Various modes of ventilator and weaning protocol full details for md exams 15marks answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete MD exam answer.
Modes of Mechanical Ventilation and Weaning Protocol
INTRODUCTION
Mechanical ventilation (MV) controls the same basic respiratory variables as spontaneous negative-pressure breathing: respiratory rate, tidal volume (VT), inspiratory flow rate, PEEP (positive end-expiratory pressure), and FiO₂. The mode determines the balance of control between the clinician/ventilator and the patient.
Four basic parameters are set in any ventilator mode:
- Size of breath — tidal volume (volume control) or inspiratory pressure (pressure control)
- Frequency — set respiratory rate or patient-triggered
- PEEP — baseline positive pressure maintained in the circuit
- FiO₂ — fraction of inspired oxygen
CLASSIFICATION OF VENTILATOR MODES
A. CONTROLLED MANDATORY VENTILATION (CMV)
All breaths are machine-initiated at a set rate and volume/pressure. The patient has no input. Used in deeply sedated/paralyzed patients. Rarely used alone today.
B. ASSIST CONTROL VENTILATION (AC / CMV with assist)
Definition: The clinician sets a minimum RR, VT (or driving pressure), PEEP, FiO₂, and inspiratory flow rate. Every patient-triggered effort receives a full machine breath at the preset parameters.
Two subtypes:
1. AC – Volume Control (AC-VC) — Most common initial mode
| Set (Independent) | Monitored (Dependent) |
|---|---|
| V | Peak & plateau airway pressure, minute ventilation (V |
- Guarantees minimum V
Tand minute ventilation → ensures CO₂ clearance - Plateau pressure (measured via inspiratory hold with zero flow) reflects alveolar pressure; keep ≤30 cmH₂O (lung-protective)
- Peak pressure = dynamic airway pressure (flow × resistance) + alveolar pressure; elevated peak with normal plateau → ↑ airway resistance (kinked tube, bronchospasm, auto-PEEP)
- Disadvantage: High plateau pressures → barotrauma; dyspneic patients may have flow starvation → patient-ventilator dyssynchrony and increased work of breathing
2. AC – Pressure Control (AC-PC / PCV)
| Set | Monitored |
|---|---|
| Inspiratory driving pressure, RR, PEEP, FiO₂ | Tidal volume, V |
- A set driving pressure is applied above PEEP each breath; inspiration ends when flow decreases below a threshold (~20% peak flow)
- V
Tvaries depending on lung compliance → must monitor closely; no guaranteed minute ventilation - Useful when limiting peak pressures (ARDS, post-thoracic surgery with fresh suture lines)
- Important hazard: Spontaneously breathing patients generate negative intrathoracic pressure; net transalveolar pressure = set driving pressure + patient's negative effort → can produce larger V
Tthan expected → volume trauma despite apparently normal ventilator pressures
C. PRESSURE-REGULATED VOLUME CONTROL (PRVC)
A hybrid "dual-control" mode using advanced microprocessor technology.
- Clinician sets a target V
T(like volume control) but the ventilator delivers the lowest pressure necessary to achieve it (like pressure control) - Senses patient inspiratory effort and allows variable inspiratory flow → better patient comfort and ventilator synchrony than classic AC-VC
- V
Tcan vary breath-to-breath (ventilator adaptation is not instantaneous) - Caution in ARDS: Strong patient efforts can generate V
Texceeding the set target → risk of volume trauma; must monitor closely
D. PRESSURE SUPPORT VENTILATION (PSV)
Definition: Entirely patient-triggered; no mandatory breaths. Clinician sets inspiratory support pressure, PEEP, and FiO₂.
| Set | Monitored |
|---|---|
| Inspiratory pressure, PEEP, FiO₂ | V |
Mechanism: Patient's inspiratory effort triggers the ventilator → pressure is raised to the set level → maintained until flow falls below ~20% of peak → expiration begins.
- V
Tdetermined by lung compliance + patient effort; not guaranteed - RR, V
T, and VEmust be monitored closely → risk of apnea and hypoventilation - Uses: Transitioning off MV (primary weaning mode), ventilation for airway support in less-sedated patients, analogous to BiPAP machine
- Gradually decrease PSV during weaning by 2–3 cmH₂O steps targeting V
T4–6 mL/kg, RR <30 breaths/min
E. SYNCHRONIZED INTERMITTENT MANDATORY VENTILATION (SIMV)
Definition: Hybrid of AC and PSV. Mandatory breaths at set rate + synchronized with patient effort; spontaneous breaths above rate receive only set pressure support (not a full machine breath).
| SIMV vs AC |
|---|
| AC: every patient-triggered breath → full V |
| SIMV: spontaneous breaths above set rate → patient-generated V |
- If rate is set high + patient deeply sedated → essentially equivalent to volume control
- If rate set low → essentially equivalent to PSV with minimal mandatory sigh breaths
- Weaning with SIMV: Progressively decrease mandatory rate by 1–2 breaths/min; when IMV rate reaches 2–4 breaths/min with acceptable ABGs and RR <30, discontinue MV
F. CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP)
- Constant positive pressure maintained throughout respiratory cycle (both inspiration and expiration)
- Patient breathes entirely spontaneously — no pressure support
- Recruits collapsed alveoli, reduces work of breathing, improves oxygenation
- Used as part of SBT (spontaneous breathing trial) and weaning
- Non-invasive CPAP via mask for obstructive sleep apnea, mild-moderate respiratory failure
G. NONINVASIVE POSITIVE PRESSURE VENTILATION (NIV / BiPAP)
- Delivered via nasal or full-face mask at two pressure levels:
- IPAP (inspiratory positive airway pressure) → assists inhalation
- EPAP (expiratory positive airway pressure) → equivalent to PEEP
- Key indications:
- COPD exacerbation with hypercapnia (pH 7.25–7.35) → reduces intubation need, shortens hospital stay; pH <7.2 → usually requires intubation
- Acute cardiogenic pulmonary edema (diuresis + vasodilators rapidly improve mechanics)
- Chronic respiratory failure (severe scoliosis, neuromuscular disease, COPD with chronic hypercapnia)
- Contraindications: inability to protect airway, high aspiration risk, inability to clear secretions, facial trauma, hemodynamic instability, upper airway obstruction
H. ADVANCED MODES
1. Airway Pressure Release Ventilation (APRV) / Bilevel Ventilation
- Two levels of CPAP: P
Highfor a longer time (THigh) + PLowfor a shorter time (TLow) - Allows spontaneous breathing at both pressure levels → minimizes sedation requirement
- P
Highensures oxygenation; PLow/TLowensures ventilation without derecruitment - Best for ARDS with severely reduced compliance and large chest wall
- Recent meta-analysis (~19 years of data) showed mortality benefit of APRV vs. conventional modes in acute hypoxemic respiratory failure
2. High-Frequency Oscillatory Ventilation (HFOV)
- Extremely low V
T(1–3 mL/kg) at very high frequency (3–15 Hz) - Theoretical appeal in ARDS (ultralow barotrauma/volutrauma)
- Clinical trials have not shown benefit in adults; may have a role in pediatric ARDS
- Used as salvage therapy or bridge to ECMO in refractory ARDS
3. ECMO (Extracorporeal Membrane Oxygenation)
- For entirely refractory hypoxemia unresponsive to all ventilator strategies
- VV-ECMO (venovenous): isolated lung pathology
- VA-ECMO (venoarterial): combined cardiac + lung dysfunction
MODES SUMMARY TABLE
| Mode | Set by Clinician | Monitored | Best Use |
|---|---|---|---|
| AC-VC | V | Plateau pressure, V | Deeply sedated/paralyzed, ARDS (lung-protective) |
| AC-PC | Driving pressure, RR, PEEP, FiO₂ | V | High peak pressures, post-thoracic surgery |
| PRVC | V | Pressure, V | Patients with variable effort needing V |
| PSV | Inspiratory pressure, PEEP, FiO₂ | V | Weaning, alert spontaneously breathing patients |
| SIMV | V | Spontaneous V | Weaning transition |
| CPAP | CPAP level | RR, V | Weaning SBT, OSA, mild hypoxemia |
| APRV | P | V | Severe ARDS |
| HFOV | Mean airway pressure, amplitude, frequency | V | Refractory ARDS (pediatric/salvage) |
WEANING FROM MECHANICAL VENTILATION
Concept
The term "weaning" implies gradual withdrawal — but evidence shows this approach unnecessarily prolongs MV by up to 40%. Current practice emphasizes active daily liberation assessment rather than passive gradual weaning.
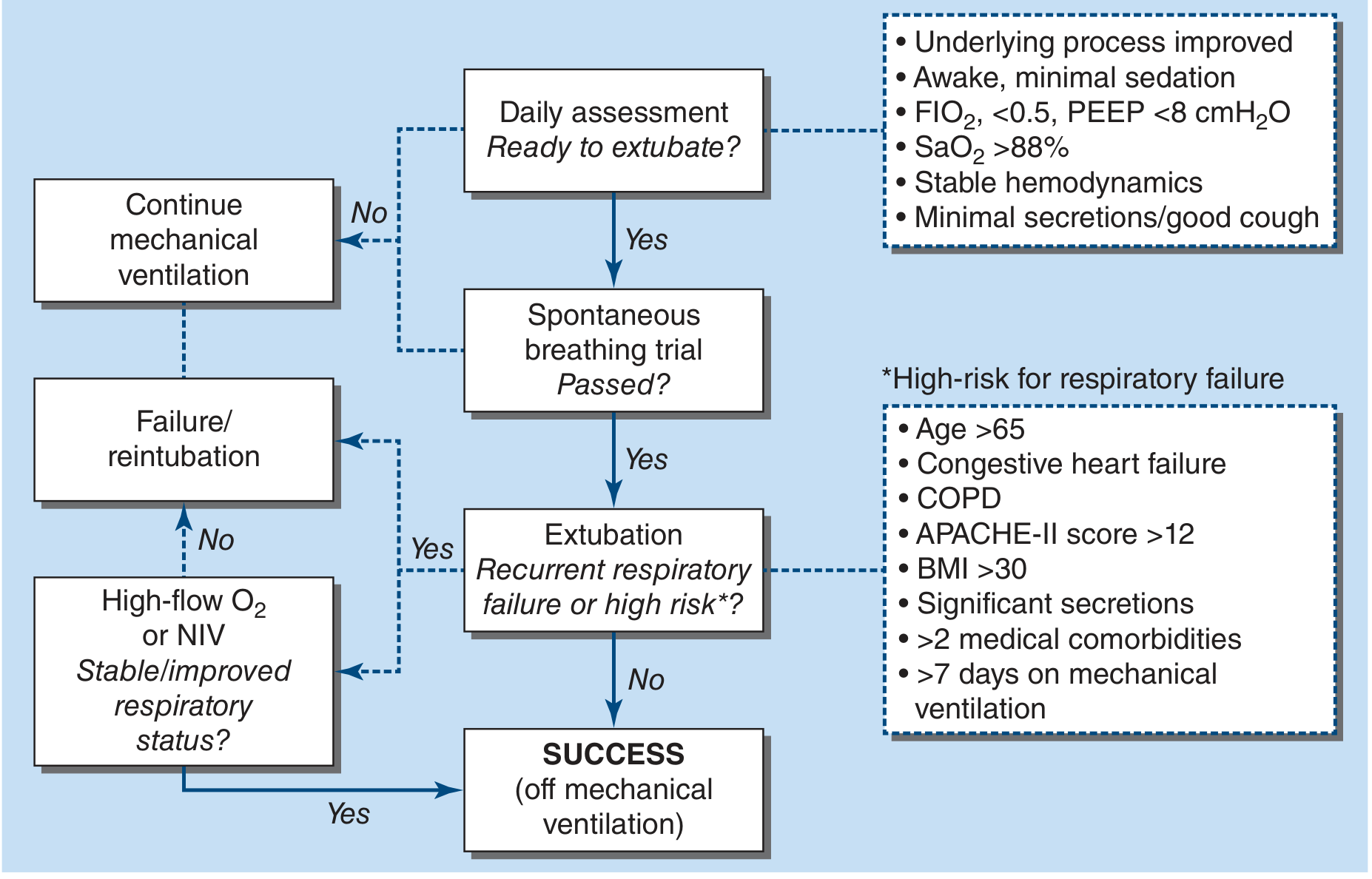
Step 1: Daily Assessment of Readiness to Extubate
Screen every day for all of the following criteria:
| Criterion | Target |
|---|---|
| Underlying disease process | Improved/resolving |
| Sedation level | Awake, minimal or no sedation |
| FiO₂ | ≤ 0.5 (50%) |
| PEEP | < 8 cmH₂O |
| SaO₂ | > 88% |
| Hemodynamics | Stable (no vasopressor requirement or minimal) |
| Secretions | Manageable; adequate cough |
| Airway reflexes | Intact |
Step 2: Spontaneous Breathing Trial (SBT)
If readiness criteria are met → perform SBT immediately.
Method:
- Reduce ventilator support to minimal (pressure support 5–7 cmH₂O, PEEP 5 cmH₂O) to compensate for ETT resistance only
- Duration: 30–120 minutes
- Alternatively: T-piece trial (no positive pressure support)
SBT Pass Criteria (all must be met):
| Parameter | Threshold |
|---|---|
| Respiratory rate | < 35 breaths/min |
| SaO₂ | > 90% |
| Systolic BP | 90–180 mmHg |
| Heart rate change | Stable; < 20% change |
| Patient comfort | No marked anxiety, agitation, or dyspnoea |
Outcome: Patients passing SBT have >70% chance of successful extubation.
Weaning Indices (Physiologic Parameters)
| Index | Measurement | Favourable Threshold |
|---|---|---|
| RSBI (Tobin Index) | f (breaths/min) / V | < 100–105 → likely to wean successfully; > 120 → continue support |
| Negative Inspiratory Force (NIF) | Max. inspiratory pressure | ≤ −25 to −30 cmH₂O |
| Tidal Volume | Spontaneous V | > 5 mL/kg |
| Vital Capacity | Measured at bedside | > 10–15 mL/kg |
| Minute Ventilation | Required minute ventilation | < 10 L/min |
| PaO₂/FiO₂ ratio | ABG-derived | ≥ 150–200 mmHg |
Important: Over-reliance on these indices versus SBT outcome delays extubation unnecessarily. SBT remains the gold standard.
Weaning Techniques (When Gradual Weaning Is Needed)
1. SIMV Weaning
- Decrease mandatory rate by 1–2 breaths/min as tolerated
- Monitor ABGs and RR at each step (minimum 15–30 min)
- Target: RR < 30, PaCO₂ < 45–50 mmHg (or pH > 7.35)
- Discontinue MV when rate reaches 2–4 breaths/min with acceptable ABGs
2. PSV Weaning (Preferred method)
- Decrease pressure support by 2–3 cmH₂O stepwise
- Monitor V
T(target 4–6 mL/kg), RR (< 30), ABGs - Extubate when PS = 5–8 cmH₂O (tube compensation level) with acceptable parameters
3. T-piece Trials / CPAP Sprints
- Patient breathes through T-piece (no ventilator support) or low-level CPAP
- Duration progressively increased over hours/days
- Assess for respiratory distress, haemodynamic changes, and desaturation
Evidence: Daily SBT protocols reduce ventilator days by 25% and ICU length of stay by 10% compared to traditional gradual weaning.
Step 3: Extubation
After successful SBT → assess for high-risk extubation failure factors:
| High-Risk Factors for Post-Extubation Failure |
|---|
| Age > 65 years |
| Congestive heart failure |
| COPD |
| APACHE-II score > 12 |
| BMI > 30 |
| Significant secretions |
| > 2 medical comorbidities |
| > 7 days on mechanical ventilation |
For high-risk patients: Transition immediately post-extubation to high-flow nasal oxygen (HFNO) or NIV → significantly reduces reintubation rates.
Weaning Algorithm (Harrison's 22E)
COMPLICATIONS OF MECHANICAL VENTILATION
| Complication | Mechanism | Prevention |
|---|---|---|
| Barotrauma (pneumothorax, pneumomediastinum) | High plateau pressure | Keep plateau ≤30 cmH₂O |
| Volutrauma | Large V | Low V |
| Atelectrauma | Cyclical alveolar collapse/reopening | Adequate PEEP |
| Ventilator-associated pneumonia (VAP) | Biofilm on ETT, microaspiration | Head elevation, oral decontamination, early weaning |
| Patient-ventilator dyssynchrony | Flow starvation, trigger failure, breath stacking | Mode adjustment, sedation |
| Haemodynamic compromise | ↑ intrathoracic pressure → ↓ venous return | Minimize PEEP, ensure euvolaemia |
| GI stress ulcers | Splanchnic ischaemia | PPI/H₂ blocker prophylaxis |
| ICU-acquired weakness | Prolonged sedation/NMB, critical illness | Daily sedation holidays, early mobilization |
KEY POINTS FOR MD EXAM
- AC-VC is the most common initial mode; guarantees V
Tand minute ventilation but requires monitoring of plateau pressure (keep ≤30 cmH₂O) - PSV is the preferred weaning mode; every breath is patient-triggered
- SIMV is a hybrid; useful for gradual weaning by reducing mandatory rate
- RSBI = f/V
T(L); <100–105 predicts successful extubation - SBT duration: 30–120 minutes; >70% success rate predicts extubation
- SBT-based daily liberation protocols reduce ventilator days by 25%
- Post-extubation NIV or HFNO in high-risk patients reduces reintubation
- In ARDS: lung-protective strategy = V
T6 mL/kg IBW, plateau ≤30 cmH₂O, PEEP titrated to lower inflection point - Approaching MV removal as a "wean" (vs. active liberation) extends unnecessary MV by up to 40%
Sources: Harrison's Principles of Internal Medicine 22E (2025); Sabiston Textbook of Surgery; Morgan & Mikhail's Clinical Anesthesiology 7E; Rosen's Emergency Medicine; Miller's Anesthesia 10E
This is a shared conversation. Sign in to Orris to start your own chat.