Normal labour
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer on normal labour. Let me compile it.
Normal Labour
Definition
Labour is a clinical diagnosis characterized by regular, painful uterine contractions that increase in frequency and intensity, accompanied by progressive cervical effacement and dilation. Uterine contractions alone, without cervical change, do not meet the criteria for labour. - Creasy & Resnik's Maternal-Fetal Medicine, p. 122
Term and Timing
- Mean duration of a human singleton pregnancy: 280 days (40 weeks) from the first day of the last normal menstrual period (LMP)
- Term = 37 to 42 weeks of gestation
- The fetoplacental unit - not the mother - is the primary controller of labour timing in humans
The Three P's: Powers, Passenger, and Passage
Labour is not a passive mechanical process. Three critical variables determine successful vaginal delivery:
| Variable | Description |
|---|---|
| Powers | Forces generated by uterine musculature (contractions) |
| Passenger | Size, attitude, lie, and presentation of the fetus |
| Passage | Size, shape, and resistance of the bony pelvis and soft tissues of the pelvic floor |
Because the fetal head and maternal pelvis are asymmetrical in shape, the fetus must execute a series of coordinated rotations - the seven cardinal movements of labour - to successfully negotiate the birth canal. - Creasy & Resnik's Maternal-Fetal Medicine, p. 137
Stages of Labour
First Stage - Cervical Effacement and Dilation
Begins with onset of labour and ends with full (10 cm) cervical dilation.
- Latent phase: irregular contractions, slow cervical change
- Active phase: regular contractions, rapid cervical dilation (typically from ~6 cm)
Second Stage - Expulsion of the Fetus
From full cervical dilation to delivery of the baby.
Third Stage - Delivery of the Placenta
From delivery of the baby to expulsion of the placenta and membranes.
Cervical Remodeling in Labour
Cervical changes begin early in pregnancy and are divided into four overlapping phases:
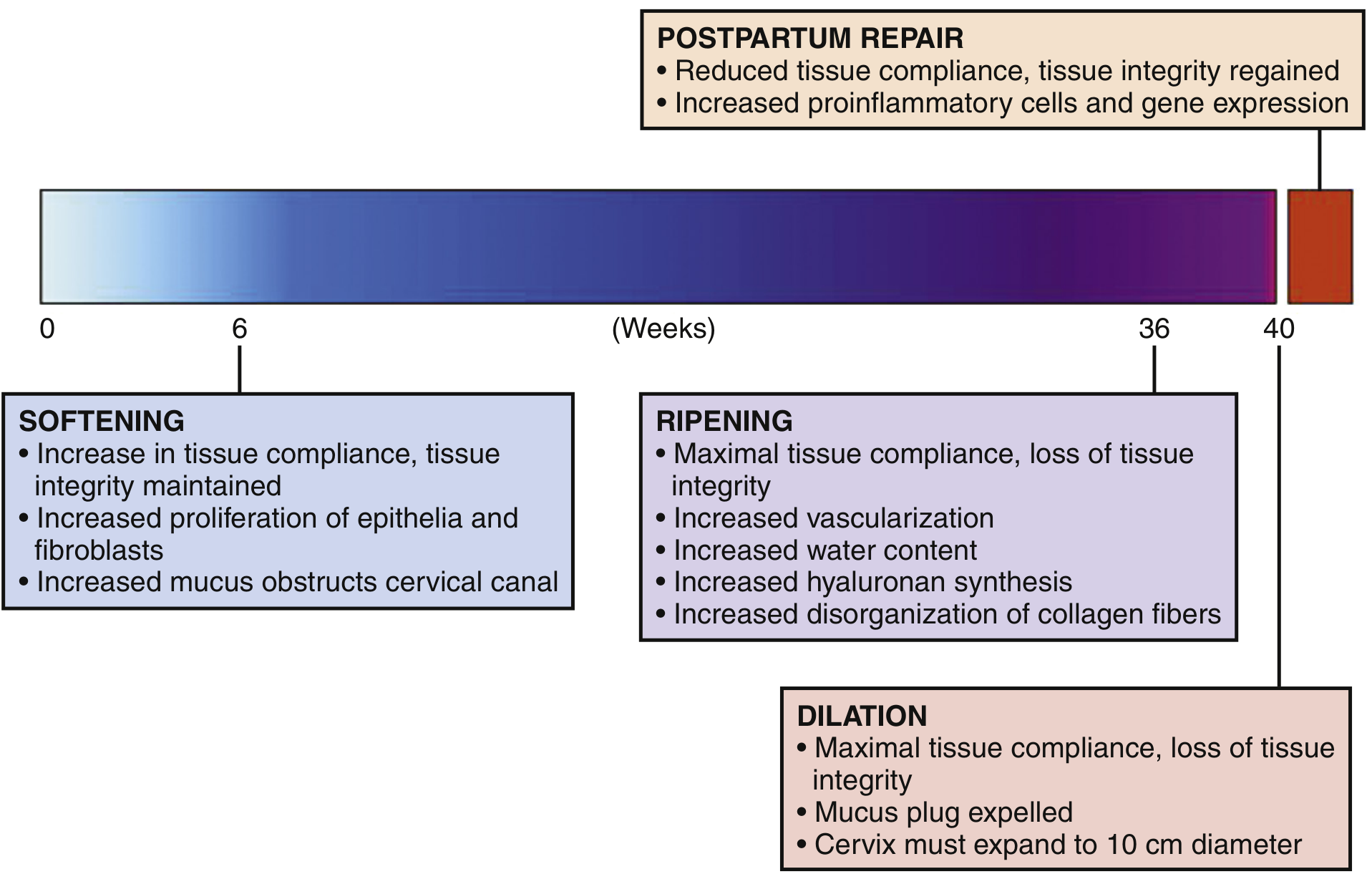
Figure: Cervical remodeling phases in human pregnancy. - Creasy & Resnik's Maternal-Fetal Medicine, Fig. 6.1
| Phase | Timing | Key Features |
|---|---|---|
| Softening | Throughout most of pregnancy (from ~6 weeks) | Increased tissue compliance; tensile strength maintained; proliferation of epithelial cells and fibroblasts; mucus obstructs cervical canal |
| Ripening | Last 1-2 weeks of gestation (~36 weeks onward) | Maximal tissue compliance; loss of tissue integrity; increased vascularization, water content, hyaluronan synthesis; disorganization of collagen fibers |
| Dilation | Active labour (~40 weeks) | Mucus plug expelled; cervix expands to 10 cm diameter |
| Postpartum Repair | After delivery | Reduced tissue compliance; tissue integrity regained; increased proinflammatory cells |
Cervical remodeling is mediated by:
- Mechanical signals from the fetal presenting part pressing against the cervix
- Endocrine/paracrine factors: progesterone, estrogen, oxytocin, and relaxin
- Biochemical changes: increased hyaluronan synthesis, local progesterone metabolism
- Traction from myometrial contractions and descent of the fetal head - Creasy & Resnik's Maternal-Fetal Medicine, p. 122-123
Hormonal Control of Labour
The hormonal cascade initiating labour involves the following key players:
Oxytocin
- Produced by the maternal posterior pituitary and by the fetus
- Acts on myometrial oxytocin receptors (OTR), whose expression increases markedly at term
- Stimulates prostaglandin synthesis in the decidua
- Upregulates gap junction formation between myocytes (connexin-43), facilitating coordinated contractions
Prostaglandins (PGE2 and PGF2α)
- Produced in the decidua, fetal membranes, and myometrium
- PGF2α acts as a uterotonic; PGE2 acts as both a cervical ripening agent and uterotonic
- Stimulate increases in intracellular calcium in myocytes
Progesterone
- Maintains uterine quiescence throughout pregnancy via progesterone receptors (PR-A and PR-B)
- A functional progesterone withdrawal occurs at term in humans - not a fall in circulating levels, but a shift in PR isoform ratio (PR-A dominance over PR-B) and local metabolism of progesterone in the cervix and myometrium
- This removes the inhibitory effect, allowing the onset of labour
Estrogen
- Promotes expression of contraction-associated proteins (CAPs) including gap junctions (connexin-43), oxytocin receptors, and prostaglandin receptors
- Counters the quiescent effects of progesterone
CRH (Corticotropin-Releasing Hormone)
- Unlike in other mammals, CRH in humans is produced by the placenta (not just the hypothalamus)
- Circulating CRH rises exponentially in late pregnancy
- Stimulates fetal HPA axis, prostaglandin production, and promotes labour onset
- Creasy & Resnik's Maternal-Fetal Medicine, p. 123-130
Myometrial Contraction Mechanism
Myometrial contraction follows the actin-myosin cross-bridge model:
- Rise in intracellular calcium (from extracellular influx and sarcoplasmic reticulum release)
- Calcium binds calmodulin (CaM)
- Calcium-CaM complex activates myosin light-chain kinase (MLCK)
- MLCK phosphorylates the 20-kDa myosin light chain
- Phosphorylated myosin binds actin, forming cross-bridges
- ATP hydrolysis causes the "power stroke" - myosin heads slide along actin filaments, shortening the cell
- Repeated asynchronous cross-bridge cycles generate continuous smooth force
Gap junctions (connexin-43) between myocytes allow synchronized electrical coupling across the uterus, coordinating contractions. - Creasy & Resnik's Maternal-Fetal Medicine, p. 130-135
Inflammatory Mechanisms in Labour
Labour at term involves a sterile physiologic inflammatory process:
- Recruitment of maternal immune cells (neutrophils, macrophages) into myometrium, cervix, and fetal membranes
- Pro-inflammatory cytokines (IL-1β, IL-6, IL-8, TNF-α) upregulate prostaglandin synthesis and matrix metalloproteinases (MMPs)
- MMPs degrade cervical extracellular matrix collagen, facilitating ripening
- This "inflammatory activation" is a normal, necessary component of term parturition and mirrors infection-induced preterm labour - but at term, it is controlled and timely
Seven Cardinal Movements of Labour
These are the sequential rotations and movements the fetal head makes to navigate the maternal pelvis:
- Engagement - fetal head enters the pelvic inlet (biparietal diameter below pelvic inlet)
- Descent - progressive downward movement throughout labour
- Flexion - head flexes so the chin meets the chest (presenting the smallest diameter)
- Internal rotation - occiput rotates anteriorly from transverse to OA (occiput anterior) position
- Extension - as head passes under the pubic symphysis, it extends (crowning and delivery of head)
- Restitution/External rotation - head rotates back to align with fetal shoulders
- Expulsion - delivery of anterior shoulder, then posterior shoulder, then rest of body
Labour Monitoring
The primary goal of labour monitoring is to achieve delivery of a healthy infant from a healthy mother with as little trauma as possible. Key elements:
- Continuous electronic fetal monitoring (CTG/EFM)
- Assessment of contraction frequency, duration, and strength
- Cervical examination for dilation, effacement, station, and membrane status
- Maternal vital signs and hydration
- Fetal heart rate patterns
- Ambulation and positions of comfort are physiologically beneficial
- Family presence reduces anxiety, may shorten labour duration, and reduces need for medications
- A 1:1 nurse-patient ratio during active labour is ideal - Creasy & Resnik's Maternal-Fetal Medicine, p. 969
Key Points Summary
| Feature | Normal Value |
|---|---|
| Gestational age at term | 37-42 weeks |
| Full cervical dilation | 10 cm |
| Cardinal movements | 7 |
| Primary hormones | Oxytocin, PGE2, PGF2α, CRH, Estrogen |
| Myocyte calcium mediator | Calmodulin / MLCK |
| Gap junction protein | Connexin-43 |
| Cervical remodeling phases | Softening → Ripening → Dilation → Postpartum Repair |
This is a shared conversation. Sign in to Orris to start your own chat.