Make an answer for pg Orthopaedic exam
cd /home/daytona/workspace/attachments/636c28be-29a7-4534-a72b-f1823d7c51b8/ && …
cd /home/daytona/workspace/attachments/636c28be-29a7-4534-a72b-f1823d7c51b8/ && …
NASCIS Trials and Methylprednisolone in Acute Spinal Cord Injury
Short Note / Essay Answer (PG Orthopaedic Exam)
Introduction
The Three NASCIS Trials
NASCIS I (Bracken et al., 1984, JAMA)
- 330 patients randomized to two different doses of MPSS within 48 hours of blunt SCI
- Primary endpoint: NEGATIVE - no significant difference in motor recovery between doses
- Notably, no placebo arm was included
- Conclusion: dosing was insufficient; a higher dose was needed
NASCIS II (Bracken et al., 1990, NEJM) ★ Most Important
- Three arms: high-dose MPSS vs naloxone vs placebo
- MPSS given within 12 hours of injury (study design)
- Primary endpoint: NEGATIVE (no significant benefit overall)
- However, a post hoc subgroup analysis of patients treated within 8 hours of injury showed improved neurologic recovery with MPSS
- Protocol (memorize this):
- Bolus: 30 mg/kg IV over 15 minutes
- Maintenance: 5.4 mg/kg/hr for 23 hours (infusion started 45 minutes after bolus)
- Total duration: 24 hours
NASCIS III (Bracken et al., 1997, JAMA)
- Three arms: MPSS for 24 hours vs MPSS for 48 hours vs tirilazad mesylate for 48 hours
- Again, primary endpoint was negative
- Post hoc subgroup analysis concluded:
- If MPSS started within 3 hours of injury → continue for 24 hours
- If MPSS started 3 to 8 hours after injury → continue for 48 hours
- Tirilazad showed no benefit
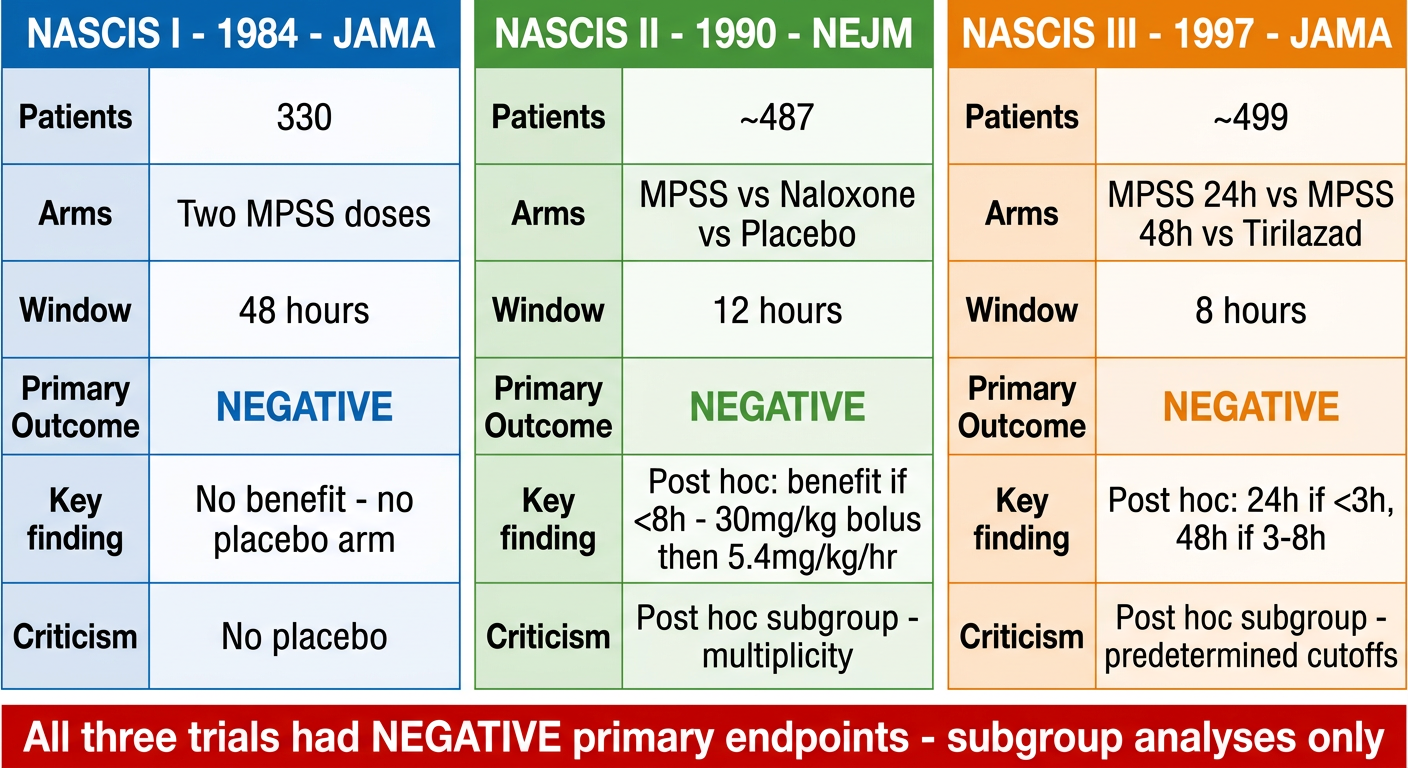
Summary Table: NASCIS Protocols
| Trial | Year | Primary Outcome | Key Finding (Subgroup) |
|---|---|---|---|
| NASCIS I | 1984 | Negative | No benefit; no placebo |
| NASCIS II | 1990 | Negative | Benefit if given < 8 hr (post hoc) |
| NASCIS III | 1997 | Negative | 24 hr if < 3 hr; 48 hr if 3-8 hr (post hoc) |
Current Clinical Protocol (NASCIS II)
| Step | Dose | Timing |
|---|---|---|
| Bolus | 30 mg/kg IV | Over 15 minutes |
| Infusion | 5.4 mg/kg/hr | For 23 hours (start 45 min after bolus) |
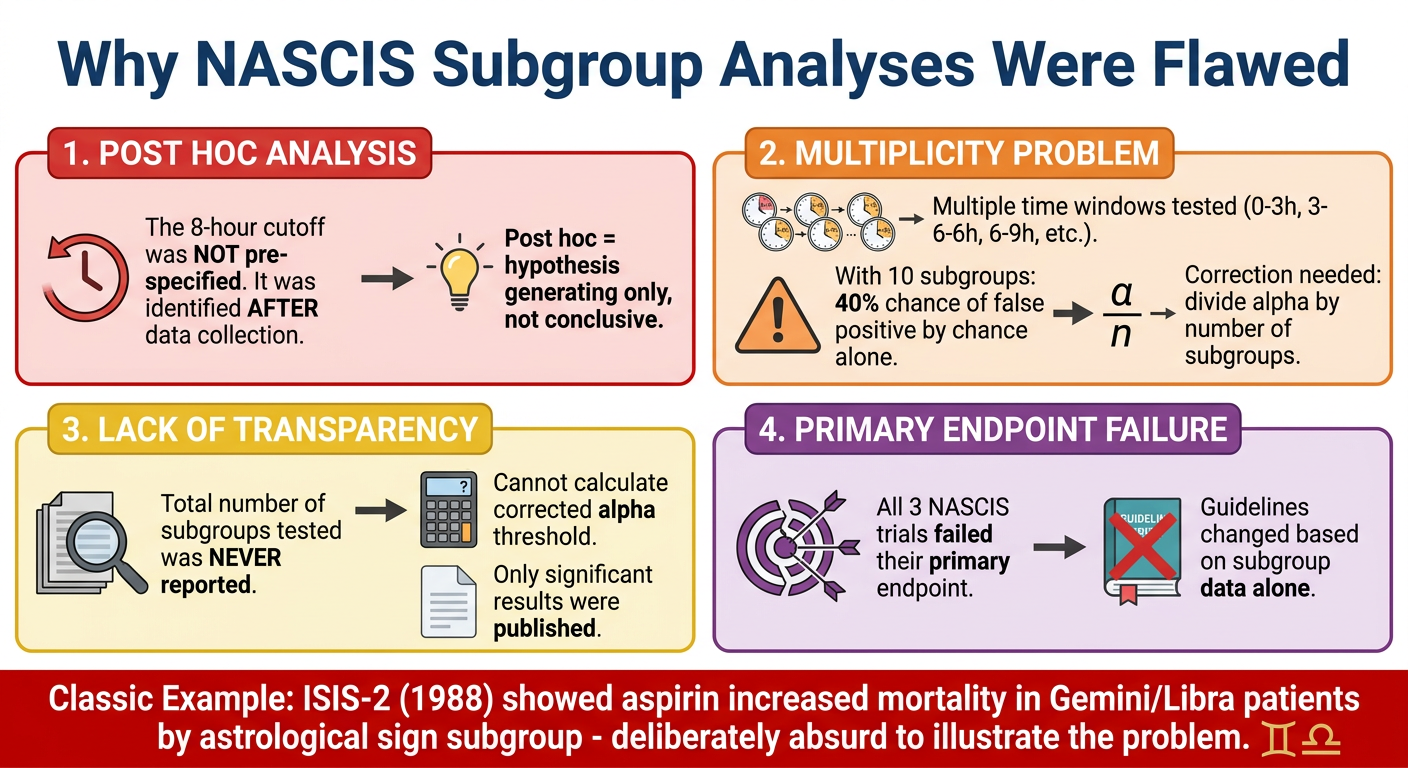
Criticisms of the NASCIS Trials (Exam Favorite)
1. Post Hoc Subgroup Analysis
- The positive results in NASCIS II and III were from subgroups NOT pre-specified in the study protocol
- The 8-hour cutoff in NASCIS II was not predetermined; it was identified after the fact (data mining)
- Post hoc analyses are hypothesis-generating only and should not carry the same weight as primary outcomes
2. Problem of Multiplicity
- When many subgroups are tested, the probability of a false-positive result increases
- With 10 subgroups, chance of a false positive = up to 40%
- Correction: divide alpha (0.05) by number of subgroups tested (e.g., with 10 subgroups, threshold becomes 0.005)
- NASCIS II never reported the total number of subgroups tested, so the appropriate correction could not be applied
3. Lack of Transparency
- NASCIS II designed enrollment for patients within 12 hours, but reported benefit only in the < 8 hour subgroup - other time windows (0-3 h, 3-6 h, 6-9 h) were likely also tested but not reported
4. Primary Endpoint Failure
- Both NASCIS II and III failed their primary endpoints; only subgroup analyses were positive
- Guidelines were nonetheless changed based on these subgroup results
5. Adverse Effects of High-Dose Steroids
- Wound infection, sepsis, pneumonia, gastrointestinal bleeding (requires GI prophylaxis)
- Hyperglycemia
- Worsening of other organ injuries in polytrauma patients
- Particularly harmful in elderly patients with comorbidities
Classic Analogy Illustrating Subgroup Misuse (ISIS-2 Trial)
Contraindications to High-Dose Methylprednisolone in SCI
- Penetrating spinal wounds (especially gunshot wounds)
- Injury > 8 hours old
- Nerve root or cauda equina injury (not cord injury)
- Age < 13 years
- Pregnancy
- Active infection
- Uncontrolled diabetes mellitus
Current Status and Guidelines
- High-dose MPSS for acute SCI is NOT standard of care
- It is considered a treatment option at best, and many centers have discontinued its use entirely
- The waning of MPSS use was driven not by a new RCT but by critical reappraisal of the NASCIS data
- Current guidelines (post-2013) frame it as an option with level III evidence, with full disclosure of risks
Key Points for Viva / Short Notes
- NASCIS = National Acute Spinal Cord Injury Study - 3 trials (1984, 1990, 1997)
- All three trials had negative primary outcomes - the "benefit" came from post hoc subgroups
- NASCIS II dose: 30 mg/kg bolus → 5.4 mg/kg/hr x 23 hrs (< 8 hours of injury)
- NASCIS III: 24 hrs if < 3 hrs; 48 hrs if 3-8 hrs
- Tirilazad mesylate (lipid peroxidation inhibitor) was tested in NASCIS III - no benefit
- Major criticism: post hoc subgroup analysis + multiplicity problem
- Not standard of care today; contraindicated in penetrating SCI, infection, DM, pregnancy
- GI prophylaxis must be co-administered if used
- The 8-hour window is the most important clinical threshold to remember
- ISIS-2 astrological subgroup = classic example of subgroup analysis fallacy
Include flow chart and images
Medical clinical decision flowchart for acute spinal cord injury management using methylprednisolone (NASCIS protocol). Clean white background, professional medical style. Flow starts with "Acute Spinal Cord Injury (Blunt Trauma)" at top. First decision diamond: "Time since injury?". Left branch "<8 hours" leads to second diamond "Contraindications present? (penetrating injury / infection / DM / pregnancy / age <13 / cauda equina)". Yes branch leads to red box "Do NOT give steroids". No branch leads to green box "Give Methylprednisolone". From green box, splits into two paths: left path ">3 hours onset" with blue box "30 mg/kg IV bolus over 15 min, then 5.4 mg/kg/hr for 23 hours (24-hour protocol)"; right path "3-8 hours from onset" with orange box "30 mg/kg IV bolus over 15 min, then 5.4 mg/kg/hr for 47 hours (48-hour protocol)". Right branch from first diamond ">8 hours" leads to red box "Do NOT give steroids - no benefit, increased harm". Bottom note: "Always co-administer GI prophylaxis. Not standard of care - treatment option only." All boxes connected by arrows, color coded, clear font, exam-ready
Medical diagram showing secondary spinal cord injury cascade after primary trauma. Clean white background, professional medical textbook style. Shows a vertical flowchart cascade with labeled boxes and arrows: Top box (red): "Primary SCI - Mechanical trauma, axonal disruption, vascular injury". Arrow down to box (orange): "Immediate: Hemorrhage, ionic shifts (Na+/Ca2+ influx), glutamate excitotoxicity". Arrow down to box (yellow): "Hours: Inflammation - neutrophil/macrophage infiltration, pro-inflammatory cytokines (TNF-α, IL-1β)". Arrow down to box (light orange): "Lipid peroxidation - free radical damage to cell membranes (target of methylprednisolone and tirilazad)". Arrow down to box (purple): "Edema and ischemia - loss of autoregulation, MAP must be maintained >85 mmHg". Arrow down to box (dark red): "Days-weeks: Apoptosis and demyelination". Arrow down to box (grey): "Weeks-months: Glial scar formation - fibrosis, barrier to axonal regeneration". On the right side, a callout arrow pointing to the lipid peroxidation box says "Methylprednisolone acts here - inhibits lipid peroxidation, reduces inflammation". All arrows going downward, color gradient from red to grey, clear professional labels
Medical infographic comparing NASCIS I, NASCIS II and NASCIS III trials side by side. Clean white background, professional exam study card style. Three columns side by side with clear headers: Column 1 header (blue): "NASCIS I - 1984 - JAMA". Column 2 header (green): "NASCIS II - 1990 - NEJM". Column 3 header (orange): "NASCIS III - 1997 - JAMA". Each column has rows for: Patients (330 / ~487 / ~499), Arms (Two MPSS doses / MPSS vs Naloxone vs Placebo / MPSS 24h vs MPSS 48h vs Tirilazad), Window (48 hours / 12 hours / 8 hours), Primary Outcome (NEGATIVE / NEGATIVE / NEGATIVE), Key finding (No benefit - no placebo arm / Post hoc: benefit if <8h - 30mg/kg bolus then 5.4mg/kg/hr / Post hoc: 24h if <3h, 48h if 3-8h), Criticism (No placebo / Post hoc subgroup - multiplicity / Post hoc subgroup - no predetermined cutoffs). At bottom: red banner "All three trials had NEGATIVE primary endpoints - subgroup analyses only". Large clear fonts, color coded columns, grid layout
Medical infographic explaining subgroup analysis problems in clinical trials. Clean white background, professional style for medical exam. Title at top: "Why NASCIS Subgroup Analyses Were Flawed". Four numbered problem boxes arranged in 2x2 grid. Box 1 (red, top-left): "1. POST HOC ANALYSIS - The 8-hour cutoff was NOT pre-specified. It was identified AFTER data collection. Post hoc = hypothesis generating only, not conclusive." Box 2 (orange, top-right): "2. MULTIPLICITY PROBLEM - Multiple time windows tested (0-3h, 3-6h, 6-9h, etc.). With 10 subgroups: 40% chance of false positive by chance alone. Correction needed: divide alpha by number of subgroups." Box 3 (yellow, bottom-left): "3. LACK OF TRANSPARENCY - Total number of subgroups tested was NEVER reported. Cannot calculate corrected alpha threshold. Only significant results were published." Box 4 (purple, bottom-right): "4. PRIMARY ENDPOINT FAILURE - All 3 NASCIS trials failed their primary endpoint. Guidelines changed based on subgroup data alone." Below the grid, a wide red banner: "Classic Example: ISIS-2 (1988) showed aspirin increased mortality in Gemini/Libra patients by astrological sign subgroup - deliberately absurd to illustrate the problem." Clean icons, arrows, professional fonts
NASCIS Trials & Methylprednisolone in Acute Spinal Cord Injury
PG Orthopaedic Exam - Complete Answer with Diagrams
1. Introduction
2. The Three NASCIS Trials - Comparison Table
NASCIS I (1984, JAMA)
- 330 patients, two MPSS doses, within 48 hours, no placebo arm
- Primary outcome: NEGATIVE (no difference between doses)
- Concluded: dose was insufficient - higher dose needed
NASCIS II (1990, NEJM) ★ Most Exam-Tested
- 3 arms: high-dose MPSS vs naloxone vs placebo
- Primary outcome: NEGATIVE
- Post hoc subgroup: benefit if MPSS given within 8 hours of injury
- Protocol:
- Bolus: 30 mg/kg IV over 15 minutes
- Infusion: 5.4 mg/kg/hr for 23 hours (begin 45 min after bolus)
NASCIS III (1997, JAMA)
- 3 arms: MPSS 24h vs MPSS 48h vs Tirilazad mesylate 48h
- Primary outcome: NEGATIVE
- Post hoc: if started <3 hours → 24-hour protocol; if 3-8 hours → 48-hour protocol
- Tirilazad (lipid peroxidation inhibitor): no benefit
3. Clinical Decision Flowchart - NASCIS Protocol
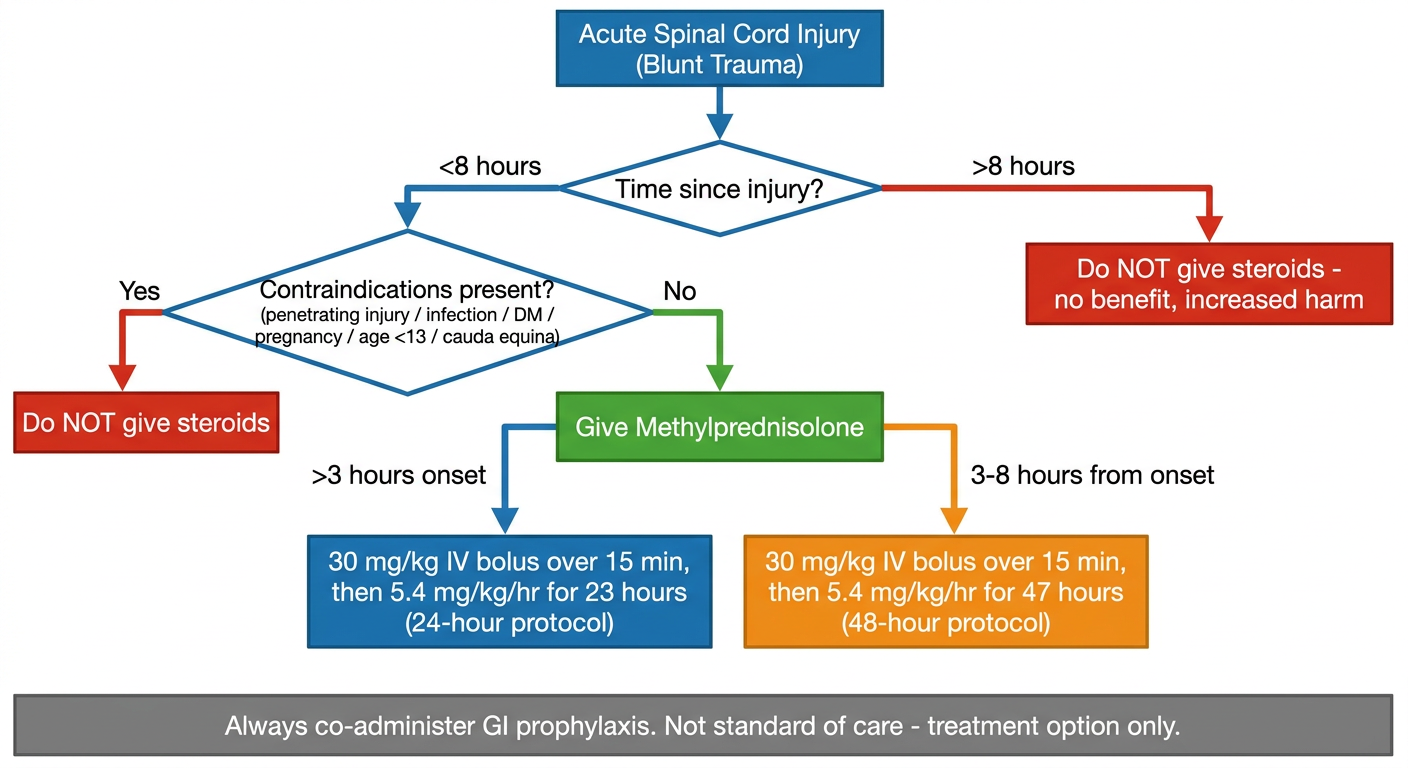
| Onset to treatment | Duration |
|---|---|
| < 3 hours | 24-hour infusion |
| 3 - 8 hours | 48-hour infusion |
| > 8 hours | Do NOT give |
4. Secondary SCI Cascade - Mechanism & Target of Methylprednisolone
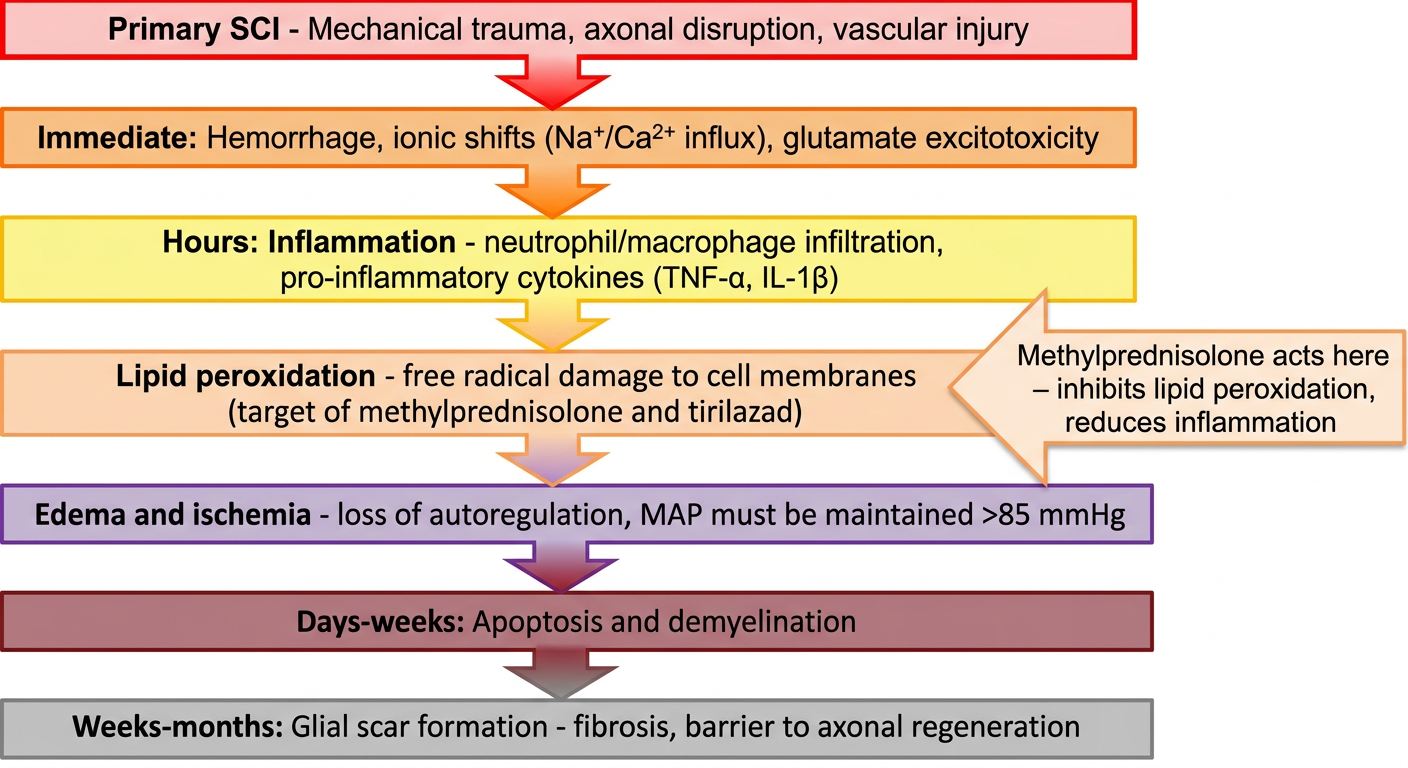
- Primary injury (mechanical) triggers an inflammatory biochemical cascade
- Secondary injury proceeds through edema, ischemia, lipid peroxidation, and apoptosis
- Methylprednisolone targets lipid peroxidation and inflammation - theoretically limiting secondary injury
- The cord also loses autoregulation - hence MAP must be maintained >85 mmHg in the ICU
5. Why the NASCIS Trials Were Criticized - Subgroup Analysis Problems
The Four Fundamental Flaws:
Classic Teaching Example: ISIS-2 Astrological Subgroup
6. Incomplete SCI Syndromes (Context for Steroid Use)
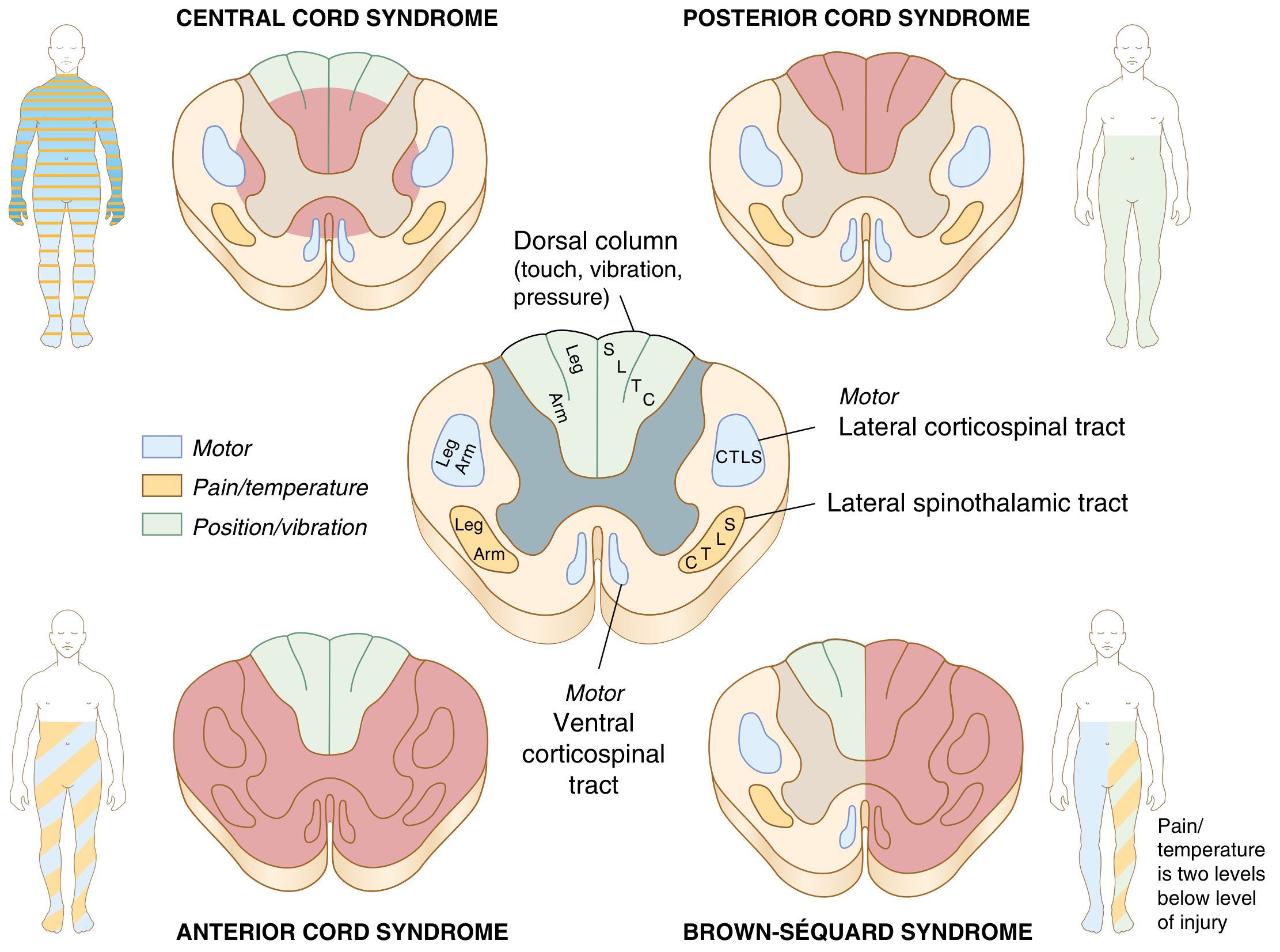
| Syndrome | Tracts affected | Clinical pattern |
|---|---|---|
| Central cord | Central gray + lateral CST | UL > LL weakness; bladder dysfunction |
| Anterior cord | Anterior 2/3 (spinothalamic + CST) | Motor loss + pain/temp loss; preserved proprioception |
| Brown-Sequard | Ipsilateral cord hemitransection | Ipsi motor + proprioception loss; contra pain/temp loss |
| Posterior cord | Dorsal columns | Proprioception + vibration loss; motor preserved |
7. Contraindications to High-Dose MPSS
- Penetrating SCI (especially gunshot wounds)
- Injury > 8 hours old
- Nerve root / cauda equina / brachial plexus injury
- Age < 13 years
- Pregnancy
- Active infection / sepsis
- Uncontrolled diabetes mellitus
8. Current Status
- High-dose MPSS is NOT standard of care
- Considered a Level III evidence treatment option at best
- Many major spine centers have discontinued its use entirely
- The turn against MPSS was driven by critical reappraisal of subgroup statistics, not by a new RCT
- If used, always co-administer GI prophylaxis (H2 blocker / PPI)
- Mean arterial pressure >85 mmHg maintenance in ICU is recommended regardless of steroid use
9. High-Yield Exam Points
| Point | Answer |
|---|---|
| NASCIS II bolus dose | 30 mg/kg IV over 15 min |
| NASCIS II infusion | 5.4 mg/kg/hr x 23 hours |
| Window for steroids | < 8 hours from injury |
| If started < 3 hr | 24-hour protocol |
| If started 3-8 hr | 48-hour protocol |
| Tested in NASCIS III vs MPSS | Tirilazad mesylate |
| Primary endpoints in all 3 NASCIS | All NEGATIVE |
| Main statistical flaw | Post hoc subgroup analysis + multiplicity |
| ISIS-2 subgroup example | Astrological sign (Gemini/Libra) |
| Is it standard of care? | No |
| Drug mechanism | Inhibits lipid peroxidation, reduces inflammation |