. They are NOT first-line for chronic HF.
7d. Device Therapy
| Device | Indication |
|---|---|
| ICD (implantable cardioverter-defibrillator) | EF ≤35%, NYHA class II-III, on GDMT ≥3 months, expected survival >1 year |
| CRT (cardiac resynchronization therapy) | EF ≤35%, LBBB, QRS ≥150 ms, NYHA class II-IV |
| CRT-D | Combines ICD and CRT |
| LVAD (left ventricular assist device) | Bridge to transplant or destination therapy in advanced HF |
7e. HFpEF (EF ≥50%) - Management
HFpEF management is more limited in terms of mortality-reducing drugs:
- SGLT2 inhibitors now show mortality/morbidity benefit in HFpEF (EMPEROR-Preserved, DELIVER trials)
- Treat underlying causes: control hypertension, rate control in AF, manage obesity/diabetes
- Diuretics for symptoms
- ARBs/MRAs: modest benefit
- No proven benefit for ACE inhibitors, β-blockers, or digoxin specifically in HFpEF
- ASE 2025 updated recommendations for evaluating diastolic function and diagnosing HFpEF by echocardiography (PMID 40617625)
8. Prognosis
- Annual mortality of ~10% for stable HF; 50% at 5 years overall
- NYHA class IV: 1-year mortality ~50%
- NT-proBNP and NYHA class are the strongest prognostic markers
- Sudden cardiac death (arrhythmic) accounts for ~50% of deaths in HFrEF - rationale for ICD
- ICD/CRT, ARNI, and SGLT2 inhibitors have substantially improved outcomes in the modern era
9. Key Exam Summary Points
| Point | Detail |
|---|---|
| Gold-standard imaging | Echocardiogram |
| Best biomarker | BNP / NT-proBNP |
| First-line for HFrEF | ARNI + β-blocker + MRA + SGLT2i (4 pillars) |
| ACE-I → ARNI washout | 36-hour gap required |
| β-blockers with mortality benefit | Only carvedilol, metoprolol succinate, bisoprolol |
| MRA contraindication | K⁺ >5.0 mmol/L or creatinine >2.5 mg/dL |
| Digoxin mechanism | Na⁺/K⁺-ATPase inhibition → ↑ Ca²⁺ → positive inotropy |
| Dobutamine use | Acute HF only (β1 agonist, ↑ arrhythmia/ischemia risk) |
| HFpEF drug with mortality benefit | SGLT2 inhibitors |
| CRT indication | EF ≤35% + LBBB + QRS ≥150 ms + NYHA II-IV |
Sources: Braunwald's Heart Disease, 2 Vol Set (A Textbook of Cardiovascular Medicine); Goldman-Cecil Medicine International Edition; Katzung's Basic and Clinical Pharmacology, 16th Edition; Robbins, Cotran & Kumar Pathologic Basis of Disease. Recent guidelines: 2024 ACC Expert Consensus on HFrEF (PMID 38466244); ASE 2025 HFpEF echocardiography recommendations (PMID 40617625).
This is a shared conversation. Sign in to Orris to start your own chat.