Position of rules tube
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
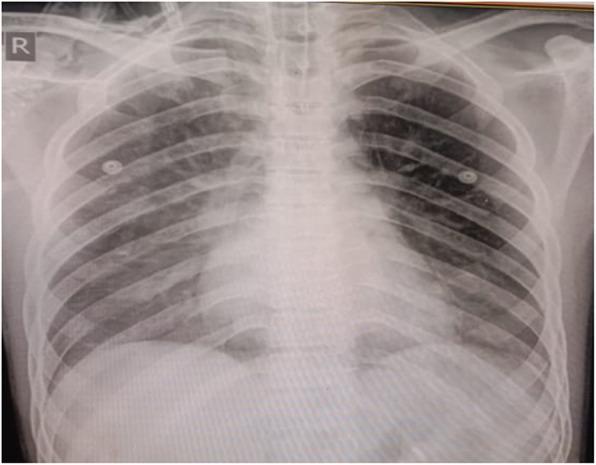
Ryle's nasogastric tube position stomach X-ray
Loading Image
Position of Ryle's Tube (Nasogastric Tube)
Ryle's tube is a radio-opaque, plastic nasogastric (NG) tube approximately 125 cm long with holes near the tip, used for gastric decompression, feeding, aspiration, and investigations.
Correct Position
The tip of a correctly placed Ryle's tube should lie in the most dependent part of the stomach — radiologically seen along the left border of the spinal column (i.e., within the gastric body/antrum, well below the diaphragm).
On a chest X-ray, correct placement is confirmed when:
- The tube follows a midline course down through the oesophagus
- It crosses the diaphragm (passes below it)
- The distal tip is seen well past the bronchial bifurcation (carina) and within the stomach bubble
How to Insert & Confirm Position
- Patient positioned semirecumbent
- Measure distance: tip of nose → xiphisternum (external estimate of required length)
- Lubricate tube, insert through a nostril, advance to 10 cm mark
- Ask patient to swallow repeatedly while advancing the tube
Confirming Correct Position (before feeding)
| Method | Criterion for Safety |
|---|---|
| Gastric aspirate pH | pH < 5 is considered safe |
| Chest X-ray | Tip below diaphragm, well past carina |
| Fluoroscopy | Tip in most dependent part of stomach, along left border of spine |
⚠️ Traditional auscultation ("whoosh test") is not a reliable method and should not be used alone.
Misplacement Complications
The most dangerous complication is tracheo-bronchial misplacement — the tube deviates into the trachea and down a mainstem bronchus (usually right). This must be excluded before feeding. Other errors include coiling in the oesophagus or hiatal hernia.
For Gastric Function Tests (S. Das)
When used for gastric secretion studies, the tube is positioned under fluoroscopy with the tip in the most dependent part of the stomach (along the left border of the spinal column), then connected to low continuous suction at 3–5 cm Hg subatmospheric pressure.
- S Das: A Manual on Clinical Surgery, 13th Ed., p. 498
- Bailey and Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.