How to treat Abg analysis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a thorough, well-organized guide:
ABG (Arterial Blood Gas) Analysis - How to Interpret & Treat
What ABG Measures
An ABG directly measures pH, PaCO2, and PaO2, while HCO3- is calculated via the Henderson-Hasselbalch equation:
pH = 6.1 + log10 ([HCO3-] / 0.03 × PaCO2)
Normal Values:
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mmHg |
| HCO3- | 21 - 27 mEq/L |
| PaO2 | 80 - 100 mmHg |
| SpO2 | > 95% |
Step-by-Step Interpretation (6-Step Method)
(Barash Clinical Anesthesia, 9e - Table 16-8)
Step 1 - Identify pH Status
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
Step 2 - Identify Primary Process
| pH | PaCO2 | HCO3- | Disorder |
|---|---|---|---|
| ↓ | ↑ | Normal/↑ | Respiratory acidosis |
| ↓ | Normal/↓ | ↓ | Metabolic acidosis |
| ↑ | ↓ | Normal/↓ | Respiratory alkalosis |
| ↑ | Normal/↑ | ↑ | Metabolic alkalosis |
Step 3 - Assess Compensation
Check whether compensation is appropriate using formulas below. Inappropriate compensation = mixed disorder.
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis (acute) | PaCO2 = 1.5 × [HCO3-] + 8 ± 2 (Winter's formula) |
| Metabolic alkalosis | PaCO2 = 40 + 0.7 × (HCO3- measured - 24) ± 5 |
| Respiratory acidosis (acute) | HCO3- rises ~1 mEq/L per 10 mmHg ↑ PaCO2 |
| Respiratory acidosis (chronic) | HCO3- rises ~3.5-5 mEq/L per 10 mmHg ↑ PaCO2 |
| Respiratory alkalosis (acute) | HCO3- falls ~2 mEq/L per 10 mmHg ↓ PaCO2 |
| Respiratory alkalosis (chronic) | HCO3- falls ~5 mEq/L per 10 mmHg ↓ PaCO2 |
Step 4 - Calculate Anion Gap (AG)
AG = Na+ - (Cl- + HCO3-) - Normal AG is < 13 mEq/L
- Correct for albumin: add 2.5 × (normal albumin - observed albumin) to the AG
- High AG acidosis: MUDPILES (Methanol, Uremia, DKA, Propylene glycol, Isoniazid/Iron, Lactic acidosis, Ethylene glycol, Salicylates)
- Normal AG acidosis: check urine AG
Step 5 - Urine Anion Gap (if non-AG acidosis)
Urine AG = Urine (Na+ + K+ - Cl-)
- Positive urine AG = GI bicarbonate losses (e.g., diarrhea)
- Negative urine AG = Renal bicarbonate losses (e.g., RTA)
Step 6 - Delta-Delta Ratio (if high AG present)
ΔΔ = ΔAG / ΔHCO3-
- < 1.0 = mixed anion gap + non-anion gap acidosis
- 1.0-2.0 = pure anion gap metabolic acidosis
-
2.0 = mixed anion gap acidosis + metabolic alkalosis (or compensated chronic respiratory acidosis)
Treatment by Disorder
1. Respiratory Acidosis (pH ↓, PaCO2 ↑)
Goal: Improve alveolar ventilation
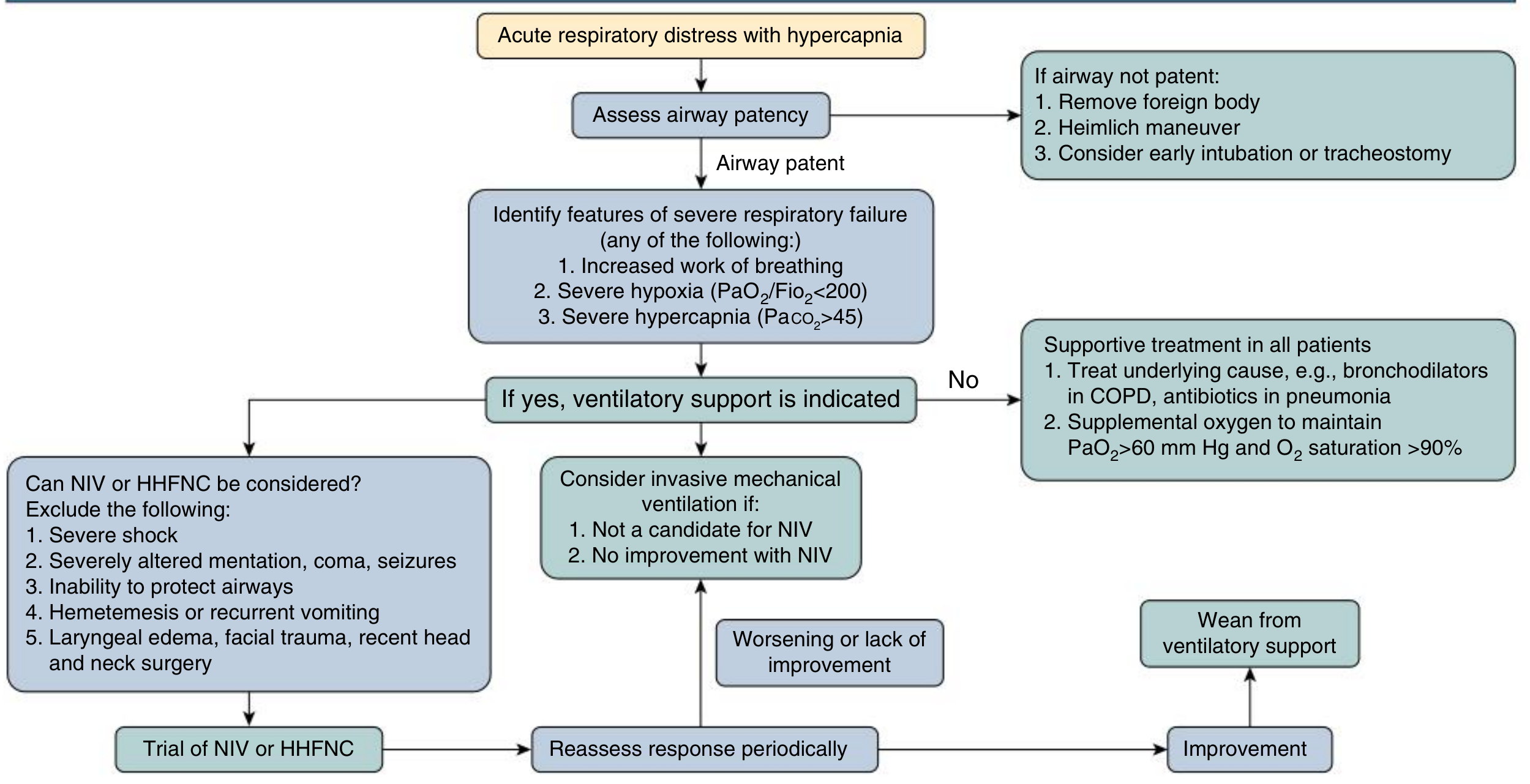
- Treat underlying cause (e.g., bronchodilators in COPD, antibiotics in pneumonia)
- Supplemental oxygen to maintain PaO2 > 60 mmHg and SpO2 > 90%
- NIV (BiPAP/CPAP) if increased work of breathing, PaO2/FiO2 < 200, or PaCO2 > 45 - use if patient is conscious, hemodynamically stable, and able to protect airway
- Invasive mechanical ventilation if: NIV fails, unable to protect airway, severe shock, coma, seizures, hematemesis
- Permissive hypercapnia in ARDS (lung-protective ventilation with TV < 6 mL/kg to keep plateau pressure < 30 mmHg)
- Avoid sodium bicarbonate in respiratory acidosis - it worsens CO2 retention
(Comprehensive Clinical Nephrology, 7e; Barash Clinical Anesthesia, 9e)
2. Metabolic Acidosis (pH ↓, PaCO2 ↓, HCO3- ↓)
Goal: Treat the underlying cause first
- Mild metabolic acidosis (pH > 7.25) - often no emergent treatment needed
- Emergent treatment if: HCO3- < 15 mmol/L or pH < 7.15-7.20
- Sodium bicarbonate (IV): indicated for:
- Renal failure with AKI/CKD metabolic acidosis
- Hyperchloremic/non-AG acidosis
- Renal tubular acidosis (long-term oral NaHCO3 + chloride restriction)
- Controversial in lactic acidosis and DKA - treat the underlying cause primarily
- Monitor for bicarbonate complications: metabolic alkalosis, hypocalcemia, hypokalemia, hypernatremia, volume overload
- DKA: IV fluids, insulin, potassium replacement - bicarbonate rarely needed
- Lactic acidosis: treat the cause (sepsis, shock, hypoxia)
(Brenner & Rector's The Kidney, 2e; Miller's Anesthesia, 10e)
3. Respiratory Alkalosis (pH ↑, PaCO2 ↓)
Goal: Treat the underlying cause
- Reassurance and removal of stressors
- Breathing retraining - diaphragmatic breathing
- Do NOT use paper bag rebreathing - can cause dangerous hypoxemia
- Short-acting benzodiazepines if conservative measures fail
- In mechanically ventilated patients: reduce tidal volume and/or respiratory rate
- Improve sedation and analgesia if patient is breathing over the set rate
- Long-term: cognitive behavioral therapy + treat precipitating conditions
(Comprehensive Clinical Nephrology, 7e)
4. Metabolic Alkalosis (pH ↑, PaCO2 ↑, HCO3- ↑)
Goal: Correct volume and chloride deficits
- Chloride-responsive alkalosis (urine Cl- < 25 mEq/L): give normal saline (0.9% NaCl) or Ringer's lactate to correct hypochloremia and volume contraction
- Contraction alkalosis: correct free water deficit using:
Free water deficit = 0.6 × weight (kg) × ([Na+]/140 - 1) - Chloride-resistant alkalosis (urine Cl- > 40 mEq/L - e.g., hyperaldosteronism, Cushing's): treat the underlying cause, potassium-sparing diuretics
- In mechanically ventilated patients who are chronic CO2 retainers - reduce minute ventilation cautiously to avoid unmasking metabolic alkalosis
(Miller's Anesthesia, 10e; Barash Clinical Anesthesia, 9e)
Quick Acute on Chronic Respiratory Acidosis Distinction
- Acute: PaCO2 > 45, pH < 7.35, HCO3- rises ~1 mEq/L per 10 mmHg ↑ CO2
- Chronic: PaCO2 > 45, pH near-normal (7.35-7.45), HCO3- rises ~3.5-5 mEq/L per 10 mmHg ↑ CO2 (renal compensation over 3-5 days)
- A-a gradient helps identify cause: normal A-a gradient with hypercapnia = hypoventilation/depressed drive; widened A-a gradient (> 20) = pulmonary disease
Key Pearls
- Always draw ABG and venous electrolytes simultaneously - bicarbonate values should match within 2-3 mEq/L; a discrepancy means lab error or timing mismatch
- Always calculate the anion gap even when pH and PaCO2 are normal - a hidden high AG signals a mixed disorder
- For every acute rise in PaCO2 of 10 mmHg, pH falls by 0.08
- Sodium bicarbonate worsens respiratory acidosis - avoid it unless the primary disorder is metabolic
Sources: Barash, Cullen & Stoelting's Clinical Anesthesia 9e | Comprehensive Clinical Nephrology 7e | Brenner & Rector's The Kidney | Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.