Tell me streptococci from sketchy
Reading File
Finding Sources
Searching the Web
Sketchy Micro streptococci mnemonic summary
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the full Sketchy-style breakdown of Streptococci:
🍓 Streptococci - Sketchy Micro Style
Overview: The Classification Ladder
Streptococci are gram-positive cocci in chains, catalase-negative. The two major classification systems used clinically are:
| System | Basis | Key Groups |
|---|---|---|
| Lancefield | Cell wall carbohydrate antigen | A, B, C, D, F, G... |
| Hemolysis | Type of RBC lysis on blood agar | α, β, γ |
1. Streptococcus pyogenes (Group A Strep = GAS)
Trigger words: Group A, pharyngitis, pyoderma, rheumatic fever, glomerulonephritis
Basics
- Gram-positive cocci in short to medium chains (4-10 cells)
- β-hemolytic (complete clear zone on blood agar)
- β-hemolysis caused by Streptolysin O (oxygen-labile) and Streptolysin S (oxygen-stable)
- Aerobically: only Streptolysin S is active → incubate anaerobically for best yield
- More than 100 M-protein serotypes
GAS Cell Wall Structure
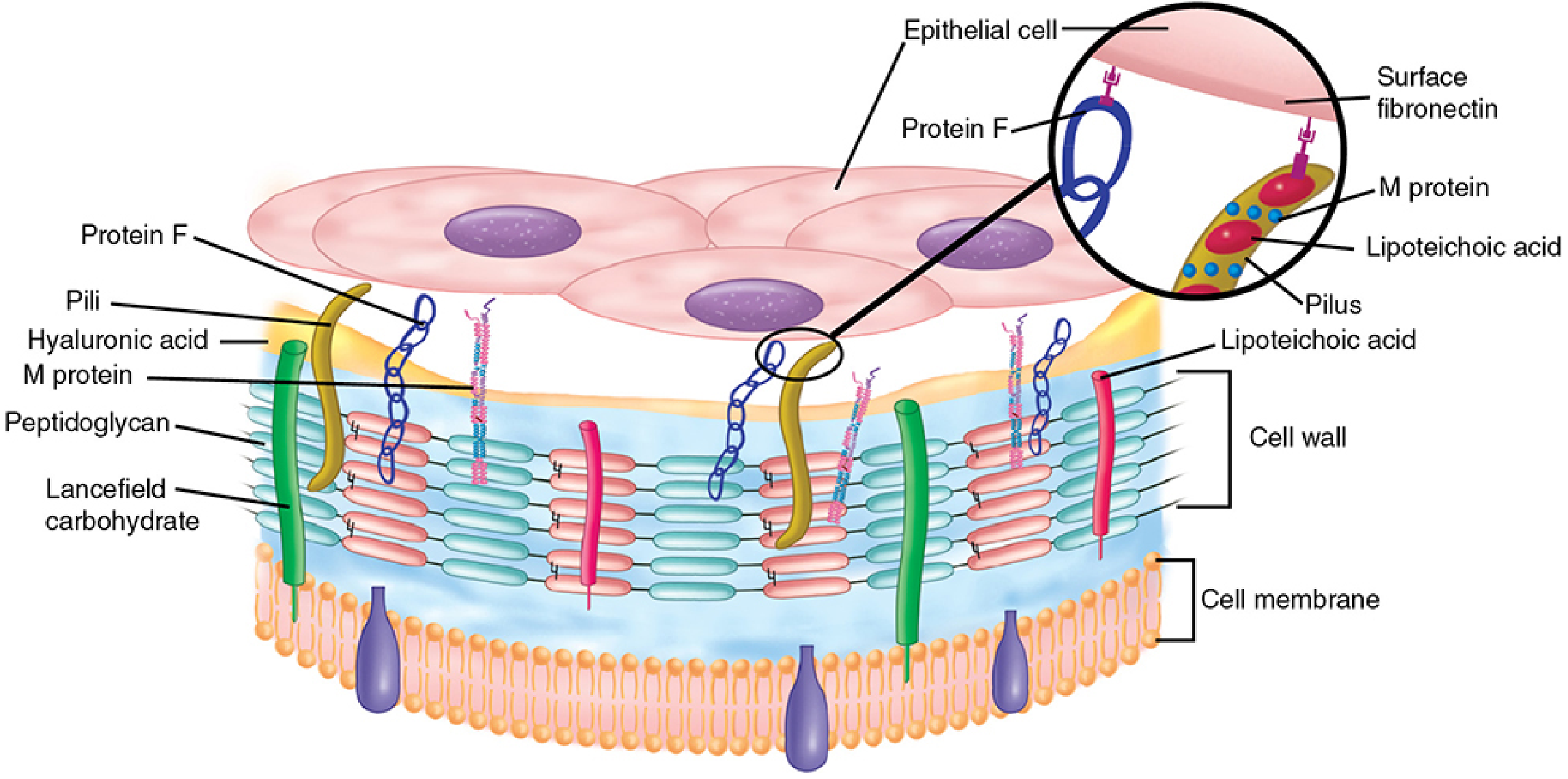
M protein and lipoteichoic acid (LTA) extend from cell wall surface. LTA + Protein F bind fibronectin on host epithelial cells. Lancefield group A carbohydrate sits inside the peptidoglycan matrix.
Virulence Factors (High-Yield Table)
| Factor | Function | Memory Hook |
|---|---|---|
| M protein | Antiphagocytic - binds Factor H → blocks C3b deposition; >100 serotypes; structural homology to myosin (key for ARF) | "M for Major virulence" |
| Hyaluronic acid capsule | Antiphagocytic, resembles host tissue → poor immunogen | |
| C5a peptidase | Inactivates C5a → blocks PMN chemotaxis | |
| Streptolysin O (SLO) | Oxygen-labile, pore-forming toxin; β-hemolysis; immunogenic → ASO antibodies | "O = Oxygen-labile, Oh so immunogenic" |
| Streptolysin S (SLS) | Oxygen-stable; causes surface hemolysis; NOT immunogenic | "S = Stable in air, Silent (non-immunogenic)" |
| Streptokinase | Lyses fibrin clots - promotes spread | |
| Hyaluronidase | "Spreading factor" - breaks down connective tissue | |
| DNase (streptodornase) | Degrades DNA in pus; anti-DNase B antibody used for skin infections | |
| Pyrogenic exotoxins (SPE A, B, C) | Superantigens → massive cytokine release → scarlet fever, STSS | "Pyrogenic = fire = rash/fever" |
| Protein F | Adhesin - binds fibronectin | |
| Lipoteichoic acid (LTA) | Adhesin - binds fibronectin |
Diseases
Suppurative (direct infection):
- Pharyngitis - #1 cause in children 5-15 yrs; sandpaper-like tonsils, exudate, tender anterior cervical nodes; no cough
- Impetigo / Pyoderma - golden-crusted skin lesions; children 2-5 yrs with poor hygiene; different M protein types than pharyngitis strains
- Scarlet fever - pharyngitis + SPE exotoxin → strawberry tongue + diffuse sandpaper rash (starts trunk, spares palms/soles) + circumoral pallor
- Erysipelas - bright red, raised, sharply demarcated skin infection (superficial dermis/lymphatics)
- Cellulitis - deeper soft tissue
- Necrotizing fasciitis - "flesh-eating bacteria"; rapidly spreading; surgical emergency
- Streptococcal Toxic Shock Syndrome (STSS) - SPE superantigens → massive cytokine storm → shock, renal failure, coagulopathy, rash; more invasive than staph TSS
Non-suppurative / Post-infectious (sequelae):
Acute Rheumatic Fever (ARF) - 2-4 weeks after pharyngitis only (not skin)
- Mechanism: Molecular mimicry - M protein homology to myosin → anti-streptococcal antibodies cross-react with cardiac tissue
- Jones Criteria (major): JONES = Joint (migratory polyarthritis), cOreA (Sydenham chorea), Nodules (subcutaneous), Erythema marginatum, heart (carditis)
- Prevention: treat pharyngitis with penicillin within 9 days
Post-streptococcal Glomerulonephritis (PSGN) - 1-4 weeks after pharyngitis OR 3-6 weeks after skin infection
- Immune complex deposition → diffuse proliferative glomerulonephritis
- Clinical: edema, hypertension, hematuria (cola-colored urine), proteinuria, ↓ serum complement (C3)
- Usually self-limited; does NOT prevent PSGN by treating the infection
Diagnosis
- Throat culture on sheep blood agar (anaerobically for best yield)
- Rapid strep test (antigen detection) - quick but less sensitive
- Identification: Bacitracin-sensitive (GAS unique among streptococci), PYR-positive, Lancefield group A antigen
- Serology: ASO titer - confirms prior pharyngitis; Anti-DNase B - for pharyngitis OR skin infection (more sensitive for PSGN)
Treatment
- Penicillin V or amoxicillin (pharyngitis) - no resistance ever documented
- Penicillin + clindamycin (systemic/invasive disease) - clindamycin blocks toxin production
- Penicillin-allergic: oral cephalosporin or macrolide
- No vaccine
2. Streptococcus agalactiae (Group B Strep = GBS)
Trigger words: Group B, neonatal disease, screening pregnant women
Basics
- β-hemolytic, gram-positive cocci in chains
- Group-specific B carbohydrate antigen + type-specific capsular polysaccharides (types Ia, Ib, II-VIII)
- Primary virulence = antiphagocytic polysaccharide capsule
- CAMP test positive (enhances hemolysis of Staph aureus sphingomyelinase)
- Bacitracin-resistant (unlike Group A)
Who Gets It?
| Population | Disease |
|---|---|
| Neonates (early-onset, 0-7 days) | Acquired during birth; sepsis, pneumonia, meningitis; premature rupture of membranes is a risk factor |
| Neonates (late-onset, 1 week - 3 months) | Meningitis, bacteremia |
| Pregnant women | Endometritis, UTI, wound infections, postpartum bacteremia |
| Immunocompromised adults | Bacteremia, pneumonia, bone/joint infections (diabetics, cancer, alcoholism) |
Prevention
- Screen all pregnant women at 35-37 weeks with vaginal/rectal swab culture
- Give IV penicillin G intrapartum (≥4 hours before delivery) if GBS positive
- No vaccine currently available
Treatment
- Penicillin G (drug of choice) ± aminoglycoside for serious infections
- Cephalosporin or vancomycin for penicillin-allergic patients
3. Streptococcus pneumoniae (Pneumococcus)
Trigger words: Diplococci, capsule, pneumonia, meningitis, vaccine, optochin, bile-soluble
Basics
- α-hemolytic (partial/green hemolysis)
- Lancet-shaped gram-positive diplococci (pairs)
- No Lancefield group antigen
- Distinctive polysaccharide capsule (>90 serotypes) = major virulence factor
- Cell wall has C-polysaccharide (teichoic acid with phosphorylcholine) - binds CRP; activates autolytic enzyme amidase
Virulence Factors
| Factor | Role |
|---|---|
| Polysaccharide capsule | Antiphagocytic - most important virulence factor |
| Pneumolysin | Pore-forming toxin; damages respiratory epithelium; activates complement |
| IgA protease | Cleaves secretory IgA in nasopharynx → colonization |
| Surface protein adhesins | Attachment to oropharynx |
| Teichoic acid / peptidoglycan fragments | Stimulate local inflammation |
Epidemiology
- Nasopharynx colonizer → endogenous spread to lungs, sinuses, ears, blood, meninges
- Highest colonization in young children and their contacts
- Disease more common in cool months
- At-risk: antecedent viral URI (influenza), asplenia (sickle cell → overwhelming sepsis), elderly, immunosuppressed, alcoholics
Diseases (mnemonic: MOPS)
- Meningitis (most common bacterial in adults; #1 overall with H. flu and N. meningitidis)
- Otitis media (most common bacterial cause in children)
- Pneumonia (most common bacterial CAP in adults; lobar pneumonia, rust-colored sputum)
- Sinusitis
Diagnosis
- Gram stain: gram-positive lancet-shaped diplococci
- Culture on sheep blood agar; α-hemolysis
- Identification: Optochin-sensitive (distinguishes from viridans strep), bile-soluble (bile salts lyse the organism by activating autolytic amidase)
- Quellung reaction (capsular swelling with type-specific antibody)
- Urine antigen test (C-polysaccharide) - sensitive for meningitis CSF, less sensitive for urine
- PCR - test of choice when antibiotics already given
Treatment
- Penicillin (susceptible strains)
- Vancomycin + ceftriaxone (empirical meningitis / until sensitivities known)
- Resistance: PBP2a-mediated (especially in meningitis dosing)
Vaccines
| Vaccine | Target | Who |
|---|---|---|
| PCV13 (Prevnar 13) | 13-valent conjugated | All children <2 years; immunocompromised adults |
| PPSV23 (Pneumovax 23) | 23-valent polysaccharide | Adults ≥65, high-risk groups (asplenia, sickle cell, DM) |
| PCV15/PCV20 | Newer conjugates | Adults ≥65 (current preference over PPSV23) |
4. Viridans Streptococci
Trigger words: Oral flora, endocarditis, dental procedure, α-hemolytic
Basics
- α-hemolytic (green partial hemolysis)
- No Lancefield antigens, no capsule
- Optochin-resistant (key to distinguish from Pneumococcus), bile-insoluble
- Normal residents of oral cavity (and GI, GU tract)
- Species: S. sanguis, S. salivarius, S. mitis, S. mutans, S. intermedius
High-Yield Associations
| Species | Disease |
|---|---|
| S. sanguis, S. mitis | Subacute bacterial endocarditis (SBE) on damaged valves after dental procedures |
| S. mutans | Dental caries (produces glucan/dextran from sucrose → plaque) |
| S. bovis (now S. gallolyticus) | Endocarditis + colon cancer - always colonoscope if isolated! |
| S. anginosus group (S. constellatus, S. intermedius) | Abscesses (brain, liver, lung); variable hemolysis; associated with A, B, C, G Lancefield antigens |
| Granulicatella / Abiotrophia (nutritionally variant strep, NVS) | Need pyridoxal (B6) to grow; striking association with endocarditis |
Endocarditis
- Dental procedures → bacteremia → viridans strep adhere to damaged/abnormal valves (prior rheumatic fever, MVP, prosthetic valves)
- Antibiotic prophylaxis (amoxicillin 1 hour before dental procedure) in high-risk cardiac conditions
5. Enterococcus (Group D - formerly Streptococci)
Trigger words: GI flora, UTI, resistant, peritonitis, nosocomial
Basics
- Gram-positive cocci in pairs and short chains (morphologically similar to pneumococcus)
- Group D glycerol teichoic acid cell wall antigen
- Variable hemolysis (α, β, or γ)
- Naturally resistant to cephalosporins (important!)
- Can form biofilms
- Two clinically important species: E. faecalis (more common, less resistant) and E. faecium (more resistant)
Epidemiology
- Colonizes the GI tract of humans and animals
- Spreads when broad-spectrum antibiotics (especially cephalosporins) disrupt normal flora
- Nosocomial; survives on environmental surfaces for prolonged periods
Diseases
- UTI (catheter-associated, most common)
- Peritonitis (polymicrobial)
- Endocarditis (especially in elderly, GI/GU instrumentation)
- Bacteremia, wound infections
Treatment
- Ampicillin (E. faecalis) ± gentamicin (synergy for endocarditis)
- Vancomycin for penicillin-resistant strains
- Linezolid or daptomycin for VRE (vancomycin-resistant enterococcus)
Quick Differentiation Table
| Feature | S. pyogenes (A) | S. agalactiae (B) | S. pneumoniae | Viridans | Enterococcus |
|---|---|---|---|---|---|
| Hemolysis | β | β | α | α | Variable |
| Lancefield | A | B | None | None | D |
| Bacitracin | Sensitive ✓ | Resistant | Resistant | Resistant | Resistant |
| Optochin | Resistant | Resistant | Sensitive ✓ | Resistant | Resistant |
| Bile solubility | Insoluble | Insoluble | Soluble ✓ | Insoluble | Insoluble |
| PYR test | Positive ✓ | Negative | Negative | Negative | Positive ✓ |
| CAMP test | Negative | Positive ✓ | Negative | Negative | Negative |
| Capsule | Hyaluronic acid | Polysaccharide | Polysaccharide | None | None |
Sketchy Mnemonics to Remember
- GAS (Group A) = "SHoP": Scarlet fever, Heart (rheumatic fever), glomerulonePHritis
- ASO titer = Confirms pharyngitis; Anti-DNase B = Confirms pharyngitis OR pyoderma
- GBS (Group B) = "Baby's Bug" - think neonatal meningitis/sepsis; screen mom at 35-37 weeks
- Pneumococcus = "MOPS" + optochin + bile soluble + diplococci
- S. bovis endocarditis = always rule out colon cancer
- Viridans = optochin-resistant α-hemolytics = oral flora endocarditis; S. mutans = dental caries
- Enterococcus = intrinsically cephalosporin-resistant; VRE treated with linezolid/daptomycin
Sources: Sherris & Ryan's Medical Microbiology 8e; Murray's Medical Microbiology 9e - comprehensive cross-referenced coverage of all streptococcal species.
This is a shared conversation. Sign in to Orris to start your own chat.