explain me 10 common heart diseases with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Searching the Web
common heart diseases ECG changes patterns images cardiology
Finding Sources
Finding Sources
Searching the Web
ECG images STEMI atrial fibrillation heart block WPW LVH pericarditis site:litfl.com OR site:ecgwaves.com
Finding Sources
Searching the Web
ECG examples STEMI atrial fibrillation complete heart block WPW syndrome LVH pericarditis
Reading File
Reading Web Page
https://litfl.com/anterior-myocardial-infarction-ecg-library
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have excellent textbook content and key ECG images. Let me compile the comprehensive answer now.
10 Common Heart Diseases: ECG Changes & Images
Here is a detailed breakdown of 10 common cardiac conditions, their ECG hallmarks, and visual examples drawn from Braunwald's Heart Disease, Harrison's Principles, Guyton & Hall Physiology, and LITFL/clinical sources.
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes full-thickness (transmural) ischemia. A "current of injury" develops between the infarcted and normal zones.
ECG Changes (sequential evolution):
- Hyperacute T waves - tall, peaked T waves within minutes of onset
- ST elevation - convex-upward (tombstone) elevation in leads over the infarcted territory
- Reciprocal ST depression in leads opposite the infarct zone
- Pathological Q waves - develop within hours to days (necrosis)
- T-wave inversions follow in the same leads
- Lead localisation:
- Anterior (V1-V4): LAD occlusion
- Inferior (II, III, aVF): RCA or LCx occlusion
- Lateral (I, aVL, V5-V6): LCx occlusion
Harrison's, p. 1916: "Severe, acute ischemia lowers the resting membrane potential and shortens the duration of the action potential... current flows between those regions. When the acute ischemia is transmural, the ST vector usually is shifted in the direction of the outer (epicardial) layers, producing ST elevations and sometimes hyperacute T waves over the ischemic zone."
ECG Image - Anterolateral STEMI:
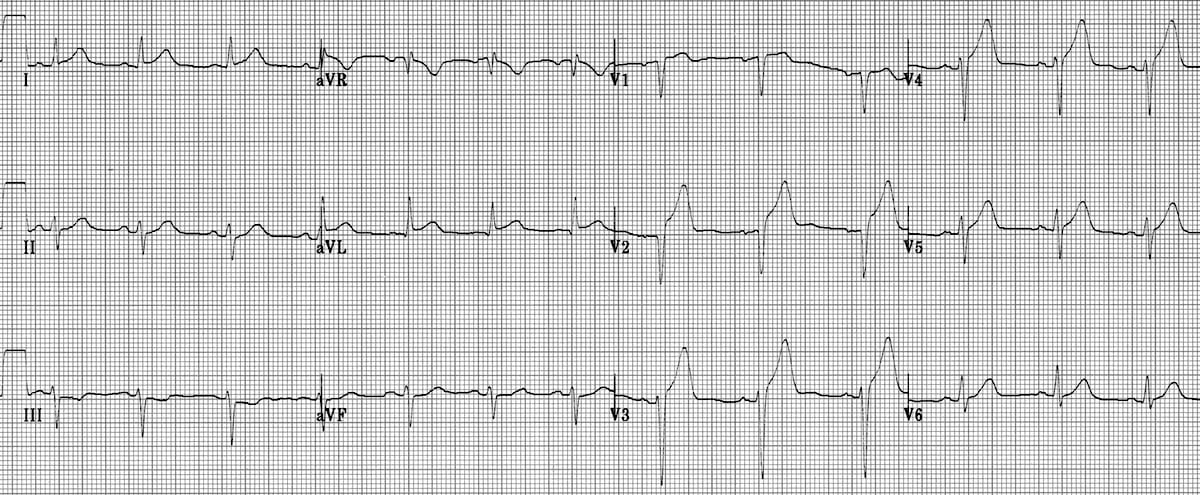
(From LITFL ECG Library - ST elevation maximal in V1-V4 with reciprocal depression in inferior leads)
2. NSTEMI / Unstable Angina
Pathophysiology: Partial coronary occlusion causes subendocardial ischemia. The ST vector shifts inward (toward the ventricular cavity), causing overlying leads to show depression rather than elevation.
ECG Changes:
- ST depression (horizontal or downsloping) - often in multiple leads
- T-wave flattening or inversion (especially deep inversions in V1-V4 = Wellens sign, indicating critical LAD stenosis)
- Hyperacute T waves early in course
- No Q waves (no full-thickness necrosis in unstable angina)
- Normal ECG in up to 50% at presentation - serial ECGs mandatory
Harrison's, p. 1916: "With ischemia confined primarily to the subendocardium, the ST vector typically shifts toward the subendocardium and ventricular cavity, so that overlying leads show ST-segment depression (with ST elevation in lead aVR)."
ECG Image - Anterior STEMI evolving / Wellens T waves:

FIGURE 247-12 from Harrison's: "Severe anterior wall ischemia may cause prominent T-wave inversions in the precordial leads (Wellens T wave sign) - usually associated with high-grade stenosis of the LAD."
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, rapid firing from multiple atrial foci (often pulmonary vein triggers). Atrial rate 350-600 bpm; the AV node acts as a gatekeeper, allowing irregular ventricular conduction.
ECG Changes:
- Absent P waves - replaced by fibrillatory baseline (f waves), fine and irregular, best seen in V1 and II
- Irregularly irregular ventricular rate - the hallmark; no two R-R intervals are equal
- Ventricular rate typically 100-160 bpm if uncontrolled
- Narrow QRS unless aberrant conduction or pre-existing bundle branch block
- No organized atrial activity
Guyton & Hall, p. 176: "Because the waves are weak, and many of them are of opposite polarity at any given time, they usually almost completely electrically neutralize one another. Therefore in the ECG one can see either no P waves or only a fine, high-frequency, very low voltage wave record. Conversely, the QRS-T complexes are normal unless there is some pathology of the ventricles, but their timing is irregular."
ECG Image - Atrial Fibrillation (Lead II):

From Guyton & Hall Physiology - note the irregular QRS complexes without identifiable P waves, and fibrillatory baseline
4. Atrial Flutter
Pathophysiology: A single large reentry circuit (typically counterclockwise around the tricuspid annulus) generates organized atrial activity at 250-350 bpm.
ECG Changes:
- Sawtooth flutter waves (F waves) at ~300 bpm - best seen in leads II, III, aVF and V1
- Regular atrial rate - no isoelectric baseline between flutter waves
- 2:1 AV conduction is most common, giving a ventricular rate of ~150 bpm
- Regular (if fixed block ratio) or slightly irregular (variable block) ventricular response
- Narrow QRS unless aberrant conduction
Key clinical tip: Any regular tachycardia at exactly 150 bpm should always prompt suspicion for atrial flutter with 2:1 block.
5. Complete (Third-Degree) Heart Block
Pathophysiology: Complete dissociation between atrial and ventricular electrical activity. The AV node fails to conduct any impulses. The ventricles are driven by a slow escape rhythm from below the block.
ECG Changes:
- P waves present at normal rate (60-100 bpm) - marching through at their own rate
- QRS complexes at a much slower independent rate (20-45 bpm) - wide if junctional below the bundle of His
- No relationship between P waves and QRS - P waves "march through" QRS complexes
- AV dissociation - the defining feature
- Slow ventricular rate (escape rate) - may cause syncope (Stokes-Adams attacks) or hemodynamic compromise
- Caused by: inferior MI (usually transient, narrow QRS escape), anterior MI (worse prognosis, wide QRS), digoxin toxicity, Lyme disease, surgical trauma
Braunwald's Heart Disease: New AV block in infective endocarditis indicates perivalvular extension of infection and is a marker for death - "The occurrence of a new conduction abnormality is a multivariate risk predictor for death associated with IE."
(From ECGguru.com - P waves and QRS march independently; slow ventricular escape rate)
6. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Increased left ventricular muscle mass (from hypertension, aortic stenosis, HCM) generates greater electrical forces during depolarization, producing high-voltage QRS complexes.
ECG Changes:
- Tall R waves in left-sided leads (I, aVL, V5, V6) and deep S waves in right leads (V1, V2)
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥ 35 mm (age > 35)
- Cornell criteria: R in aVL + S in V3 > 28 mm (men) or > 20 mm (women)
- ST depression and T-wave inversion in lateral leads (V5, V6, I, aVL) = "LVH strain pattern" (repolarization abnormality)
- Left axis deviation
- Left atrial enlargement (bifid P wave in II = P mitrale; negative terminal deflection in V1)
- Prolonged QRS may develop
7. Right Bundle Branch Block (RBBB)
Pathophysiology: Delayed or blocked conduction through the right bundle branch causes the right ventricle to depolarize late via slow cell-to-cell conduction rather than the fast Purkinje system.
ECG Changes:
- Wide QRS ≥ 120 ms
- RSR' ("M-shaped" or "rabbit ears") pattern in V1 - the hallmark
- Wide, slurred S wave in I, aVL, V5, V6 (late rightward activation)
- ST depression and T-wave inversion in V1-V3 (secondary repolarization changes - expected with BBB)
- Causes: PE (new RBBB = ominous), anterior MI, congenital heart disease, idiopathic
8. Left Bundle Branch Block (LBBB)
Pathophysiology: Blocked left bundle branch forces the left ventricle to depolarize via the right bundle, creating a slow, abnormal depolarization sequence. New LBBB is a STEMI equivalent.
ECG Changes:
- Wide QRS ≥ 120 ms
- Broad, notched ("M-shaped") R wave in I, aVL, V5, V6 with no septal Q waves
- Deep QS or rS pattern in V1 (dominant S wave)
- Discordant ST changes - ST/T in opposite direction to the main QRS deflection (always)
- New LBBB + chest pain = treat as STEMI (Sgarbossa criteria used to detect superimposed STEMI)
- Causes: severe IHD, dilated cardiomyopathy, hypertension, aortic stenosis
9. Pericarditis
Pathophysiology: Inflammation of the pericardium causes epicardial injury affecting ventricular repolarization diffusely. Unlike MI, changes are diffuse (not territorial) and evolve in distinct stages.
ECG Changes - Four Classic Stages:
- Stage 1 (hours to days): Diffuse concave-up ("saddle-shaped") ST elevation in most leads (except aVR and V1 which show ST depression); PR segment depression (atrial injury) - the most specific finding
- Stage 2 (days): ST normalises; T waves flatten
- Stage 3 (1-3 weeks): Diffuse T-wave inversions
- Stage 4 (weeks to months): ECG normalises
Key ECG features to distinguish from STEMI:
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST shape | Concave up (saddle) | Convex up (tombstone) |
| Distribution | Diffuse, all leads | Territorial (one territory) |
| PR depression | Present | Absent |
| Reciprocal changes | Only in aVR/V1 | Present in multiple leads |
| Q waves | Absent | Develop |
10. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. Part of the ventricle depolarizes early via the accessory pathway (creating a delta wave), while the rest depolarizes through the normal AV node-His-Purkinje system.
ECG Changes:
- Short PR interval < 120 ms (bypass of AV node delay)
- Delta wave - slurred upstroke at the start of the QRS (pre-excitation wave)
- Wide QRS > 120 ms (fusion of accessory + normal pathway depolarization)
- Discordant ST-T changes - secondary to abnormal depolarization
- Type A WPW (left-sided pathway): dominant R in V1 mimics RVH or posterior MI
- Type B WPW (right-sided pathway): dominant S in V1; negative delta waves in inferior leads can mimic inferior MI ("pseudo-infarction pattern")
- Risk: If AF develops with WPW, impulses bypass the AV node's rate-limiting function - can cause VF and sudden death
Harrison's, p. 1916: "Prolongation of QRS duration does not necessarily indicate a conduction delay but may be due to preexcitation of the ventricles via a bypass tract, as in Wolff-Parkinson-White (WPW) patterns."
Quick Summary Table
| # | Condition | Key ECG Features |
|---|---|---|
| 1 | STEMI | ST elevation + Q waves (territorial) |
| 2 | NSTEMI/UA | ST depression + T inversions; no Q waves |
| 3 | Atrial Fibrillation | Irregularly irregular; absent P waves; fibrillatory baseline |
| 4 | Atrial Flutter | Sawtooth flutter waves ~300 bpm; usually 2:1 block |
| 5 | Complete Heart Block | AV dissociation; slow ventricular escape rate |
| 6 | LVH | High-voltage QRS; lateral strain pattern; left axis |
| 7 | RBBB | Wide QRS; RSR' in V1; S wave in lateral leads |
| 8 | LBBB | Wide QRS; M-pattern in V5-V6; QS in V1; discordant ST |
| 9 | Pericarditis | Diffuse concave ST elevation + PR depression; 4 stages |
| 10 | WPW Syndrome | Short PR + delta wave + wide QRS; risk of AF with VF |
Sources:
- Braunwald's Heart Disease (Cardiology), Chapter 61 & 80
- Harrison's Principles of Internal Medicine 22E, Chapter 247
- Guyton & Hall Textbook of Medical Physiology, Chapter 13
- LITFL ECG Library for clinical ECG examples
For an excellent video overview of the most common ECG patterns:
This is a shared conversation. Sign in to Orris to start your own chat.