Anemia during pregnancy
Reading File
Finding Sources
Searching PubMed
"anemia" AND "pregnancy" AND "management"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Anemia During Pregnancy
Anemia is the most common medical complication of pregnancy. It affects maternal and fetal outcomes across a spectrum from mild physiologic dilution to severe pathologic deficiency. The WHO defines anemia in pregnancy as hemoglobin (Hb) < 11 g/dL; severe anemia is Hb < 7 g/dL in the gravid patient, or < 8 g/dL postpartum.
1. Physiologic Basis - Why Anemia is Expected in Pregnancy
During pregnancy, blood volume increases by 40-45% (maximum at 34 weeks). Plasma volume rises by ~47%, but red blood cell (RBC) mass rises only ~17%. This disproportionate expansion causes a relative hemodilution - the hemoglobin nadir occurs between weeks 26-34.
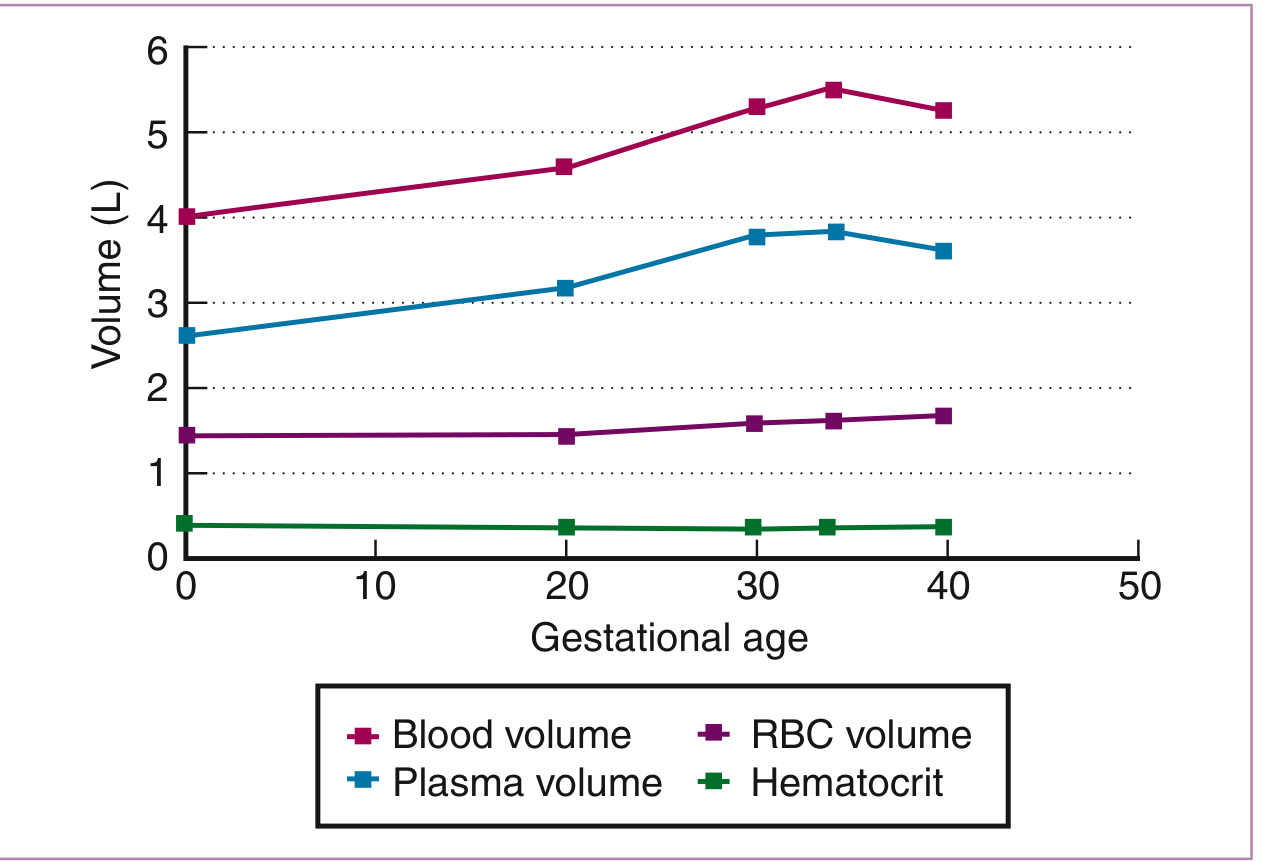
Hematologic changes during pregnancy. Plasma volume rises much faster than RBC volume, producing hemodilution. (Creasy & Resnik's Maternal-Fetal Medicine)
Key point: MCV and MCHC do not change with dilutional anemia. Progressive decreases in these indices suggest pathologic iron deficiency anemia (IDA).
Note: Women with Hb of 13-15 g/dL may actually have inadequate plasma volume expansion, which itself is associated with low birthweight and preterm birth.
2. Types of Anemia in Pregnancy
Four types predominate:
| Type | Prevalence | Key Feature |
|---|---|---|
| Dilutional (physiologic) | Universal | Normal MCV/MCHC |
| Iron deficiency anemia | 75% of all anemias in pregnancy; up to 47% prevalence | Microcytic, hypochromic |
| Folate deficiency | 2nd most common; low in high-income countries | Megaloblastic (macrocytic) |
| Sickle cell / hemoglobinopathies | Significant maternal/fetal morbidity | Variable morphology |
3. Iron Deficiency Anemia (IDA)
The dominant cause of anemia in pregnancy.
Pathophysiology
- Iron requirements increase substantially during pregnancy (fetal/placental needs + expanded maternal RBC mass)
- Women enter pregnancy with marginal iron stores: ~50% of primigravidas have minimal marrow iron in the first trimester
- Incidence of iron deficiency rises from 18% in T1 to 29% in T3 (NHANES data)
- Only 6% of iron-deficient women are also anemic - Hb alone is insufficient screening
Clinical Features
- Symptoms: fatigue, lethargy, headache, pica (craving clay, ice, starch)
- Signs: pallor, glossitis, cheilitis, koilonychia (rare)
- Lab: microcytic (low MCV), hypochromic (low MCHC), low serum iron, high TIBC, low serum ferritin (most sensitive test - cutoff of 30 ng/mL gives 92% sensitivity, 98% specificity)
Risks of Severe IDA (Hb < 6-7 g/dL)
- Increased fetal mortality
- Preterm birth and low birthweight
- Premature rupture of membranes
- Gestational hypertension
- Reduced amniotic fluid volume
- Neonatal anemia (2024 meta-analysis PMID 39425056 confirms association between maternal and neonatal anemia)
Treatment of IDA
Oral Iron (first-line, mild-moderate IDA):
- Ferrous sulfate 325 mg 1-3x/day (most common in US)
- WHO recommends 60 mg elemental iron/day + folic acid
- Single daily dosing is as effective as multiple doses and reduces GI side effects (nausea, constipation, GERD)
- Intermittent dosing (2-3x/week) has equivalent efficacy with fewer side effects
- Reticulocytosis expected at 7-10 days; Hb can rise ~1 g/week in severe cases
- Absorption enhanced by 500 mg ascorbic acid co-administration
- Continue for 6 months after Hb normalizes to replete stores
- Consider vitamin B6 supplementation in non-responders
Intravenous Iron (preferred in specific situations):
- Not used in the first trimester
- Treatment of choice for all IDA in the third trimester
- Severe IDA (Hb < 9 g/dL) in the second trimester
- Indications also include malabsorption, oral iron intolerance, need for rapid repletion
Six IV iron formulations approved in the US: iron sucrose (most commonly used), ferric carboxymaltose, ferumoxytol, ferric gluconate, iron isomaltoside, low-molecular-weight iron dextran
- Test dose only required for low-molecular-weight iron dextran
- Dose formula: Weight (kg) x (Target Hb - Actual Hb) x 0.24 + 500 mg; target Hb = 11-12 g/dL
Prophylaxis:
- ACOG, WHO, and major health authorities recommend ≥30 mg ferrous iron daily during all pregnancies
4. Folate Deficiency Anemia
- Folate requirements increase 5-10 fold in pregnancy (for rapid cell division)
- Megaloblastic (macrocytic) anemia - the second most common type
- Higher risk with: multiple gestations, short interpregnancy interval, malnutrition, hyperemesis gravidarum, malabsorption, antiepileptic drug use, alcoholism, poor diet
- Key consequence: Low folate is strongly linked to neural tube defects; also associated with placental abruption, preeclampsia, preterm birth, spontaneous abortion
Diagnosis: Serum folate (rapid response - normalizes within days of a folate-rich meal) + RBC folate (better for chronic status)
Treatment / Prevention:
- 0.4 mg/day - routine supplementation for all pregnant women
- 1.0 mg/day - known pregnancy-related folate deficiency
- 4.0 mg/day - prior neural tube defect pregnancy (starting 1 month before conception through 12 weeks GA)
- Continue throughout 2nd and 3rd trimesters per ACOG
5. Sickle Cell Disease (SCD) and Hemoglobinopathies
Sickle Cell Disease
- Pregnant women with SCD have a 6-fold increased risk of maternal death vs. controls
- Maternal complications: more frequent painful crises, preterm labor, PROM, infections, VTE (1.7-10x higher), preeclampsia, increased cesarean rate
- Fetal complications: placental infarction/insufficiency, low birthweight, small-for-gestational-age, preterm birth
Management:
- Vasoocclusive crises: treat as in nonpregnant patients
- Hydroxyurea is CONTRAINDICATED (known teratogenicity)
- NSAIDs avoided after 30 weeks gestation
- Regional anesthesia preferred for cesarean (general anesthesia increases post-op sickling)
- Iron supplementation and transfusion are controversial - risk of iron overload
- VTE prophylaxis should be considered
Thalassemias
- Alpha-thalassemia: MCV disproportionately low relative to Hb degree; normal RBC count; normal/mildly elevated RDW - key distinction from IDA (which shows proportional MCV-Hb drop, low RBC count, elevated RDW)
- Hb Bart's hydrops fetalis (all 4 alpha genes deleted) = incompatible with extrauterine life
- Beta-thalassemia: Diagnosed via Hb HPLC (elevated HbA2 > 3.5%); partner testing and genetic counseling essential
6. Laboratory Evaluation
Key labs with pregnancy-adjusted reference ranges (Creasy & Resnik):
| Test | Reference Range |
|---|---|
| Hb (anemia cutoff) | < 11 g/dL |
| MCV | 81-99 µm³ (trimester-dependent) |
| Serum ferritin | > 20 µg/L (best single test for iron deficiency) |
| Transferrin saturation | 16-60% |
| Serum folate | 8-240 µg/L (trimester-dependent) |
| Serum B12 | 99-656 pg/mL (trimester-dependent) |
| Hb electrophoresis | > 98% HbA, < 3.5% HbA2 |
| Direct Coombs | Negative |
7. Fetal Impact
A 2024 systematic review and meta-analysis (PMID 39425056) confirmed a significant association between maternal anemia and neonatal anemia, reinforcing the importance of diagnosing and treating maternal iron deficiency before delivery to optimize neonatal iron stores.
Summary
- Dilutional anemia is normal in pregnancy - treat only when iron deficient or symptomatic
- IDA accounts for ~75% of all pregnancy anemias; ferritin < 30 ng/mL is the most sensitive diagnostic marker
- Oral iron is first-line; IV iron preferred in T3 or severe anemia in T2
- Folate 0.4-4 mg/day (dose-dependent on risk) prevents megaloblastic anemia and neural tube defects
- SCD requires vigilant maternal monitoring; hydroxyurea is contraindicated
- Screen all women for thalassemia if CBC shows thalassemic indices (low MCV, normal/high RBC count, normal RDW)
Sources: Creasy & Resnik's Maternal-Fetal Medicine, Ch. 55; Rosen's Emergency Medicine; Goldman-Cecil Medicine
Make a 15 marks answer for examination point of view
Anemia in Pregnancy — 15 Marks Examination Answer
Definition
Anemia in pregnancy is defined as hemoglobin (Hb) < 11 g/dL at any point during pregnancy (WHO). Severe anemia is Hb < 7 g/dL.
Physiological Basis (Why Anemia Occurs)
During pregnancy, blood volume increases by 40-45% (maximum at 34 weeks):
- Plasma volume increases by 47%
- RBC mass increases by only 17%
This disproportionate hemodilution lowers Hb, hematocrit, and RBC count — but MCV and MCHC remain unchanged. This is the basis of physiological/dilutional anemia, which is normal and requires no treatment.
The Hb nadir occurs between 26-34 weeks of gestation.
Classification / Types
| Type | Frequency | Morphology |
|---|---|---|
| Iron Deficiency Anemia (IDA) | 75% of all anemias | Microcytic, hypochromic |
| Folate Deficiency | 2nd most common | Macrocytic (megaloblastic) |
| Vitamin B12 Deficiency | Uncommon | Macrocytic |
| Hemoglobinopathies (SCD, Thalassemia) | Significant | Variable |
| Aplastic/Hemolytic Anemia | Rare | Normocytic |
1. Iron Deficiency Anemia (IDA)
Etiology
- Increased iron demand: fetal growth, placenta, expanded maternal RBC mass
- Poor prepregnancy iron stores (50% of primigravidas have minimal marrow iron)
- Inadequate dietary intake
Clinical Features
- Symptoms: Fatigue, lethargy, headache, pica (craving clay, ice, starch - classic)
- Signs: Pallor, glossitis, cheilitis, koilonychia (rare), angular stomatitis
Diagnosis
- Microcytic, hypochromic picture on peripheral smear
- Low MCV, low MCHC, low serum iron, high TIBC
- Serum ferritin - most sensitive test (cutoff < 30 ng/mL: sensitivity 92%, specificity 98%)
- Low transferrin saturation (< 16%)
- Bone marrow: absent stainable iron (gold standard, rarely done)
Maternal and Fetal Complications
- Preterm birth, low birthweight
- Premature rupture of membranes (PROM)
- Gestational hypertension
- Reduced amniotic fluid
- Increased maternal mortality
- Neonatal anemia (directly correlated to maternal iron status)
Treatment
Oral Iron (mild-moderate IDA, Hb 9-11 g/dL):
- Ferrous sulfate 325 mg once to three times daily
- Single daily dose as effective as multiple doses; reduces GI side effects
- Reticulocytosis expected at 7-10 days; Hb rises ~1 g/week
- Add 500 mg ascorbic acid to enhance absorption
- Continue 6 months after normalization to replete stores
- Intermittent dosing (2-3x/week) acceptable - fewer side effects
Intravenous Iron (preferred in):
- Third trimester (all IDA)
- Severe IDA (Hb < 9 g/dL) in the second trimester
- Oral iron intolerance / malabsorption
- Not used in first trimester
- Agents: Iron sucrose (most common), ferric carboxymaltose, ferric gluconate
- Dose formula: Weight × (Target Hb - Actual Hb) × 0.24 + 500 mg; target Hb = 11-12 g/dL
Prophylaxis:
- ACOG and WHO: ≥ 30-60 mg elemental iron daily throughout pregnancy
2. Folate Deficiency Anemia
Etiology
- Folate requirements increase 5-10 fold in pregnancy
- Risk factors: multiple gestation, hyperemesis gravidarum, antiepileptic drugs (phenytoin, phenobarbitone), alcoholism, malnutrition, malabsorption
Clinical Features
- Megaloblastic (macrocytic) anemia
- Glossitis, angular stomatitis
Complications
- Neural tube defects (most important - spina bifida, anencephaly)
- Placental abruption, preeclampsia, preterm birth, spontaneous abortion
Diagnosis
- Macrocytic anemia with hypersegmented neutrophils on smear
- Low serum folate, low RBC folate (RBC folate is more reliable for chronic deficiency)
Treatment / Prevention
| Indication | Dose |
|---|---|
| All pregnant women (routine) | 0.4 - 0.8 mg/day |
| Known folate deficiency | 1.0 mg/day |
| Prior neural tube defect pregnancy | 4.0 mg/day (start 1 month pre-conception, continue to 12 weeks) |
3. Sickle Cell Disease (SCD) in Pregnancy
Complications
- Maternal: 6-fold increased maternal death risk, frequent painful crises, VTE (1.7-10x more common), preeclampsia, PROM, infections, increased cesarean rate
- Fetal: Placental infarction, low birthweight, small-for-gestational-age, preterm birth
Management
- Treat pain crises as in nonpregnant patients
- Hydroxyurea - CONTRAINDICATED (teratogenic)
- NSAIDs - avoid after 30 weeks
- Regional anesthesia preferred for cesarean (general anesthesia increases sickling)
- Iron supplementation controversial (risk of iron overload)
- VTE prophylaxis
4. Thalassemia in Pregnancy
- Alpha-thalassemia trait: Mild microcytic anemia; MCV disproportionately low relative to Hb; RBC count normal or high; RDW normal - distinguishes it from IDA
- Beta-thalassemia trait: HbA2 > 3.5% on Hb electrophoresis; requires partner testing and genetic counseling
- Hb Bart's hydrops fetalis (4 alpha-gene deletion): Incompatible with life - universal stillbirth
Key Laboratory Values (Pregnancy-Adjusted)
| Parameter | Normal Range in Pregnancy |
|---|---|
| Hemoglobin | > 11 g/dL |
| MCV | 81-99 µm³ |
| Serum ferritin | > 20 µg/L |
| Transferrin saturation | 16-60% |
| TIBC | Increases (up to 580-597 µg/dL in T3) |
| Serum folate | 8-240 µg/L |
| HbA2 (electrophoresis) | < 3.5% |
Differential Diagnosis of Anemia Types by CBC Pattern
| Finding | Suggests |
|---|---|
| Low MCV, low RBC, high RDW | IDA |
| Low MCV, normal/high RBC, normal RDW | Thalassemia trait |
| High MCV, hypersegmented neutrophils | Folate / B12 deficiency |
| Normal MCV, positive Coombs | Hemolytic anemia |
| Normal MCV, reticulocytosis | Blood loss / hemolysis |
Summary Points (Quick Recall)
- Most common cause of anemia in pregnancy = Iron deficiency (75%)
- Most sensitive test for IDA = Serum ferritin (< 30 ng/mL)
- IV iron preferred in T3 and severe IDA; not in T1
- Folate 4 mg/day required for prior NTD pregnancy
- Hydroxyurea contraindicated in SCD during pregnancy
- Physiologic anemia: MCV and MCHC remain normal - reassure, no treatment needed
- Hb nadir at 26-34 weeks due to plasma volume expansion
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Rosen's Emergency Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.