Is body edema seen in mitral stenosis and regurgitation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Body Edema in Mitral Stenosis and Mitral Regurgitation
The short answer: Yes, body (peripheral) edema can occur in both, but the mechanism and timing differ. It is a late feature driven by right ventricular (RV) failure in both conditions.
Mitral Stenosis (MS)
Mechanism:
- The stenotic mitral valve obstructs left ventricular filling → left atrial pressure rises → pulmonary venous pressure rises.
- This leads first to pulmonary edema (early/moderate disease).
- Chronically elevated pulmonary pressures cause pulmonary arterial hypertension → RV pressure overload.
- As disease progresses, right ventricular failure develops → systemic venous congestion.
- Systemic venous congestion manifests as ascites and peripheral (body) edema - a late-stage finding.
From Goldman-Cecil Medicine:
"As the disease progresses and right ventricular failure occurs, ascites and edema are common. Neck vein elevation, ascites, and edema are present if right ventricular failure has developed."
So the order of edema in MS is:
- Early: Pulmonary edema (left-sided congestion)
- Late: Peripheral/body edema + ascites (right-sided failure)
Additional point: About 50% of pregnant women with severe MS experience pulmonary edema during pregnancy due to increased blood volume and cardiac output.
Mitral Regurgitation (MR)
Mechanism - Chronic MR:
- Regurgitant flow into the left atrium → LA and LV volume overload → LV dilates.
- Progressive LV dysfunction → elevated left atrial and pulmonary venous pressures → pulmonary edema.
- With sustained pulmonary hypertension → RV failure → peripheral edema.
From Symptom to Diagnosis (4th Ed.):
"Patients with mitral regurgitation may be identified during an evaluation of shortness of breath, dyspnea on exertion, edema, orthopnea, and fatigue."
Complications of MR explicitly listed include:
- Dyspnea, 2. Pulmonary edema, 3. Atrial fibrillation, 4. Sudden death
Mechanism - Acute severe MR:
- Sudden volume overload → acute pulmonary edema (often the presenting emergency). Patients are typically sitting upright in frank pulmonary edema.
Key Distinction: Type of Edema
| Feature | Mitral Stenosis | Mitral Regurgitation |
|---|---|---|
| Pulmonary edema | Yes - classic, early feature | Yes - especially acute severe MR |
| Peripheral/body edema | Yes - late, from RV failure | Yes - late, from LV then RV failure |
| Ascites | Yes - with advanced RV failure | Yes - with advanced RV failure |
| Mechanism | LA obstruction → pulmonary HTN → RV failure | Volume overload → LV failure → pulmonary HTN → RV failure |
Summary
- Pulmonary edema is characteristic of both conditions (more acute/dramatic in MR; common in MS).
- Peripheral/body edema occurs in both, but represents late-stage disease with RV failure and systemic venous congestion.
- In MS, body edema is specifically driven by the sequence: mitral obstruction → pulmonary hypertension → RV pressure overload → RV failure.
- In MR, body edema results from: volume overload → LV dysfunction → pulmonary hypertension → RV failure.
- When peripheral edema is present in MS, you also typically find neck vein distention, ascites, and hepatomegaly - all signs of right heart failure.
Sources: Goldman-Cecil Medicine (International Ed.), Braunwald's Heart Disease (11th Ed.), Symptom to Diagnosis (4th Ed.), Miller's Anesthesia (10th Ed.)
What is colicky pain
Finding Sources
Reading File
Reading File
Excellent content. Here is the complete answer:
Colicky Pain
Definition: Colicky pain (colic) is a type of pain characterized by sudden onset, reaching a peak rapidly, then passing off - only to return in waves. It is caused by forceful, spasmodic contractions of smooth muscle in the wall of a hollow viscus (tube or organ) that is trying to overcome an obstruction or expel its contents.
The word comes from the Greek kolon (large intestine), but colic now refers to the pain pattern, not just gut pain.
Common Features of All Colics
From S. Das - Manual on Clinical Surgery:
- (a) Sudden appearance of gripping pain which stays for a period, during which the patient almost tosses on the bed, then passes off as suddenly as it came
- (b) Nausea, vomiting, belching, retching
- (c) Varying degree of collapse
- (d) Absence of true muscle guarding (though voluntary abdominal wall contraction may mimic it)
Associated symptoms: sweating, vomiting, and clammy extremities are very common.
Why It Is Wavey (Pathophysiology)
The hollow viscus (ureter, bile duct, intestine) contracts forcefully against an obstruction (stone, stricture, fecalith). Smooth muscle has a cyclical contraction-relaxation pattern:
- Contraction phase = intense, gripping pain
- Relaxation phase = pain subsides or disappears
- This repeats, giving the classic "wave" pattern
The key: the organ wall has smooth muscle that contracts rhythmically - when this is against a resistance, the patient feels waves of severe pain.
Types of Colicky Pain
| Type | Cause | Location | Radiation | Key Features |
|---|---|---|---|---|
| Biliary colic | Gallstone obstructing cystic/common bile duct | Right hypochondrium | Right scapular angle, right shoulder | Triggered by fatty food; nausea/vomiting; may have jaundice |
| Ureteric (renal) colic | Stone in the ureter | Loin/flank | Groin, testis, inner thigh (L1-L2) | Hematuria; testis may be drawn up; profuse sweating; most severe colic |
| Intestinal colic | Small bowel obstruction, enteritis | Periumbilical/central abdomen | - | Relieved by passing flatus; distension; visible peristalsis in thin patients |
| Appendicular colic | Obstructive appendicitis | Right iliac fossa | - | Vomiting + fever; serious - risk of gangrene |
| Lead colic | Lead poisoning | Diffuse abdomen | - | Painter/battery worker history; blue line on gums; severe constipation |
Important Note: "Biliary Colic" Is a Misnomer
Despite being called a colic, biliary pain is often steady rather than truly colicky (intermittent waves). The common bile duct has very little smooth muscle in its wall, which is why the pain does not have the classic gripping-releasing wave pattern seen in ureteric colic. Ureteric colic is the most classic, severe example of true colicky pain.
How Colicky Pain Differs from Other Pain Types
| Feature | Colicky Pain | Peritonitic Pain | Ischemic Pain |
|---|---|---|---|
| Character | Wavey, gripping, comes and goes | Constant, worsened by movement | Constant, severe |
| Patient behavior | Writhes, cannot stay still | Lies perfectly still | Variable |
| Muscle guarding | Absent (between waves) | Present (rigid abdomen) | Variable |
| Cause | Smooth muscle spasm vs. obstruction | Peritoneal inflammation | Vascular compromise |
Key teaching point: The patient with colic cannot stay still - they roll around, pace, toss on the bed. This contrasts sharply with peritonitis, where any movement worsens the pain and the patient lies completely still.
Sources: S. Das Manual on Clinical Surgery (13th Ed.), Brenner and Rector's The Kidney (2-Vol Set), Tintinalli's Emergency Medicine, Bailey and Love's Short Practice of Surgery (28th Ed.)
Renal filteration physiology for usmle
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a complete, USMLE-focused answer. Here it is:
Renal Filtration Physiology - USMLE High-Yield Review
1. Overview
Glomerular filtration is the first step in urine formation. Blood enters the glomerular capillaries via the afferent arteriole, a fraction is filtered into Bowman's space, and the remainder exits via the efferent arteriole. The filtered fluid (ultrafiltrate) contains water and all small solutes, but no proteins or blood cells.
- GFR (normal): ~125 mL/min (180 L/day filtered, ~1.5 L excreted)
- Renal Plasma Flow (RPF): ~625 mL/min
- Filtration Fraction (FF) = GFR/RPF = 125/625 = 20%
2. The Glomerular Filtration Barrier (3 Layers)
| Layer | Structure | Function |
|---|---|---|
| Endothelium | Fenestrated pores 70-100 nm | Prevents blood cells from passing; allows proteins |
| Glomerular Basement Membrane (GBM) | Lamina rara interna + lamina densa + lamina rara externa | Main barrier - negatively charged, blocks large proteins (especially albumin) |
| Podocytes (Epithelium) | Foot processes with filtration slits (25-60 nm) | Secondary size/charge barrier |
USMLE pearl: In minimal change disease, podocyte foot processes are effaced (flattened) on EM - GBM looks normal on light microscopy but proteins leak through. This is the most common cause of nephrotic syndrome in children.
Two determinants of filterability:
- Molecular size - molecules <4 nm pass freely; >8 nm are excluded
- Electrical charge - negative GBM repels negatively charged proteins (albumin); loss of negative charge = proteinuria
3. Starling Forces - The GFR Equation
$$\text{GFR} = K_f \times \text{Net Filtration Pressure}$$
$$\text{Net Filtration Pressure} = (P_G - P_B) - (\pi_G - \pi_B)$$
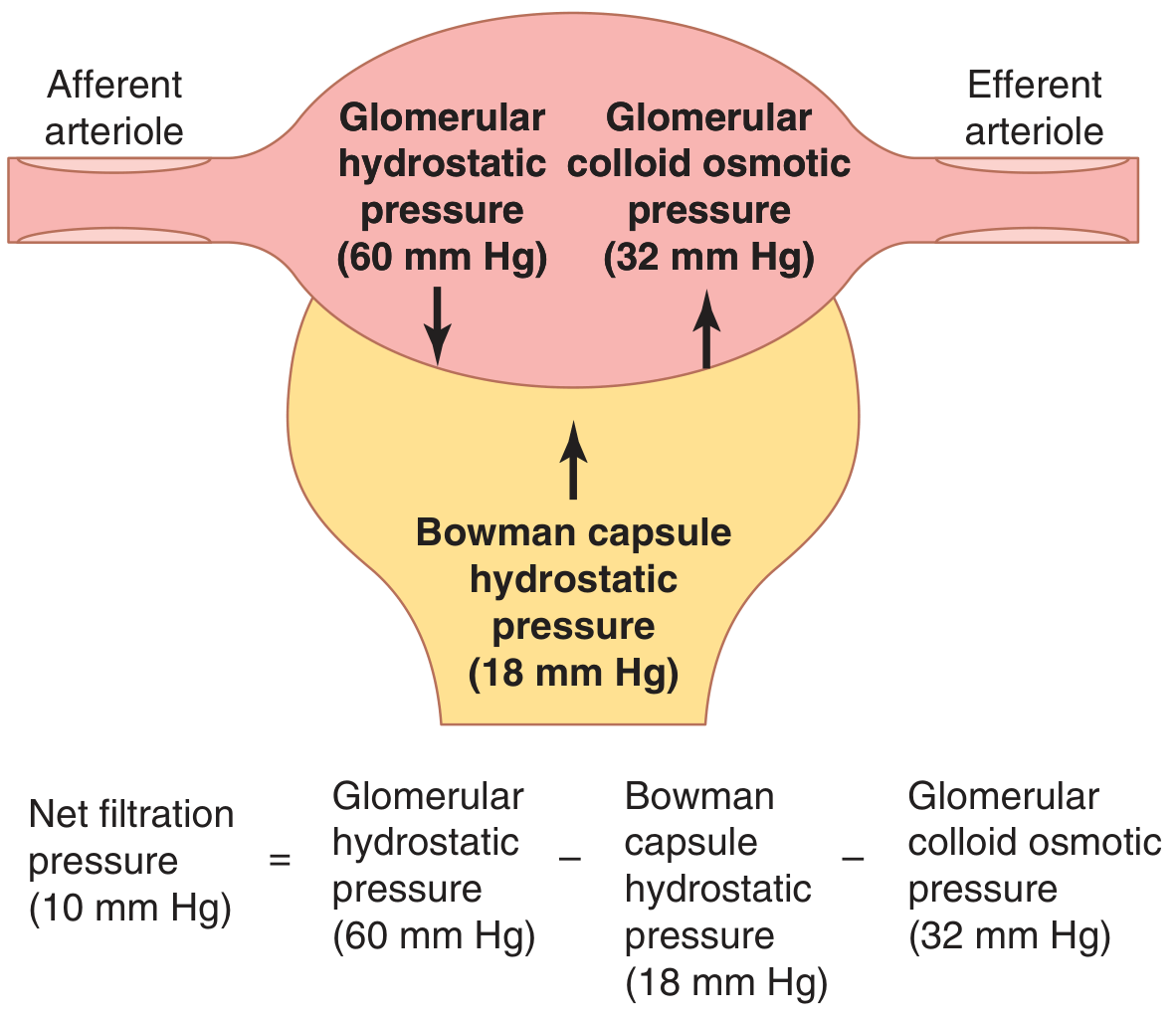
| Force | Value | Direction | Notes |
|---|---|---|---|
| P_G - Glomerular hydrostatic pressure | 60 mmHg | Favors filtration | Main driving force |
| P_B - Bowman capsule hydrostatic pressure | 18 mmHg | Opposes filtration | Rises with ureteral obstruction |
| π_G - Glomerular capillary oncotic pressure | 32 mmHg | Opposes filtration | Rises along capillary as fluid is filtered out |
| π_B - Bowman capsule oncotic pressure | ~0 mmHg | Favors filtration | Normally negligible (no protein in filtrate) |
Net filtration pressure = 60 - 18 - 32 = +10 mmHg
K_f (filtration coefficient) = permeability × surface area. Normal ~12.5 mL/min/mmHg. Reduced in diabetes, HTN, aging.
Filtration Equilibrium
As blood travels along the glomerular capillary, protein is left behind as fluid filters out. This raises π_G progressively until net filtration pressure = 0. This point of filtration equilibrium normally occurs at the end of the glomerular capillary.
4. Arteriolar Control of GFR - The Most-Tested Concept
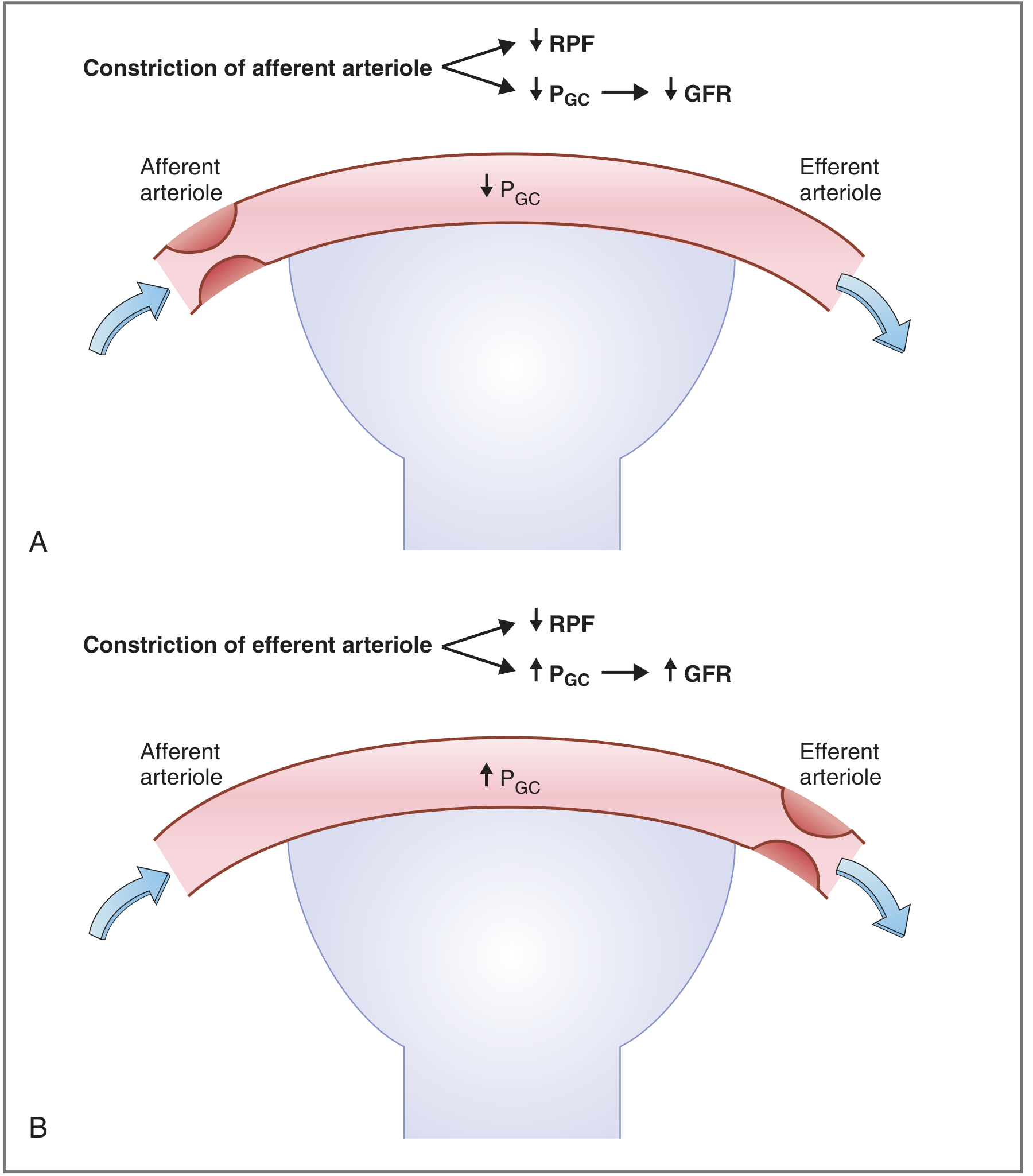
| Manipulation | RPF | GFR | Filtration Fraction | Mechanism |
|---|---|---|---|---|
| Afferent constriction | ↓ | ↓ | No change | Less blood enters glomerulus → ↓P_G → ↓GFR |
| Efferent constriction | ↓ | ↑ | ↑ | Blood dams up in glomerulus → ↑P_G → ↑GFR |
| Afferent dilation | ↑ | ↑ | No change | More blood enters → ↑P_G |
| Efferent dilation | ↑ | ↓ | ↓ | Blood escapes easily → ↓P_G |
Key rule: Afferent and efferent constriction both reduce RPF, but have opposite effects on GFR.
5. Angiotensin II - High-Yield Drug Target
Angiotensin II preferentially constricts the efferent arteriole (more than the afferent).
- Low Ang II: Efferent constriction dominant → ↓RPF, ↑GFR, ↑FF
- High Ang II (e.g., hemorrhage): Constricts both; GFR is partially "protected" due to efferent preference
ACE inhibitors / ARBs:
- Block Ang II → dilate efferent arteriole → ↓P_G → ↓GFR, ↑RPF, ↓FF
- Used in diabetic nephropathy to reduce glomerular hyperfiltration and proteinuria
- Contraindicated in bilateral renal artery stenosis - removing efferent tone causes acute GFR crash
NSAIDs:
- Block prostaglandins → constrict afferent arteriole → ↓GFR
- Dangerous in volume-depleted patients who rely on prostaglandins to maintain afferent tone
6. Other Factors That Change GFR
| Factor | Effect on GFR | Mechanism |
|---|---|---|
| ↓Plasma protein (nephrotic, liver failure) | ↑GFR | ↓π_G → ↑net filtration pressure |
| ↑Plasma protein (dehydration, hyperproteinemia) | ↓GFR | ↑π_G → ↓net filtration pressure |
| Ureteral obstruction (stone) | ↓GFR | ↑P_B → opposes filtration |
| Renal disease / diabetes / HTN | ↓GFR | ↓K_f (thickened GBM, loss of capillaries) |
| High-protein diet | ↑GFR | ↑proximal Na reabsorption → ↓macula densa NaCl → TGF → afferent dilation |
7. Autoregulation of GFR (MAP 80-180 mmHg)
GFR stays relatively constant despite changes in blood pressure via two mechanisms:
A. Myogenic mechanism (fast)
- ↑BP → stretches afferent arteriole wall → Ca²+ channels open → smooth muscle contracts → ↑resistance → maintains constant flow
B. Tubuloglomerular Feedback (TGF) - via Juxtaglomerular Apparatus
- ↑GFR → ↑NaCl delivery to macula densa → macula densa releases adenosine/ATP → afferent arteriole constricts → ↓GFR back toward normal
- ↓GFR → ↓NaCl at macula densa → afferent arteriole dilates + renin released → ↑GFR
JGA components: Macula densa (distal tubule cells) + Juxtaglomerular cells (afferent/efferent arteriole wall) + Extraglomerular mesangial cells
8. Measuring GFR - Clearance Concept
$$\text{Clearance} = \frac{U \times \dot{V}}{P}$$
where U = urine concentration, V̇ = urine flow rate, P = plasma concentration
Gold standard: Inulin clearance
- Freely filtered, not reabsorbed or secreted - clearance exactly equals GFR
- Not used clinically (must be infused)
Clinical substitute: Creatinine clearance (~GFR)
- Slightly overestimates GFR because creatinine is secreted by proximal tubules
- Estimated by Cockcroft-Gault or CKD-EPI formulas
PAH clearance = Renal Plasma Flow (RPF)
- PAH is freely filtered AND secreted → essentially all PAH is cleared in one pass
- Clearance of PAH ≈ RPF (~625 mL/min)
9. Quick Summary Table for USMLE Vignettes
| Clinical Scenario | What happens to GFR |
|---|---|
| ACE inhibitor given | ↓GFR (efferent dilation) |
| NSAID in dehydrated patient | ↓GFR (afferent constriction) |
| Bilateral renal artery stenosis + ACE-I | Acute ↓↓GFR (remove efferent tone) |
| Renal artery stenosis (one side) | Contralateral kidney compensates |
| Heart failure (low BP) | ↓GFR (↓P_G) - Ang II partially preserves it |
| Nephrotic syndrome | Acute ↑GFR (↓π_G), chronic ↓GFR (K_f loss) |
| Ureteral stone | ↓GFR (↑P_B) |
| Sepsis/shock | ↓GFR (afferent vasoconstriction by catecholamines) |
Sources: Guyton & Hall Textbook of Medical Physiology (14th Ed.), Costanzo Physiology (7th Ed.), Comprehensive Clinical Nephrology (7th Ed.), Harrison's Principles of Internal Medicine (22nd Ed., 2025)
This is a shared conversation. Sign in to Orris to start your own chat.