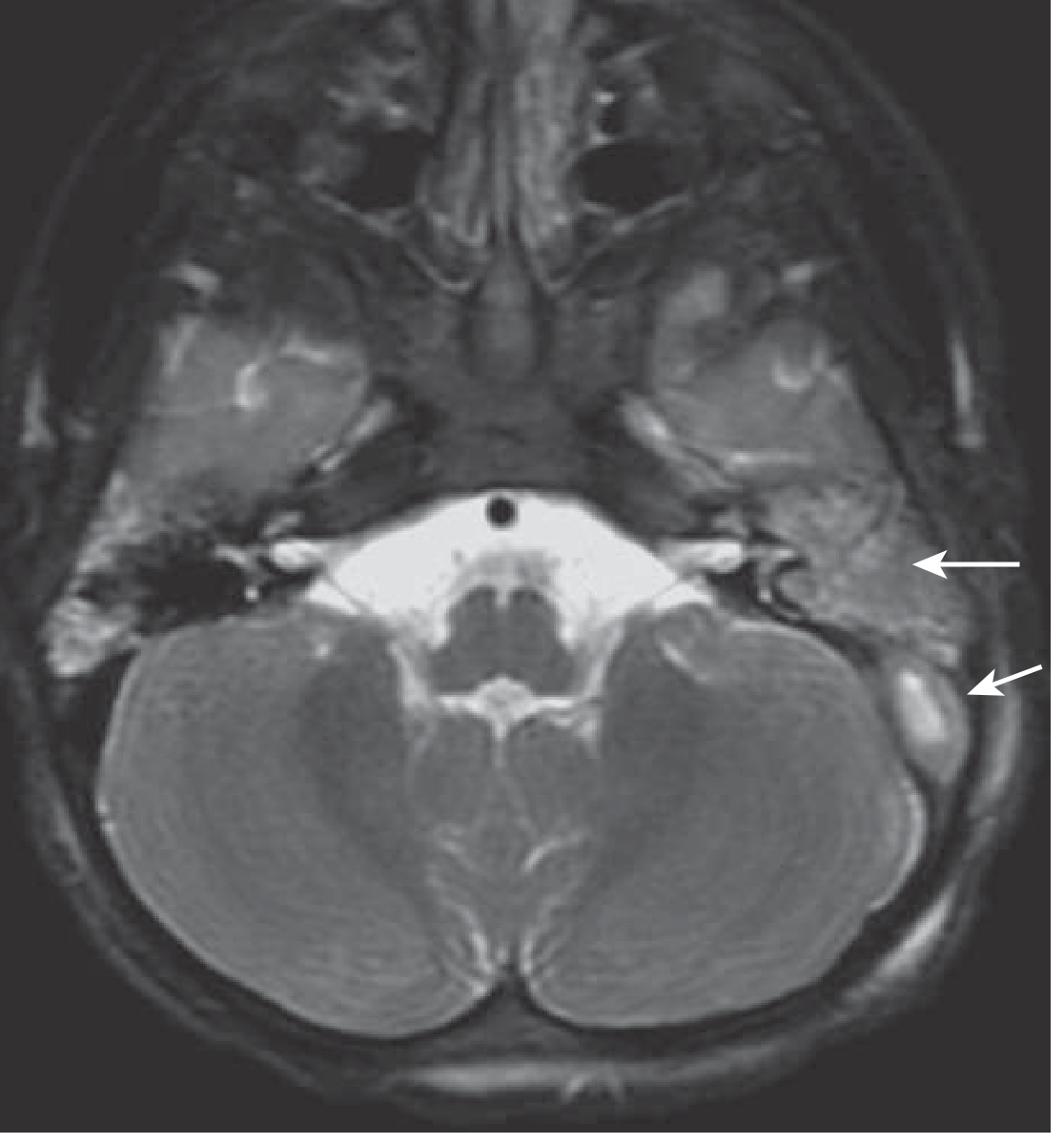
Mri study shows Sluggish flow in left transverse sinus and left sigmoid sinus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cerebral venous sinus thrombosis" AND "transverse sinus" AND MRI
Reading File
Finding Sources
Searching PubMed
"cerebral venous thrombosis" AND "MRI" AND "diagnosis"
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough interpretation of this MRI finding:
Sluggish Flow in Left Transverse and Sigmoid Sinuses - MRI Interpretation
What This Finding Means
"Sluggish flow" in the left transverse and sigmoid sinuses is an ambiguous MRI descriptor that can represent three distinct entities, which must be distinguished from each other:
| Possibility | Significance | Action |
|---|---|---|
| Normal variant / Hypoplastic sinus | Benign, no treatment needed | Correlate with anatomy |
| Slow flow (non-thrombotic) | Benign artifact or reduced flow | Gadolinium-enhanced MRV to confirm patency |
| Cerebral Venous Sinus Thrombosis (CVST) | Serious - requires anticoagulation | Full workup urgently |
Anatomy Review
The transverse sinuses extend laterally from the torcular Herophili (where superior sagittal, straight, and occipital sinuses converge) and drain into the sigmoid sinuses, which then empty into the internal jugular veins. Importantly, one transverse sinus is frequently hypoplastic - most commonly the left - as right-sided dominance is the norm. A hypoplastic sinus may show reduced or absent flow signal on MRV and can easily be misread as thrombosis.
"Often, one hypoplastic transverse sinus can cause confusion if a sinus thrombosis is suspected. In these cases, the jugular notch in the occipital bone and jugular foramen may be smaller on the side of the hypoplastic transverse sinus."
- Goldman-Cecil Medicine
Why Slow Flow Can Mimic Thrombosis on MRI
On 2D Time-of-Flight (TOF) MR venography (the most common technique used):
- Normal venous sinuses appear as bright/hyperintense flow signal
- Absent or reduced flow = loss of that signal, which looks like thrombosis
- But: slow/sluggish flow also causes loss of the TOF signal, creating a "flow gap" artifact
Ayanzen et al. (2000) found flow gaps in 31% of patients with entirely normal MRI findings - and these gaps occurred almost exclusively in the nondominant (90%) or codominant (10%) transverse sinuses, i.e., exactly where this patient's finding is located. Flow gaps were NOT found in the dominant transverse sinus or superior sagittal/straight sinuses - so those locations carry higher suspicion for true thrombosis.
"Variations in the speed of blood flow and anatomical variants of the venous sinuses may change their usual signal characteristics, leading to a false diagnosis of venous sinus thrombosis. Slow flow in a venous sinus may cause increased signal on T1- and T2-weighted images, potentially leading to a false assumption of thrombosis."
- Bradley & Daroff's Neurology in Clinical Practice
How to Differentiate: What to Look For
On conventional MRI sequences:
- In true thrombosis: loss of normal T1/T2 flow void + signal intensity changes in the sinus itself (iso- then hyperintense as clot ages, especially on T1 when methemoglobin forms)
- In slow flow/hypoplasia: T1 and T2 images usually show no thrombus signal within the sinus lumen
On MR venography (MRV):
- Absent or severely reduced flow signal in the affected sinus
- In thrombosis: often accompanied by engorged cortical draining veins "upstream"
- In hypoplasia: contralateral sinus is dominant, ipsilateral jugular foramen/notch may be smaller
Gadolinium-enhanced imaging (the key differentiator):
- Slow flow / hypoplasia: gadolinium fills the sinus, confirming patency
- True thrombosis: "empty delta sign" / no contrast filling within the lumen; only peripheral/dural wall enhancement around the clot
- Phase-contrast MRV can also detect very slow flow that TOF misses
Susceptibility-weighted imaging (SWI):
- Thrombosed sinuses appear expanded and exaggeratedly hypointense ("blooming")
- Prominent serpiginous veins in the drainage territory indicate venous congestion
Red Flags for True CVST
If any of the following are present, CVST must be actively excluded:
- Headache (especially new, progressive, or thunderclap)
- Papilledema / raised ICP symptoms (visual changes, pulsatile tinnitus)
- Seizures, focal neurological deficits, or encephalopathy
- Left temporal/parietal parenchymal abnormality on the same MRI (edema, FLAIR signal, hemorrhagic venous infarct - characteristically in the posterolateral temporal lobe / inferior parietal lobule for lateral sinus involvement)
- Risk factors: oral contraceptive use, pregnancy/puerperium, thrombophilia, dehydration, mastoiditis/otitis media (septic lateral sinus thrombosis), malignancy, Behcet disease
Causes of True Left Transverse/Sigmoid Sinus Thrombosis
| Category | Examples |
|---|---|
| Procoagulant states | OCP, pregnancy, protein C/S deficiency, antiphospholipid syndrome, factor V Leiden |
| Local infection | Otitis media/mastoiditis (septic lateral sinus thrombosis - look for mastoid signal on same MRI) |
| Trauma | Adjacent skull fracture |
| Inflammatory | Behcet disease, vasculitis |
| Malignancy | Direct invasion or hypercoagulable state |
| Idiopathic | ~25% of cases |
Recommended Workup
- Gadolinium-enhanced MRI/MRV - most important next step; demonstrates whether contrast fills the sinus (rules out thrombosis) or shows empty delta sign (confirms thrombosis)
- CT venography (CTV) - excellent alternative; optimal for major dural sinus thrombosis; shows the delta sign (intraluminal clot surrounded by contrast)
- SWI sequence - if not already done; very sensitive for sinus thrombosis
- Compare sinus size bilaterally - if left transverse is hypoplastic by anatomy (smaller jugular foramen, nondominant side), this likely represents a benign variant
- If CVST confirmed: thrombophilia screen, mastoid assessment, coagulation studies
Clinical Bottom Line
Sluggish flow in the left transverse and sigmoid sinuses most commonly represents a normal left-sided hypoplastic/nondominant sinus - a well-documented pitfall in MRV interpretation. However, CVST cannot be excluded on this finding alone. The next step is gadolinium-enhanced MRI/MRV (or CT venography) to confirm sinus patency and correlate with clinical symptoms. If the patient is symptomatic (headache, raised ICP, focal deficits), treat as CVST until proven otherwise.
Sources: Bradley & Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology
What will be the final diagnosis?
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
The clinical picture is now complete and the diagnosis is clear. Here is the full answer:
Final Diagnosis: Cerebral Venous Sinus Thrombosis (CVST) - Left Lateral Sinus
The Diagnostic Triad Is Complete
The three findings together establish CVST with near certainty:
| Finding | Significance |
|---|---|
| Sluggish / absent flow - left transverse & sigmoid sinuses | Thrombotic occlusion of the left lateral sinus |
| Hemorrhagic venous infarct | Venous outflow obstruction → venous hypertension → parenchymal edema → hemorrhagic transformation (characteristically in the posterolateral temporal lobe / inferior parietal lobule - the drainage territory of the lateral sinus and vein of Labbé) |
| Seizures | Cortical irritation from the hemorrhagic infarct in the adjacent cortex |
"CVT should be suspected in patients presenting with stroke symptoms without risk factors, unexplained new seizures or refractory headaches, or signs of intracranial hypertension."
- Rosen's Emergency Medicine
Why This Is No Longer a Diagnostic Dilemma
Earlier, "sluggish flow alone" could represent a hypoplastic/nondominant sinus (a benign variant). However:
- A hypoplastic sinus does not cause hemorrhagic infarction - it is a structural absence with no outflow obstruction
- A slow flow artifact does not cause parenchymal injury
- Only true thrombosis with venous hypertension causes the downstream parenchymal damage seen here
"If anticoagulation is not implemented early, the reduction in parenchymal venous drainage leads to venous hypertension and subsequent infarction, which is frequently haemorrhagic."
- Grainger & Allison's Diagnostic Radiology
Pathophysiology
Thrombus in left transverse + sigmoid sinus
↓
Obstruction of venous outflow
↓
Venous hypertension in left posterolateral hemisphere
↓
Interstitial edema (vasogenic, then cytotoxic)
↓
Hemorrhagic venous infarct (left temporal/parietal cortex)
↓
Cortical irritation → Seizures
Next Steps
- Gadolinium-enhanced MRI + MRV - still needed to confirm extent and rule out additional sinus involvement (superior sagittal sinus, straight sinus)
- CT venography - excellent alternative; shows the "empty delta sign" (intraluminal clot surrounded by contrast) and defines extent
- SWI sequence - shows "blooming" in the thrombosed sinus and identifies all hemorrhagic foci
- Urgent anticoagulation - LMWH preferred over UFH; even in the presence of hemorrhagic infarction, anticoagulation is still indicated (evidence shows it does not worsen hemorrhage and prevents clot propagation)
- Seizure management - antiepileptic drug (e.g., levetiracetam)
- Thrombophilia workup - antiphospholipid antibodies, protein C/S, factor V Leiden, prothrombin gene mutation
- Look for precipitant - oral contraceptive use? mastoiditis (check mastoid signal on the same MRI)? pregnancy/puerperium? malignancy?
Summary
Final Diagnosis: Left-sided Cerebral Venous Sinus Thrombosis (CVST) involving the left transverse and sigmoid sinuses, complicated by hemorrhagic venous infarction and seizures.
This is a neurological emergency. MRI + MRV with gadolinium (or CT venography) should be performed urgently to confirm, map the full extent, and guide anticoagulation therapy.
Sources: Rosen's Emergency Medicine; Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine; Bradley & Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.