24 year male with 4 day fever with rash. Differential diagnosis and approach to management
Reading File
search_medical_text
fever with rash differential diagnosis young adult
search_medical_text
fever rash management workup approach investigations
search_medical_image
fever rash differential diagnosis approach
GradeResponse
GradeResponse
GradeResponse
Here is a structured clinical approach to a 24-year-old male with 4 days of fever and rash:
1. History — Critical First Step
(Harrison's, p. 649)
Gather the following before anything else:
| Domain | Key Questions |
|---|---|
| Rash characterization | Site of onset, direction/rate of spread, evolution (macular → papular → vesicular → petechial?) |
| Associated symptoms | Cough, coryza, conjunctivitis, lymphadenopathy, arthralgia, headache, myalgia, sore throat |
| Epidemiology | Travel history (tropical regions), animal/arthropod bites, sexual history, sick contacts |
| Immune/med status | Immunizations, recent medications (within 1 month), HIV status, prosthetic material |
| Dietary exposures | Unpasteurized dairy, undercooked meat |
2. Rash Morphology — Narrows the Differential
| Rash Type | Key Differentials |
|---|---|
| Maculopapular (centrifugal) | Measles, Rubella, EBV (mono), Drug reaction, Secondary syphilis, Typhoid (rose spots) |
| Maculopapular (centripetal — trunk first) | Roseola (HHV-6), Rubella |
| Petechial / Purpuric | Meningococcemia ⚠️, RMSF ⚠️, Dengue, ITP, Vasculitis |
| Vesicular / Bullous | Varicella, Herpes zoster, HSV, Hand-Foot-Mouth (enterovirus) |
| Diffuse erythematous + desquamation | Scarlet fever (S. pyogenes), Toxic shock syndrome (TSS) ⚠️ |
| Target lesions | Erythema multiforme, Lyme disease (early disseminated) |
| Eschar | Rickettsial disease, Scrub typhus |
3. Differential Diagnosis — Organized by Likelihood
🔴 Can't-Miss / Life-Threatening (Rule Out First)
| Condition | Distinguishing Features |
|---|---|
| Meningococcemia | Petechial/purpuric non-blanching rash, starts on extremities, rapidly progressing, septic shock, meningism |
| Rocky Mountain Spotted Fever (RMSF) | Tick exposure, rash starts on wrists/ankles → spreads centrally, thrombocytopenia, elevated transaminases |
| Toxic Shock Syndrome | Diffuse macular erythroderma, hypotension, multiorgan failure; staph or strep focus |
| Dengue hemorrhagic fever | Thrombocytopenia, plasma leakage, warning signs (abdominal pain, vomiting, mucosal bleeding) |
| Secondary syphilis with systemic involvement | Sexual history, involvement of palms/soles, painless |
🟡 Common Infectious Causes
| Condition | Distinguishing Features |
|---|---|
| Dengue fever | Tropical travel, retro-orbital pain, "breakbone" myalgia, islands of skin sparing (classic), thrombocytopenia |
| Infectious mononucleosis (EBV) | Pharyngitis, posterior cervical LAD, atypical lymphocytosis, splenomegaly; rash post-amoxicillin is characteristic |
| Measles | Prodrome of 3 Cs (cough, coryza, conjunctivitis), Koplik spots, maculopapular rash cephalocaudal spread (Harrison's, p. 6035) |
| Rubella | Milder than measles, post-auricular/suboccipital lymphadenopathy, no cough |
| Chikungunya | Travel, severe polyarthralgia, maculopapular rash |
| Typhoid fever | Relative bradycardia, rose spots (trunk), splenomegaly, travel to endemic area |
| Leptospirosis | Water exposure, conjunctival suffusion, myalgia (calf), jaundice |
| Rickettsial (Scrub typhus) | Eschar (tache noire), scrub vegetation exposure, Asia |
| Enteroviral exanthem | Summer/autumn, young adults, coxsackievirus/echovirus |
🟢 Non-Infectious
| Condition | Features |
|---|---|
| Drug hypersensitivity | New medication in past 2–4 weeks, morbilliform rash, eosinophilia |
| Stevens-Johnson Syndrome / TEN | Medication trigger, mucosal involvement (eyes, mouth, genitals), skin detachment ⚠️ |
| Adult-onset Still's disease | Quotidian salmon-colored rash (evanescent, appears with fever spikes), arthritis, hyperferritinemia |
| Vasculitis (e.g., HSP) | Palpable purpura, arthralgia, renal involvement |
4. Approach to Management
Step 1: Immediate Assessment (Triage)
- Vital signs — hypotension/tachycardia → resuscitate first
- Look for red flags: non-blanching rash, meningism, altered consciousness, mucosal involvement, signs of bleeding → admit + empiric treatment immediately
Step 2: Initial Investigations
| Investigation | What It Tells You |
|---|---|
| CBC with differential | Thrombocytopenia (dengue, RMSF, leptospira), leukopenia (viral), atypical lymphocytes (EBV), leukocytosis (bacterial) |
| Peripheral smear | Atypical lymphocytes, malaria parasites, schistocytes (TTP) |
| LFTs, RFTs, electrolytes | Hepatitis (EBV, dengue, leptospira), renal involvement |
| CRP / ESR / Procalcitonin | Bacterial vs viral trend |
| Blood cultures (×2) | Before antibiotics if bacterial cause suspected |
| Serology | Dengue NS1 Ag + IgM/IgG; Widal; Leptospira IgM; Monospot / EBV VCA IgM; VDRL; Rickettsial IgM |
| Urine R/E | Leptospirosis, vasculitis |
| Chest X-ray | Measles pneumonia, secondary infection |
| Skin biopsy | If diagnosis unclear — vasculitis, RMSF, drug reaction |
Step 3: Directed Treatment (Based on Diagnosis)
| Condition | Treatment |
|---|---|
| Meningococcemia | IV Ceftriaxone 2g q12h STAT |
| RMSF / Rickettsial | Doxycycline 100mg BD × 7–14 days (start empirically if suspected) |
| Dengue (uncomplicated) | Supportive — paracetamol, oral hydration, avoid NSAIDs/aspirin |
| Dengue hemorrhagic fever | IV fluids, close monitoring, platelet transfusion if <10,000 or active bleeding |
| Typhoid | Ceftriaxone IV or azithromycin (depending on local resistance) |
| EBV mono | Supportive, avoid contact sports (splenic rupture risk), avoid amoxicillin |
| Scarlet fever / GAS | Phenoxymethylpenicillin or amoxicillin × 10 days |
| TSS | Source control + flucloxacillin/vancomycin + IVIg in severe cases |
| Drug reaction | Stop offending drug, antihistamines; systemic steroids for severe reactions |
| SJS/TEN | Stop drug, admit to burns unit, ophthalmology, dermatology |
5. A Classic Example — Dengue Fever Rash
(Relevant in a young male with 4-day fever, especially with travel history)
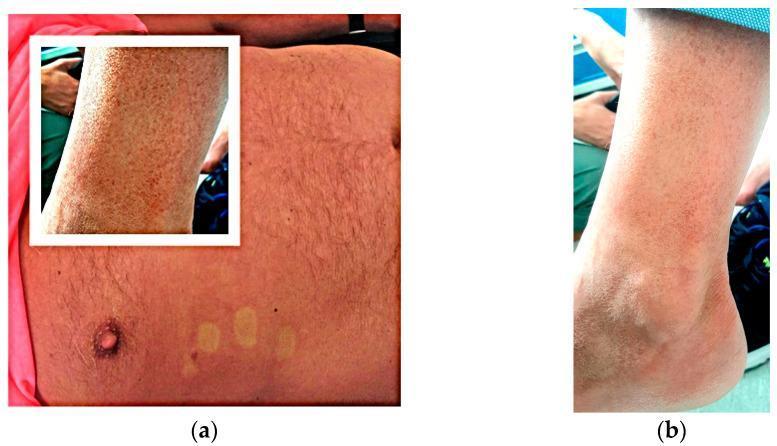
Panel (a): Macular erythematous rash with characteristic "islands of skin sparing" on trunk. Panel (b): Purpuric/petechial lesions on lower extremity suggesting thrombocytopenia.
Summary Algorithm
Fever + Rash (4 days)
│
├── Non-blanching / petechial? → Rule out Meningococcemia / RMSF IMMEDIATELY
│
├── Mucosal involvement? → Rule out SJS/TEN
│
├── Travel history?
│ ├── Tropical → Dengue, Chikungunya, Typhoid, Malaria + rash
│ └── Animal/tick bite → RMSF, Lyme, Rickettsial
│
├── Pharyngitis + LAD → EBV / Strep (Scarlet fever)
│
├── Drug history → Drug reaction / DRESS
│
└── Quotidian rash + arthritis + high ferritin → Still's disease
Clinical Pearl: In any patient with fever + non-blanching rash, do NOT delay empiric Ceftriaxone and Doxycycline while awaiting workup — the cost of under-treating RMSF or meningococcemia is death.
Thermoregulation
Reading File
search_medical_text
thermoregulation physiology hypothalamus body temperature control
search_medical_text
heat loss mechanisms sweating vasoconstriction fever pathophysiology pyrogens
search_medical_image
thermoregulation hypothalamus temperature regulation diagram
GradeResponse
GradeResponse
GradeResponse
Thermoregulation
1. Overview
The human body maintains a core temperature of 36.5–37.5°C (97.7–99.5°F) in a neutral environment, despite continuous metabolic heat production and variable environmental temperatures. This is achieved through a tightly regulated balance between heat production and heat loss, orchestrated primarily by the hypothalamus (Harrison's, p. 635).
2. The Thermoregulatory Center
Hypothalamic Control
The preoptic anterior hypothalamus (POA) is the primary integration hub. It receives two streams of input (Harrison's, p. 635):
- Peripheral signals — from thermoreceptors in the skin via peripheral nerves
- Central signals — from the temperature of blood directly bathing hypothalamic neurons
These signals are integrated and compared against an internal set point. Deviations trigger corrective effector responses.
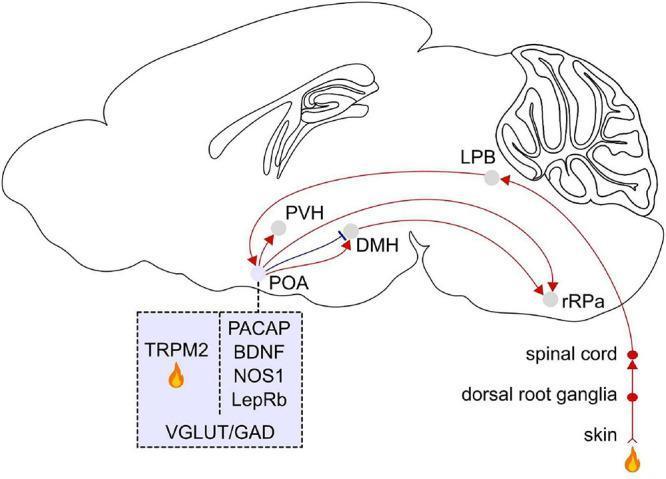
Afferent and efferent neural pathways of thermoregulation centered on the preoptic area (POA) of the hypothalamus.
Key Neural Pathways
| Pathway | Route |
|---|---|
| Afferent (peripheral → central) | Skin thermoreceptors → Dorsal root ganglia → Spinal cord → Lateral parabrachial nucleus (LPB, pons) → POA |
| Efferent (central → effectors) | POA → Paraventricular hypothalamus (PVH) → Dorsomedial hypothalamus (DMH) → Rostral Raphe Pallidus (rRPa) → sympathetic/somatic effectors |
Molecular Sensors in the POA
Warm-sensitive POA neurons express: PACAP, BDNF, NOS1, LepRb, and the local heat sensor TRPM2 (a thermosensitive ion channel). These neurons use both glutamatergic (VGLUT) and GABAergic (GAD) signaling.
3. Peripheral Thermoreceptors
| Receptor Type | Location | Fiber | Responds to |
|---|---|---|---|
| Warm receptors | Skin, viscera | C fibers (unmyelinated) | Temp 30–45°C; peak ~38°C |
| Cold receptors | Skin (superficial) | Aδ fibers (thinly myelinated) | Temp 10–35°C; peak ~25°C |
| Central thermoreceptors | Hypothalamus, spinal cord, brainstem | — | Core blood temperature |
Cold receptors outnumber warm receptors in the skin (~3–10:1), making humans more sensitive to cold.
4. Heat Production Mechanisms
The body generates heat through:
| Mechanism | Details |
|---|---|
| Basal metabolic rate (BMR) | Ongoing cellular metabolism — primary source at rest |
| Shivering thermogenesis | Involuntary skeletal muscle contractions; can increase heat production 4–5× |
| Non-shivering thermogenesis (NST) | Brown adipose tissue (BAT) — uncoupling protein-1 (UCP-1) uncouples oxidative phosphorylation, generating heat instead of ATP; important in neonates and cold-acclimatized adults |
| Voluntary muscle activity | Exercise increases heat production up to 10–20× basal |
| Specific dynamic action of food | Especially protein digestion increases metabolic rate |
5. Heat Loss Mechanisms
Four physical mechanisms govern heat dissipation from the body surface:
| Mechanism | Description | % of Heat Loss (at rest) |
|---|---|---|
| Radiation | Infrared electromagnetic waves emitted from skin surface to surrounding environment | ~60% |
| Evaporation | Sweating + insensible perspiration; obligatory at high environmental temperatures when radiation/convection fail | ~25% |
| Conduction | Direct transfer via contact with solid objects (e.g., cool surface) | ~3% |
| Convection | Heat carried away by air/water moving over skin surface | ~12% |
Evaporation becomes the dominant heat loss mechanism when ambient temperature exceeds body temperature — radiation and convection reverse direction.
6. Effector Responses — The Feedback Loop
Response to Cold (Core Temp ↓ below set point)
- Cutaneous vasoconstriction — reduces blood flow to skin, conserves core heat
- Piloerection — traps insulating air (vestigial in humans)
- Shivering — generates heat via muscle contractions
- Non-shivering thermogenesis — BAT activation via sympathetic norepinephrine → UCP-1
- Behavioral — seeking warmth, huddling, adding clothing
Response to Heat (Core Temp ↑ above set point)
- Cutaneous vasodilation — increases blood flow to skin; heat transferred from core to surface
- Sweating — eccrine sweat glands (cholinergic sympathetic); evaporation cools skin
- Decreased metabolic rate (mild)
- Behavioral — seeking shade, removing clothing, reduced activity
7. Fever — A Regulated Rise in the Set Point
Fever is not a failure of thermoregulation — it is a purposeful upward resetting of the hypothalamic set point (Harrison's, p. 637).
Mechanism of Fever
Exogenous pyrogens (LPS, viral proteins, toxins)
↓
Macrophages/monocytes activated
↓
Endogenous pyrogens released:
IL-1β, IL-6, TNF-α, IFN-γ
↓
Circumventricular organs (organum vasculosum of lamina terminalis — OVLT)
(lack blood-brain barrier)
↓
Phospholipase A2 → Arachidonic acid → COX-2 → PGE2
↓
PGE2 acts on EP3 receptors in POA
↓
Set point ↑ → body temperature perceived as "too cold"
↓
Vasoconstriction + Shivering → Temperature rises to new set point
Maintaining and Defervescing Fever (Harrison's, p. 637)
- Maintenance: Once blood temperature matches the new (higher) set point, the hypothalamus maintains it via the same heat-balance mechanisms used in the afebrile state.
- Defervescence: When pyrogen concentration falls (resolution of infection) or antipyretics are given (COX inhibition → ↓PGE2), the set point resets downward → vasodilation + sweating dissipates heat → "breaking the fever."
Fever vs. Hyperthermia — A Critical Distinction
| Feature | Fever | Hyperthermia |
|---|---|---|
| Set point | Elevated | Normal |
| Mechanism | Pyrogen → PGE2 → hypothalamic reset | Heat gain exceeds heat dissipation capacity |
| Examples | Infection, autoimmune, malignancy | Heat stroke, malignant hyperthermia, NMS |
| Response to antipyretics | Yes | No |
| Risk | Beneficial (up to ~41°C); harmful above | Medical emergency at any degree |
8. Temperature Measurement — Clinical Points
| Site | Normal Range | Notes |
|---|---|---|
| Oral | 36.5–37.5°C | Standard; avoid after hot/cold food |
| Rectal | ~0.4°C higher than oral | Most accurate core measurement |
| Axillary | ~0.5°C lower than oral | Least reliable |
| Tympanic | Approximates core | Operator-dependent accuracy |
Fever is defined as a core temperature >38.3°C (101°F) in adults (Harrison's).
9. Clinical Disorders of Thermoregulation
| Disorder | Mechanism | Key Features |
|---|---|---|
| Heat exhaustion | Volume/salt depletion from sweating | Temp <40°C, weakness, nausea, intact CNS |
| Heat stroke | Thermoregulatory failure; set point overwhelmed | Temp >40°C, anhidrosis, altered consciousness — emergency |
| Hypothermia | Heat loss > heat production | Core <35°C; cardiac arrhythmias below 30°C |
| Malignant hyperthermia | Ryanodine receptor mutation (RYR1); triggered by halogenated anesthetics/succinylcholine | Extreme hyperthermia, rigidity, rhabdomyolysis |
| Neuroleptic malignant syndrome (NMS) | Dopamine D2 receptor blockade | Hyperthermia, rigidity, autonomic instability, altered consciousness |
| Fever of unknown origin (FUO) | Persistent pyrexia >38.3°C for >3 weeks, cause unknown after 1 week investigation | Infections, malignancy, autoimmune most common |
Summary
TEMPERATURE STIMULUS
│
├── Cold detected
│ → Vasoconstriction → Shivering → NST (BAT/UCP-1)
│
└── Heat detected
→ Vasodilation → Sweating → Behavioral changes
POA (Hypothalamus) = Master thermostat
Set point controlled by PGE2 (fever) and normal neural signals
Heat balance = Heat production ↔ Heat loss (Radiation + Evaporation + Conduction + Convection)
The elegance of thermoregulation lies in its dual-sensing architecture — central blood temperature monitoring combined with peripheral skin receptor input — allowing the hypothalamus to anticipate thermal challenges before core temperature actually changes.
This is a shared conversation. Sign in to Orris to start your own chat.