Approach to haemorhagic shock : APH
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full, well-structured answer.
Haemorrhagic Shock in APH (Antepartum Haemorrhage)
What is APH?
Antepartum Haemorrhage (APH) is defined as bleeding from the genital tract after 24 weeks of gestation and before delivery of the baby. The two major obstetric causes are:
| Cause | Hallmark Feature |
|---|---|
| Placenta Praevia | Painless, bright-red vaginal bleeding; placenta over/near cervical os |
| Placental Abruption | Painful bleeding; placenta separates prematurely from uterine wall |
Other causes: vasa praevia, local causes (cervical ectropion, polyp, carcinoma), uterine rupture.
Physiological Considerations in Pregnancy
Before applying standard shock protocols, remember that pregnancy alters baseline parameters:
- Blood volume is 40-50% increased by term - pregnant patients must lose a relatively larger volume before showing signs of hypovolaemia. This means standard shock signs appear later and may underestimate the severity of haemorrhage.
- Physiologic anaemia of pregnancy: haematocrit 32-34% at 32-34 weeks due to plasma volume expansion exceeding red cell mass expansion.
- Lower PaCO2 (30 mmHg normally) - a PaCO2 of 40 mmHg in pregnancy actually reflects hypoventilation and impending respiratory acidosis.
- Reduced bicarbonate buffering capacity - vulnerable to metabolic acidosis under stress.
- ECG changes - left axis shift, flattened T waves in lead III - do not misinterpret as pathological.
- Up to 2 litres of blood can accumulate silently in the gravid uterus with abruption, with no or minimal external bleeding.
Classification of Haemorrhagic Shock (ATLS)
| Class | Blood Loss (mL) | Blood Loss (% BV) | Pulse | BP | Pulse Pressure | RR | Urine Output (mL/h) | CNS/Mental Status |
|---|---|---|---|---|---|---|---|---|
| I | Up to 750 | Up to 15% | <100 | Normal | Normal/↑ | 14-20 | >30 | Slightly anxious |
| II | 750-1500 | 15-30% | >100 | Normal | ↓ | >20-30 | 20-30 | Mildly anxious |
| III | 1500-2000 | 30-40% | >120 | ↓ | ↓ | 30-40 | 5-15 | Anxious + confused |
| IV | >2000 | >40% | >140 | ↓ | ↓ | >35 | Negligible | Confused + lethargic |
Important in pregnancy: Vital sign thresholds are less reliable. HR and BP responses are notoriously variable. A normal BP does not exclude significant haemorrhage. Use base deficit and lactate as more sensitive early markers - even before BP falls, base deficit becomes more negative as lactic acid accumulates.
Initial Assessment: ABCDE + Obstetric Survey
Primary Survey (Simultaneous resuscitation and assessment)
A - Airway
- Secure and maintain airway; high-flow oxygen (15 L/min via non-rebreather mask)
- In pregnancy, risk of aspiration is higher (delayed gastric emptying) - rapid-sequence intubation if needed
B - Breathing
- Assess ventilation and oxygenation; SpO2 monitoring
- Target SpO2 ≥95%
C - Circulation
- Establish 2 large-bore IV cannulae (16G or larger) immediately
- Draw blood: FBC, group and crossmatch, coagulation screen (PT, aPTT, fibrinogen, FDPs), U&E, LFTs, ABG, LDH, uric acid
- Fibrinogen normal in pregnancy = 400-450 mg/dL; <300 mg/dL indicates significant coagulation factor consumption (risk of DIC)
- Insert urinary catheter and monitor hourly urine output (target ≥30 mL/h, ideally >0.5 mL/kg/h)
- Continuous cardiac monitoring + pulse oximetry
D - Disability
- GCS/AVPU; pupil assessment
- Altered mental status = severe shock or CNS event
E - Exposure
- Full examination; quantify vaginal blood loss
- Keep warm - prevent hypothermia (part of the "lethal triad": hypothermia + acidosis + coagulopathy)
Differentiation: Placenta Praevia vs. Abruption
| Feature | Placenta Praevia | Placental Abruption |
|---|---|---|
| Pain | Painless | Painful (constant abdominal/back pain) |
| Bleeding | Bright red, revealed | May be concealed (dark); up to 2 L hidden |
| Uterus | Soft, non-tender | Woody-hard, tender ("woody uterus") |
| Fetal presentation | Often malpresentation (high head) | Usually engaged |
| Fetal distress | Variable | Common (most sensitive indicator) |
| Digital VE | ABSOLUTELY CONTRAINDICATED until placenta praevia excluded | Can be done if praevia excluded |
| Coagulopathy (DIC) | Less common | Common (abruption triggers DIC via thromboplastin release) |
Key rule: Never perform digital or instrumental vaginal examination until placenta praevia is excluded by ultrasound. This can precipitate catastrophic haemorrhage.
Diagnostic Investigations
Bedside/Urgent
- Ultrasound (transabdominal ± transvaginal) - investigation of choice for placenta localisation
- Transvaginal USS is safe and more accurate for placenta-os relationship
- Empty bladder first to avoid false-positive praevia
- USS has poor sensitivity for abruption (24% sensitivity, 96% specificity) - a negative USS does NOT rule out abruption
- Cardiotocography (CTG) - fetal heart rate monitoring; most sensitive indicator of placental abruption is fetal distress on CTG
- Minimum 4 hours of monitoring recommended after any significant haemorrhage
- eFAST (in trauma settings) - evaluates for hemoperitoneum, pericardial effusion
Laboratory
- FBC (baseline haemoglobin, haematocrit, platelets)
- Coagulation: PT, aPTT, fibrinogen (key - drops early in DIC), FDPs/D-dimer
- Group and crossmatch (consider activating massive transfusion protocol early)
- Base deficit (on ABG) - early, sensitive marker of occult haemorrhage even before BP falls; normal is > -2 mEq/L
- Lactate - indicator of tissue hypoperfusion
- Kleihauer-Betke test - if Rh-negative mother (quantify fetomaternal haemorrhage)
- U&E, LFTs (exclude HELLP, pre-eclampsia-related causes)
Resuscitation Protocol
Fluid Resuscitation
- Initial: Judicious isotonic crystalloid (10-20 mL/kg) while awaiting blood products
- Permissive hypotension strategy in uncontrolled haemorrhage - avoid aggressive crystalloid resuscitation (worsens coagulopathy, acidosis, hypothermia)
- Blood products - preferred over crystalloid when haemorrhage is severe:
| Situation | Action |
|---|---|
| Poor perfusion + 30-min delay to haemorrhage control | Start packed red blood cells (PRBCs) at 5-10 mL/kg |
| Suspected massive haemorrhage | Immediate PRBCs; initiate Massive Transfusion Protocol (MTP) |
| MTP activated | PRBCs : FFP : Platelets in ratio 1:1:1 |
| Rh-negative mother | Use O-negative PRBCs; give anti-D immunoglobulin 300 μg if not already given at 28 weeks |
- Fresh frozen plasma (FFP) and fresh whole blood may be needed for coagulopathy in APH
- Cryoprecipitate for fibrinogen replacement if fibrinogen <200 mg/dL
- Tranexamic acid (TXA) - early administration (within 3 hours of haemorrhage onset); inhibits fibrinolysis
Treating the Lethal Triad
Target correction of:
- Hypothermia - warm IV fluids, warming blankets, warm environment
- Acidosis - adequate resuscitation, correct base deficit
- Coagulopathy - early FFP, platelets, cryoprecipitate, TXA
Response to Initial Resuscitation
Patients can be categorised into three groups based on response to initial fluid therapy:
| Category | Definition | Implication |
|---|---|---|
| Responder | Normalisation of vitals, mental status, urine output | Haemorrhage likely controlled; proceed with further evaluation |
| Transient Responder | Initial improvement then deterioration | Ongoing haemorrhage - needs urgent definitive intervention |
| Non-Responder | Persistent hypotension despite aggressive resuscitation | Immediate source identification + surgical/interventional haemorrhage control |
Obstetric Management (Definitive Haemorrhage Control)
Placenta Praevia
- Obstetric consultation immediately; arrange transfer to tertiary obstetric facility
- Delivery - typically emergency Caesarean section (avoid vaginal delivery in major praevia)
- Minor praevia with stable patient - conservative management with close monitoring possible; corticosteroids for fetal lung maturity if preterm
- Avoid all digital cervical examination
Placental Abruption
- Mild (< 25% separation, stable mother + fetus): Expectant management with close monitoring; tocolytics generally not recommended (may mask symptoms)
- After 32 weeks or unstable: Delivery indicated (risk of further separation > benefit of prematurity)
- Severe abruption / DIC / fetal distress: Emergency delivery (Caesarean or expedited vaginal delivery depending on cervical status)
- Watch for DIC - coagulation factors consumed by thromboplastin released from injured placenta
- Tocolytics are contraindicated if abruption is the cause of preterm contractions
DIC Management (complicating APH)
- Correct underlying cause (deliver)
- FFP 15 mL/kg for clotting factor replacement
- Cryoprecipitate for fibrinogen <100 mg/dL
- Platelet transfusion if <50 × 10⁹/L (or <75 × 10⁹/L with ongoing haemorrhage)
- Consider recombinant Factor VIIa in refractory cases
Surgical Options for Uncontrolled Haemorrhage
- Uterine compression sutures (B-Lynch)
- Uterine artery ligation / internal iliac artery ligation
- Balloon tamponade (intrauterine)
- Interventional radiology - uterine artery embolisation (in stable patients)
- Peripartum hysterectomy - last resort for life-threatening haemorrhage
Monitoring Targets
| Parameter | Target |
|---|---|
| SpO2 | ≥95% |
| Urine output | ≥30 mL/h (>0.5 mL/kg/h) |
| Systolic BP | Maintain perfusion (MAP 65 mmHg) |
| Temperature | ≥36°C |
| Haemoglobin | ≥70-80 g/L |
| Fibrinogen | ≥200 mg/dL |
| Platelets | ≥50 × 10⁹/L |
| Base deficit | Better than -6 mEq/L |
Special Considerations
- Fetal monitoring: CTG must be continuous once fetal viability is established; fetal distress is the most sensitive indicator of abruption. Fetal heart rate < 110 bpm with maternal hypotension and acidosis predicts poor fetal outcome.
- Perimortem Caesarean section: If maternal cardiac arrest, perform within 4-5 minutes if fetus is viable to optimise maternal resuscitation (removes aortocaval compression).
- Aortocaval compression: Displace uterus to the left (manual or 15-degree left lateral tilt) to relieve compression on the inferior vena cava in all pregnant patients ≥20 weeks gestation.
- REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) - emerging adjunct for haemorrhage control pending surgical intervention.
Summary Algorithm for APH with Haemorrhagic Shock
APH Presenting with Shock
│
▼
ABCDE Primary Survey + Simultaneous Resuscitation
- O2, IV access ×2, bloods (FBC, coag, G+XM, ABG)
- Left lateral tilt (≥20 weeks)
- Foley catheter, monitor UO
│
▼
Immediate Investigations
- USS: localise placenta (praevia vs. abruption)
- CTG: fetal monitoring (most sensitive for abruption)
- NO digital VE until praevia excluded
│
▼
Resuscitate: Crystalloid → PRBCs → MTP (1:1:1)
- Treat lethal triad: warm, correct acid, correct coagulopathy
- Tranexamic acid early
- Anti-D for Rh-negative mothers
│
├── Placenta Praevia → Emergency LSCS
│
└── Placental Abruption
├── Stable + partial (<25%) → Expectant (if <32 wks)
└── Unstable / Severe / >32 wks → Deliver (LSCS or expedited vaginal)
│
└── DIC → FFP + Cryoprecipitate + Platelets + TXA
Sources:
- ROSEN's Emergency Medicine, 9e - Haemorrhagic Shock, Placenta Previa, Placental Abruption
- Schwartz's Principles of Surgery, 11e - Signs & Symptoms of Hemorrhagic Shock (Table 7-4); Damage Control Resuscitation
- Creasy & Resnik's Maternal-Fetal Medicine - Effect of Pregnancy on Haemostasis
- Textbook of Family Medicine, 9e - Abruptio Placentae

image.png
according to this learning outcome
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the content needed to deliver a comprehensive answer covering all 6 learning outcomes. Let me compile the full response.
APH: Complete Notes Based on Learning Outcomes
LO 1 - Definition of Antepartum Haemorrhage
APH is defined as bleeding from the genital tract after 24 weeks of gestation and before the onset of labour (or delivery of the baby).
- Incidence: affects approximately 3-5% of pregnancies
- It is a major cause of maternal and perinatal morbidity and mortality worldwide
- Bleeding may be revealed (external, visible) or concealed (blood pools behind placenta - may have NO visible bleeding but severe maternal compromise)
LO 2 - Causes, Clinical Features, and Complications of APH
Causes (in order of clinical importance)
| Cause | Approximate % |
|---|---|
| Placental abruption | ~30% |
| Placenta praevia | ~20% |
| Vasa praevia | Rare |
| Indeterminate / local causes | ~50% |
Local causes include: cervical ectropion, cervical polyp, cervicitis, cervical carcinoma, varicosities, vaginal lacerations.
Key rule: Do NOT perform a digital or speculum pelvic examination to assess vaginal bleeding in APH until transvaginal ultrasound has confirmed the location of the placenta. Mechanical disruption of the placenta by speculum or digital examination may precipitate catastrophic haemorrhage.
General Clinical Features of APH
- Vaginal bleeding after 24 weeks (may be bright red or dark)
- May be painless (praevia) or painful (abruption)
- Uterine tenderness, contractions
- Signs of maternal shock: tachycardia, hypotension, pallor, diaphoresis
- Fetal distress on CTG
Complications
Maternal:
- Haemorrhagic shock
- DIC (especially with abruption)
- Renal failure (from ischaemia)
- Pituitary necrosis (Sheehan's syndrome) from prolonged hypotension
- Peripartum hysterectomy
- Death
Fetal/Neonatal:
- Fetal distress, hypoxia, acidosis
- Intrauterine death (fetal mortality ~15% with abruption overall; 100% with severe complete abruption if not immediately delivered)
- Prematurity and its sequelae
- Growth restriction
LO 3 - Initial Management Approach to APH
This applies to ALL cases of APH regardless of cause, while diagnosis is being established.
Step 1 - Immediate Stabilisation (Simultaneous Assessment + Resuscitation)
A - Airway: Secure; high-flow O2 (15 L/min via non-rebreather mask); SpO2 ≥95%
B - Breathing: Assess ventilation; avoid hypoxia (fetoplacental perfusion depends on maternal O2)
C - Circulation:
- Establish 2 large-bore IV cannulae (16G or larger) immediately
- IV fluid resuscitation: crystalloid initially (10-20 mL/kg); then blood products if haemodynamically unstable
- Left lateral tilt (≥20 weeks) - prevents aortocaval compression by gravid uterus
- Insert urinary catheter; monitor urine output (target ≥30 mL/h)
- Continuous maternal cardiac monitoring + pulse oximetry
D - Disability: GCS/AVPU; altered consciousness = severe shock
E - Exposure: Full examination; estimate blood loss; keep warm (hypothermia worsens coagulopathy)
Step 2 - Investigations
| Investigation | Rationale |
|---|---|
| FBC (CBC) | Haemoglobin, haematocrit, platelets |
| Group & crossmatch | Emergency transfusion readiness |
| Coagulation screen: PT, aPTT, fibrinogen, FDPs/D-dimer | DIC screening - fibrinogen normal in pregnancy = 400-450 mg/dL; <300 mg/dL = significant consumption |
| U&E, LFTs | Renal function, exclude HELLP, pre-eclampsia |
| ABG (base deficit, lactate) | Sensitive early marker of occult haemorrhage even before BP falls |
| Kleihauer-Betke | If Rh-negative mother - quantifies fetomaternal haemorrhage |
| Transvaginal USS | Placenta localisation - FIRST before any vaginal examination |
| CTG | Fetal wellbeing - most sensitive for abruption |
Step 3 - Urgent Obstetric Consultation
- Arrange immediate obstetric review and/or transfer to tertiary facility with obstetric + neonatal services
- If Rh-negative and not yet received prophylaxis at 28 weeks: anti-D immunoglobulin 300 μg
Step 4 - Blood Transfusion / Massive Transfusion Protocol (if needed)
- PRBCs for significant blood loss; if massive haemorrhage: activate MTP with 1:1:1 ratio (PRBCs : FFP : Platelets)
- FFP and cryoprecipitate for DIC
- Tranexamic acid (TXA) early - inhibits fibrinolysis
- O-negative blood until type-specific available
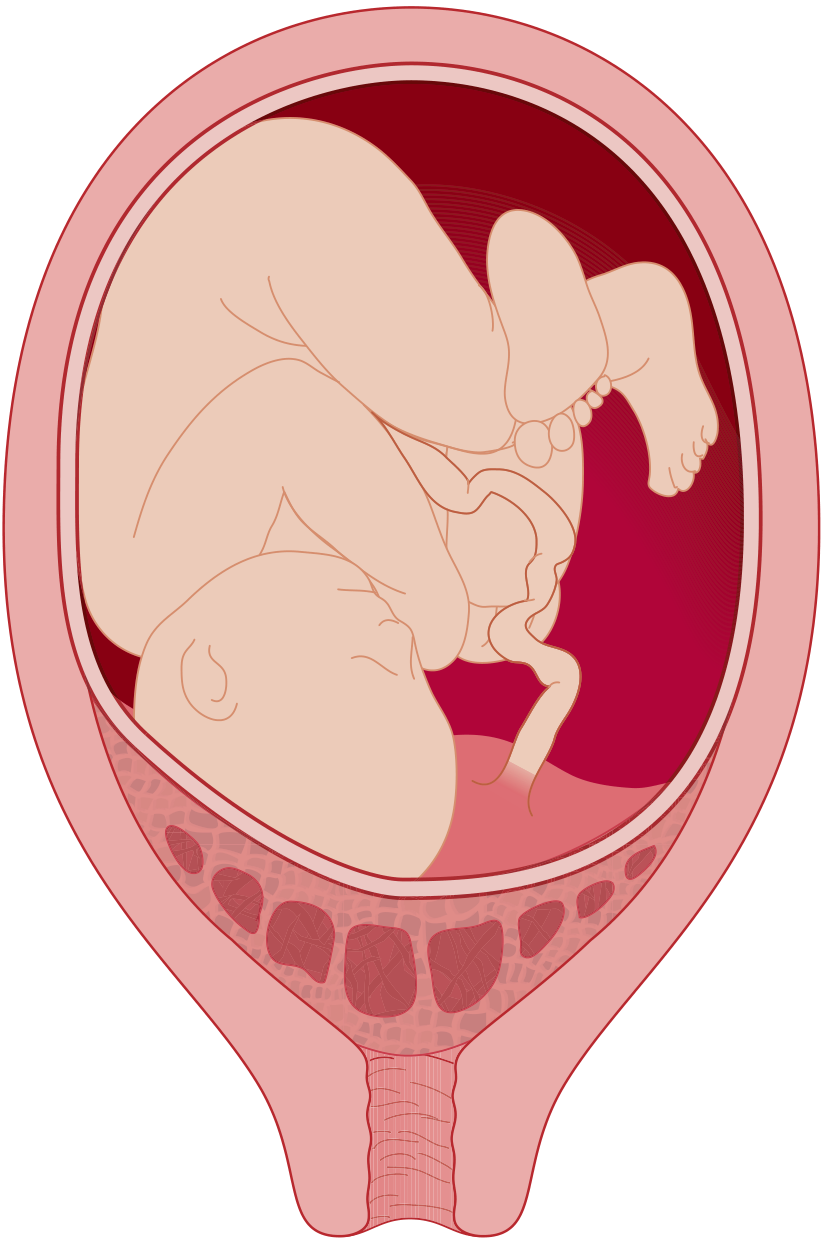
LO 4 - Abruptio Placentae: Clinical Features, Investigations & Management
Definition
Premature separation of a normally implanted placenta from the uterine lining before delivery of the fetus. Incidence is highest between 24-32 weeks.
Pathophysiology
Spontaneous haemorrhage into the decidua basalis → hematoma formation → placental separation → compression of placental vessels → uteroplacental insufficiency. With large separation, retroplacental blood may penetrate the uterine wall into the peritoneal cavity (Couvelaire uterus). The injured placenta releases thromboplastin into maternal circulation, triggering DIC. Plasminogen activator release also drives fibrinolysis.
Risk Factors
- Hypertension and pre-eclampsia (40-50% of cases)
- Abdominal trauma (motor vehicle accidents, intimate partner violence)
- Cocaine use
- Smoking
- Advanced maternal age (>35) or young age (<20)
- High parity (≥3)
- Prior abruption
- Chorioamnionitis, oligohydramnios
- Thrombophilia
Types
| Type | Blood | Pain | Fetal Status |
|---|---|---|---|
| Revealed | Visible vaginal bleeding | Present | Variable |
| Concealed | Blood trapped behind placenta; no external bleeding | Severe | Poor |
| Mixed | Both | Variable | Variable |
Grades of Severity
| Grade | Features |
|---|---|
| Mild | Slight vaginal bleeding, little uterine irritability, no fetal distress, normal coagulation |
| Moderate | Increased bleeding (or concealed loss), increased uterine irritability/tetanic contractions, declining fibrinogen, fetal distress, maternal tachycardia |
| Severe (15% of cases) | Tetanically contracted woody uterus, maternal hypotension, fibrinogen <150 mg/dL, fetal death possible |
Clinical Features (the classic triad)
- Painful vaginal bleeding - dark blood (70% of patients)
- Uterine tenderness with "woody hard" or tetanic uterus (in severe cases)
- Fetal distress on CTG (most sensitive indicator)
- Nausea, vomiting, back pain may be present
- Up to 10% have only occult bleeding with NO external haemorrhage
- Up to 2 litres of blood can be sequestered in the gravid uterus
- Uterine contractions are often 1-2 minutes apart with high baseline pressure
Investigations
| Test | Finding/Significance |
|---|---|
| CTG | Most sensitive - fetal distress; 100% negative predictive value when reassuring |
| Transvaginal USS | Specific but NOT sensitive (24% sensitivity) - retroplacental haematoma; variable echogenicity evolves over time; normal USS does NOT exclude abruption |
| Fibrinogen | <150 mg/dL = severe; first clotting factor to fall |
| Coagulation screen | PT/aPTT prolonged in DIC |
| FBC | Anaemia; thrombocytopaenia in DIC |
| Kleihauer-Betke | Fetomaternal haemorrhage; important for Rh-negative mothers |
| ABG/base deficit | Severity of maternal haemorrhage |
| MRI | Diagnostic but impractical in emergency |
Management
Immediate:
- 2 large-bore IVs, bloods, maternal stabilisation
- Continuous CTG monitoring
- Emergency obstetric consultation
- Anti-D if Rh-negative
Definitive (depends on severity and gestation):
| Scenario | Management |
|---|---|
| Mild abruption, stable mother + fetus, <32 weeks, <25% separation | Expectant management with close monitoring; corticosteroids for fetal lung maturity |
| After 32 weeks or unstable | Delivery (risk of further separation > benefit of prematurity) |
| Severe abruption / DIC / fetal distress | Emergency delivery (LSCS preferred if fetus alive; expedited vaginal if fetal demise and mother stable) |
| Tocolytics | Generally NOT recommended - most contractions are driven by abruption itself (contraindicated in abruption); stop if cervix dilated ≥4 cm |
DIC management: FFP + cryoprecipitate (fibrinogen replacement) + platelets + TXA
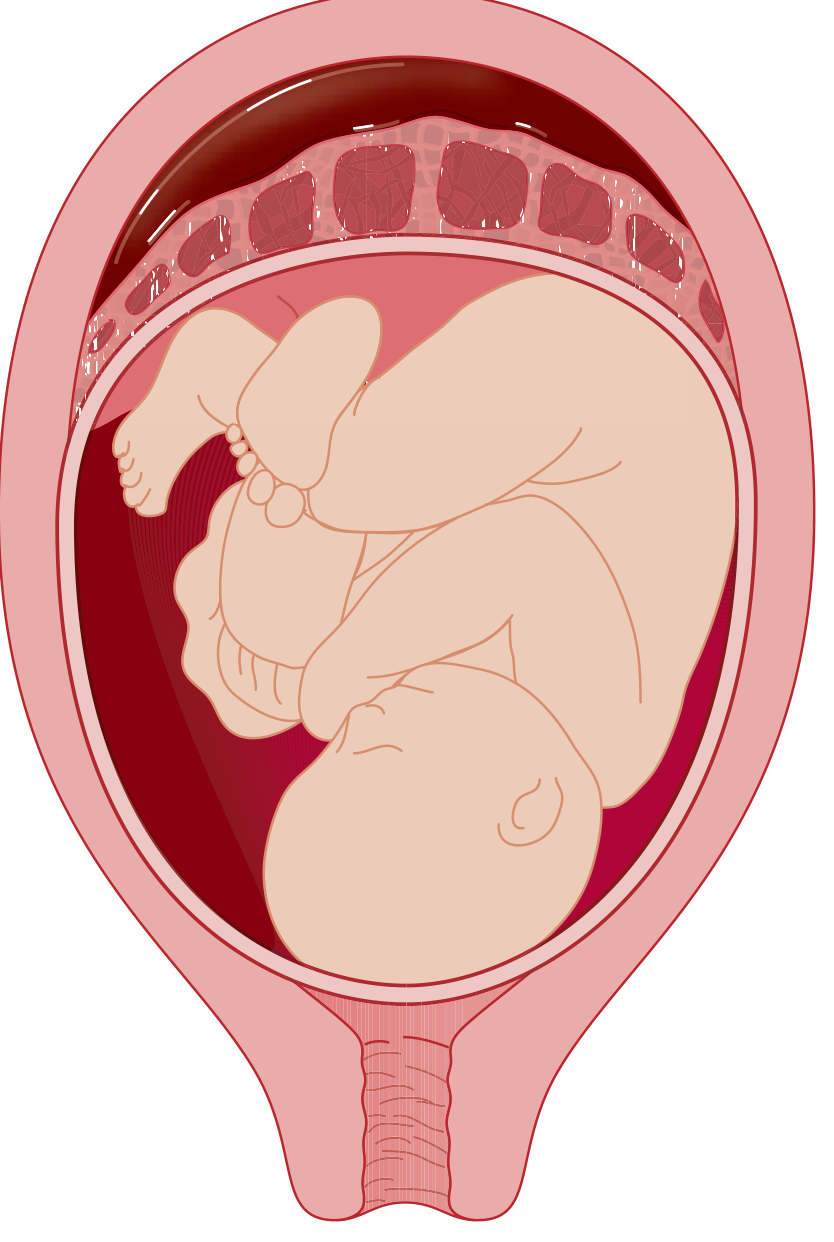
LO 5 - Placenta Praevia: Clinical Features, Investigations & Management
Definition
Implantation of the placenta over or near the internal cervical os. Normal implantation is at the corpus/fundal region. Incidence: ~1 in 200-250 pregnancies.
Types (Classification)
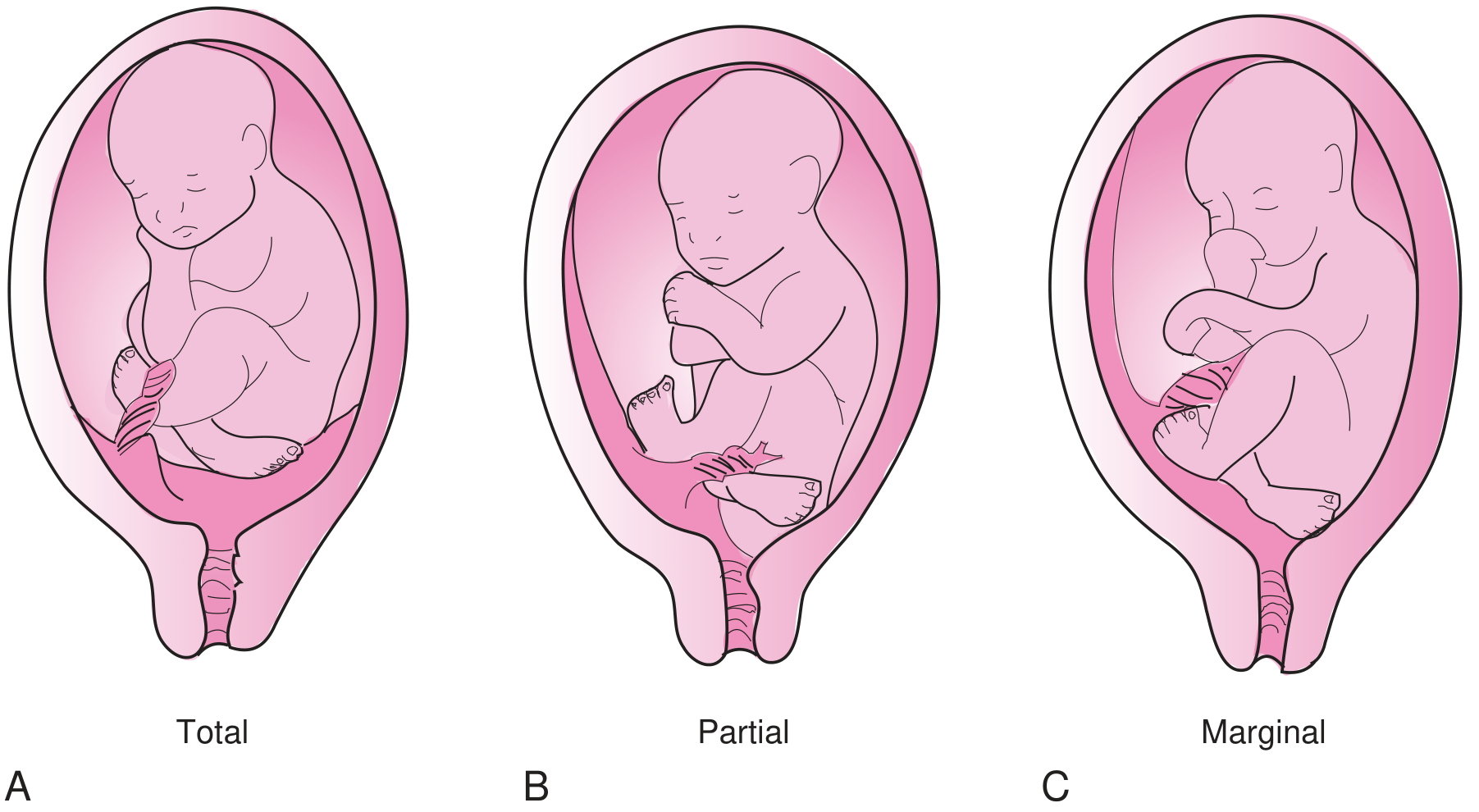
| Type | Description |
|---|---|
| Complete / Total | Placenta completely covers the internal os |
| Partial | Placenta partially covers the internal os |
| Marginal | Placenta reaches the internal os but does not cover it |
| Low-lying | Placenta implanted in lower uterine segment but does not reach the os |
Placental migration: Up to 90% of placentae diagnosed as praevia on 2nd trimester USS resolve by term as the lower uterine segment elongates. Central previa (20% of cases) is less likely to migrate and carries highest haemorrhage risk.
Risk Factors
- Previous Caesarean section (most important - risk increases with number of prior sections)
- Multiple uterine surgeries
- Advanced maternal age
- Multiparity
- Multiple gestation
- Tobacco / cocaine use
- Prior placenta praevia
- Assisted reproductive technology
- Prior miscarriage or induced abortion
Clinical Features
- Painless, bright-red, fresh vaginal bleeding - hallmark; this is the key differentiator from abruption
- Typically begins at 27-32 weeks (average first bleed)
- Initial bleeding is often self-limited, then recurs
- Women with central praevia bleed earlier and more severely
- Soft, non-tender uterus
- Fetal malpresentation common (transverse or breech) - floating, unengaged presenting part
- ~20% have some uterine irritability, but this is minor
Investigations
| Test | Details |
|---|---|
| Transvaginal USS | Investigation of choice; accuracy 93-98%; safe when performed correctly (probe angled against anterior lip of cervix, NOT advanced into cervix, NOT touching placenta); empty bladder first (full bladder causes false-positive praevia); transvaginal more accurate than transabdominal |
| Transabdominal USS | Good first-line screening; 93-98% accuracy |
| FBC, coagulation, G+XM | Standard haemorrhage workup |
| CTG | Fetal monitoring |
| NEVER digital VE | Absolutely contraindicated until praevia excluded - can precipitate torrential haemorrhage |
Management
Acute episode:
- 2 large-bore IVs; fluid/blood resuscitation; obstetric consultation
- Continuous CTG monitoring
- Baseline fibrinogen (normal in pregnancy = 400-450 mg/dL)
- Do NOT perform speculum or digital examination until placental position confirmed
- Anti-D if Rh-negative
Definitive (by obstetrician):
| Situation | Management |
|---|---|
| Stable, minor praevia, preterm | Admission, bed rest, close monitoring; corticosteroids for fetal lung maturity if <34 weeks |
| Major/complete praevia | Elective LSCS at 36-37 weeks (before labour starts) |
| Active haemorrhage, unstable / term | Emergency LSCS |
| Placenta within 1-2 cm of os, labour imminent | "Double setup" examination in the OR with teams ready for immediate LSCS |
| Placenta accreta suspected | Plan for obstetric haemorrhage management; consider interventional radiology pre-operatively |
LO 6 - Indeterminate APH, Local Causes, and Vasa Praevia
Indeterminate APH
- Accounts for approximately 50% of all APH cases
- No placenta praevia on USS, no clinical/ultrasound features of abruption
- Includes small subclinical marginal abruptions, decidual bleeding
- Management: treat empirically as significant APH until cause found; close monitoring; CTG
- Many resolve spontaneously but carry residual risk of preterm labour and fetal growth restriction
Local Causes of APH
These arise from the lower genital tract and are NOT placental in origin:
| Local Cause | Features |
|---|---|
| Cervical ectropion (erosion) | Common in pregnancy (oestrogen effect); bleeds on contact; painless; seen on speculum; NOT dangerous |
| Cervical polyp | Pedunculated, bleeds easily on contact; benign; usually not urgent |
| Cervicitis / vaginitis | Infection-related; associated discharge; swabs needed |
| Cervical carcinoma | Post-coital/contact bleeding; irregular cervix on examination; urgent colposcopy/biopsy required |
| Vaginal lacerations | May follow trauma; obvious on speculum |
| Vulvovaginal varicosities | Can rupture in pregnancy |
These causes can only be assessed AFTER placenta praevia has been excluded by ultrasound. Only then should a careful speculum examination be done.
Vasa Praevia
Definition: A rare but catastrophic condition in which unprotected fetal blood vessels (not covered by Wharton's jelly or placental tissue) traverse the fetal membranes across the cervical os, lying between the fetal presenting part and the internal os.
Pathophysiology: Almost always associated with velamentous cord insertion (cord inserts into membranes rather than directly into the placenta). When membranes rupture (spontaneously or artificially), the unprotected fetal vessels tear, causing fetal exsanguination - because the blood lost is FETAL blood, even small amounts are catastrophic.
Risk Factors:
- Velamentous cord insertion
- Placenta praevia
- Bilobed or succenturiate lobe placenta
- In vitro fertilisation (IVF)
- Multiple gestation
Clinical Features:
- Classic triad: Painless bleeding + rupture of membranes + acute fetal distress / sudden fetal bradycardia
- Blood is fetal in origin - very small volumes (100-200 mL) can cause fetal shock
- Pulsatile vessels may be palpated before the presenting part on digital examination (if done)
- Fetal heart rate may be sinusoidal or show deep, late decelerations
- Fetal mortality: 33-100% if not diagnosed/managed before rupture
Investigations:
- Colour Doppler USS - can identify aberrant vessels at the internal os early in pregnancy (primary screening tool)
- At time of acute bleeding: Apt test / Kleihauer test on vaginal blood - confirms fetal haemoglobin (fetal origin)
- CTG: fetal distress is rapid and severe
- Often a retrospective diagnosis after emergency LSCS for fetal distress
Management:
- Emergency LSCS is the treatment - there is NO time for conservative management once bleeding starts
- Antenatal diagnosis by Doppler USS allows planned elective LSCS before 36-37 weeks (before membrane rupture)
- If diagnosed antenatally: close monitoring, hospital admission near term, avoid artificial rupture of membranes
- Fetal mortality dramatically reduced with antenatal diagnosis and planned delivery
Quick Comparison: The Three Major Causes of APH
| Feature | Placenta Praevia | Abruptio Placentae | Vasa Praevia |
|---|---|---|---|
| Pain | None | Painful | None (until fetal distress) |
| Bleeding | Bright red, revealed | Dark, may be concealed | Bright red, fetal |
| Onset | After 24 weeks, peaks 27-32 wks | Any time | At membrane rupture |
| Uterus | Soft, non-tender | Tender, woody-hard | Normal |
| Fetal presentation | Malpresentation common | Usually normal | Normal |
| Coagulopathy | Rare | Common (DIC) | No (fetal loss) |
| Fetal compromise | Variable | Common | Rapid, severe |
| Blood is... | Maternal | Maternal | Fetal |
| Digital VE | Absolutely contraindicated | Can do if praevia excluded | Avoid/dangerous |
| USS | Definitive diagnosis | Low sensitivity (24%) | Colour Doppler useful |
| Definitive treatment | LSCS (usually) | Depends on severity | Emergency LSCS |
Sources:
- Tintinalli's Emergency Medicine, 9e - Abruptio Placentae, Placenta Praevia, Vasa Praevia (pp. 674-676)
- ROSEN's Emergency Medicine, 9e - Abruptio Placentae, Placenta Praevia
- Textbook of Family Medicine, 9e - Abruptio Placentae, Placenta Praevia, Vasa Praevia
- Creasy & Resnik's Maternal-Fetal Medicine - Haemostasis in Pregnancy
This is a shared conversation. Sign in to Orris to start your own chat.