Essay answer on direct laryngoscope with points
Reading File
Finding Sources
Searching the Web
direct laryngoscopy anatomy technique complications clinical anesthesia
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, well-sourced content. Let me compile the full essay answer.
Direct Laryngoscopy - Essay Answer
1. Definition
Direct laryngoscopy (DL) is a technique that allows direct visualization of the larynx - specifically the glottis and vocal cords - using a handheld instrument called a laryngoscope, without any mirrors or intermediate optical systems. It is the most commonly used technique for orotracheal intubation in clinical practice.
"The most commonly used technique for tracheal intubation is DL, which involves direct visualization of the glottis with the assistance of a laryngoscope. The ETT is inserted through the glottic opening into the trachea under continuous observation."
- Miller's Anesthesia, 10e
2. Indications
A. Airway Management / Intubation
- Securing the airway under general anesthesia
- Rapid Sequence Intubation (RSI) in emergencies
- Cardiopulmonary resuscitation (CPR / cardiac arrest)
- Respiratory failure, apnea, or airway obstruction
B. Diagnostic / Therapeutic
- Visualization of laryngeal pathology (lesions, polyps, nodules, foreign bodies)
- Removal of foreign bodies from the larynx or upper trachea
- Biopsy of laryngeal lesions
- Injection laryngoplasty
- Laser treatment of laryngeal lesions
- Microlaryngoscopy for phonosurgery
C. Special Situations
- Anticipated difficult airway (known or predicted)
- Failed bag-mask ventilation
- Trauma patients requiring airway control
- Patients with altered consciousness (GCS < 8)
3. Contraindications
Absolute
- Complete upper airway obstruction where blind manipulation could cause total loss of airway
- Penetrating trauma to the upper airway (where manipulation may convert partial to complete transection, or cause hematoma formation)
- Suspected unstable cervical spine fracture (relative - needs inline stabilization)
Relative
- Severe epiglottitis (risk of precipitating complete obstruction - awake intubation or surgical airway preferred)
- Ludwig's angina or deep neck infection
- Anticipated anatomically impossible DL (known impossible mouth opening, fused joints)
- Trismus preventing mouth opening
As noted in Roberts & Hedges: DL is contraindicated in penetrating trauma to the upper airway because "visualization of the vocal cords may not be possible, and trauma caused by the laryngoscope blade can exacerbate swelling and edema of the airway."
4. Equipment
A. The Laryngoscope
A laryngoscope consists of two main components:
- Handle - contains the light source (battery-powered or fiberoptic); held in the left hand
- Blade - attaches to the handle; inserted into the mouth
B. Blade Types
There are two fundamental blade designs:
| Feature | Macintosh (Curved) | Miller (Straight) |
|---|---|---|
| Tip placement | In the vallecula (indirectly lifts epiglottis via hyoepiglottic ligament) | Under the epiglottis (directly lifts it) |
| Preferred in | Adults (uncomplicated) | Pediatrics, anterior larynx, long floppy epiglottis |
| Common adult size | Size 3 (or 4 for larger patients) | Size 2 |
| Tongue retraction | Better (wider flange) | Less effective |
| Dental trauma | Less likely | More likely (especially with prominent upper teeth) |
| ETT passage space | More room through oropharynx | Less room |
| Laryngospasm risk | Lower | Higher (stimulates superior laryngeal nerve) |
| Light source | In handle | Bulb at tip (may slightly hamper vision) |
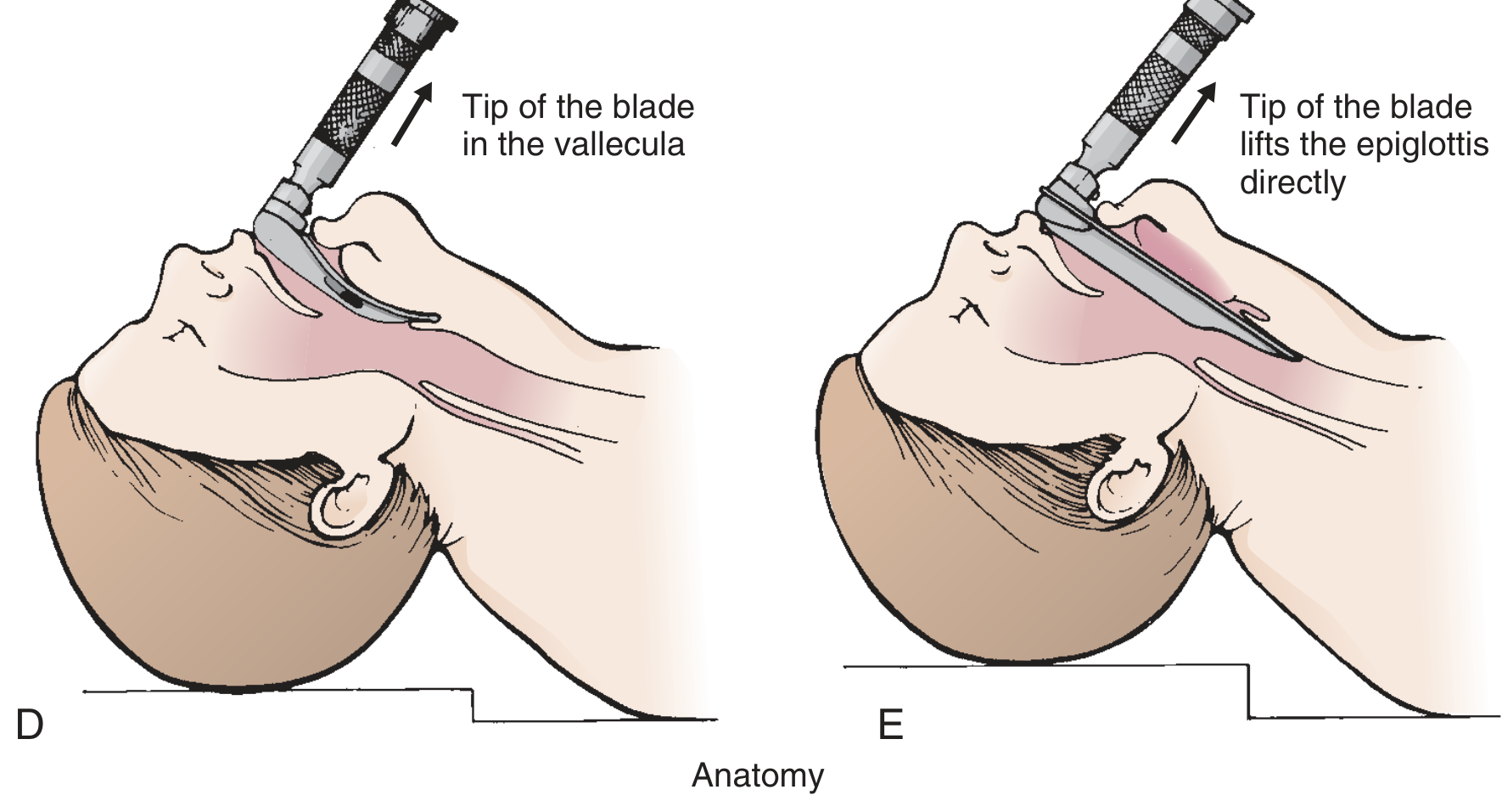
Macintosh blade tip sits in the vallecula (left); Miller blade lifts the epiglottis directly (right) - Roberts & Hedges
The curved blade tip fits into the vallecula and indirectly lifts the epiglottis via engagement of the hyoepiglottic ligament, whereas the straight blade goes under the epiglottis and lifts it directly. - Roberts & Hedges' Clinical Procedures in Emergency Medicine
C. Other Equipment Required
- Endotracheal tube (ETT): Adult males 7.5-9.0 mm ID; Adult females 7.0-8.0 mm ID; with stylet loaded
- 10 mL syringe for cuff inflation
- Suction apparatus (Yankauer catheter)
- Bougie (ETT introducer) - for difficult laryngoscopy
- Capnograph for confirmation
- Bag-valve-mask for pre/post-oxygenation
- Emergency surgical airway equipment (backup)
5. Patient Positioning - The Sniffing Position
Optimal positioning is the single most important preparation step. The goal is to align three anatomic axes:
- Oral axis (OA) - axis from the mouth
- Pharyngeal axis (PA) - axis of the pharynx
- Laryngeal axis (LA) - axis of the larynx (trachea)
The classical model was proposed by Bannister and Macbeth (1944).
The Sniffing Position achieves this alignment in two steps:
- Cervical flexion (~35°): Achieved by elevating the head on a firm cushion 7-9 cm - aligns the pharyngeal and laryngeal axes
- Atlantooccipital extension (~80°): Head extension at the neck - brings the oral axis closer into alignment with the other two
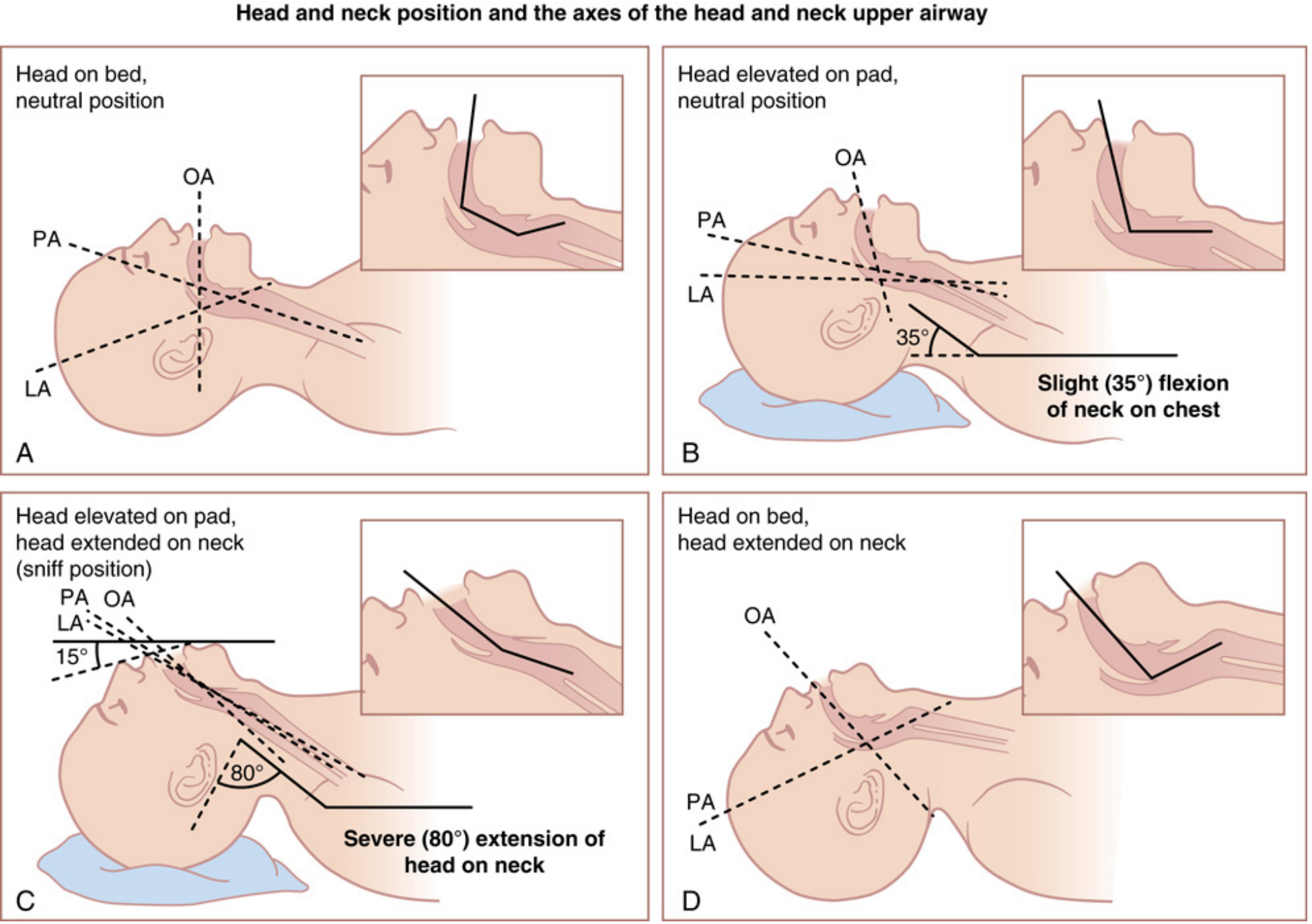
Panel C shows the optimal "sniffing position" with PA, OA, and LA in near-alignment - Miller's Anesthesia 10e
Special populations:
- Obese patients: Require elevation of shoulders and upper back ("ramped position") - align external auditory meatus with sternal notch
- Pediatric patients: Relatively larger occiput naturally places the head in slight flexion; a shoulder roll may be preferred
- C-spine precautions: In-line manual stabilization (not traction) is used; sniffing position is avoided
6. Technique - Step by Step
Preparation:
- Check all equipment - laryngoscope light, ETT cuff integrity, suction function
- Preoxygenate the patient (100% O₂ for 3-5 minutes, or 8 vital capacity breaths)
- Position in sniffing position; elevate bed so patient's head is at the level of the operator's lower sternum
- Have a skilled assistant present (for OELM, stylet removal)
Procedure:
- Open the mouth using the scissors technique - right thumb pushes caudally on right lower molars, index/middle finger pushes cranially on right upper molars
- Hold laryngoscope in the left hand - never switch hands
- Insert blade into the right side of the mouth, sweeping the tongue to the left using the flange
- Advance the blade progressively, identifying in sequence: base of tongue → epiglottis → posterior cartilages (arytenoids)
- Position the blade tip:
- Macintosh: advance into the vallecula
- Miller: advance under the epiglottis
- Apply lifting force - lift in the direction of the laryngoscope handle (at 45°, toward the junction of the opposite wall and ceiling). Never lever the blade on the upper teeth - this causes dental trauma
- Instruct assistant to retract right cheek for better visualization
- If view is inadequate: apply Optimal External Laryngeal Manipulation (OELM) - backward, upward, rightward pressure (BURP maneuver variant) on the thyroid cartilage, guided by the laryngoscopist
- Once cords visualized, never take your eyes off them
- Insert ETT from the right corner of the mouth (not midline) so it does not obstruct the view; advance until the cuff is 2-3 cm past the vocal cords
- Remove stylet when tip is at level of cords while holding ETT fixed (to minimize mucosal trauma)
- Inflate cuff and confirm placement
7. Cormack-Lehane Grading System
This system classifies the laryngoscopic view and predicts intubation difficulty (originally described by Cormack and Lehane, 1984):
| Grade | View | Clinical Significance |
|---|---|---|
| Grade 1 | Full view of the glottis (entire laryngeal aperture visible) | Easy intubation |
| Grade 2 | Only posterior portion of laryngeal aperture (arytenoids) visible | Usually straightforward; may need OELM |
| Grade 3 | Only epiglottis visible; no part of glottis seen | Difficult - use bougie |
| Grade 4 | Neither epiglottis nor glottis visible | Very difficult - alternate technique required |
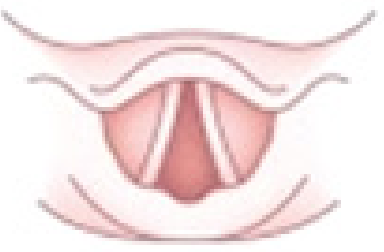
Grade 1 (Cormack-Lehane) - full laryngeal aperture visible - Miller's Anesthesia 10e
Grades 3 and 4 indicate a difficult laryngoscopy. When grades 3-4 are encountered:
- Verify optimal positioning
- Apply OELM
- Try a different blade size or style
- Use an ETT introducer (bougie)
- Consider video laryngoscopy or alternative airway technique
8. Confirmation of ETT Placement
After intubation, correct placement must be confirmed immediately:
Clinical signs (unreliable alone):
- Chest rise bilaterally on ventilation
- Condensation in the ETT
- Equal breath sounds bilaterally
- Absent breath sounds over epigastrium
Objective confirmation (gold standard):
- Capnography - a normal CO₂ waveform for at least 3 breaths is the most important and objective indicator. The "No Trace = Wrong Place" campaign (Royal College of Anaesthetists / Difficult Airway Society) mandates capnography confirmation in all settings
- Chest X-ray (definitive, post-procedure)
- Flexible bronchoscopy (when doubt remains)
9. Predictors of Difficult Laryngoscopy
(Box from Miller's Anesthesia, based on ASA Task Force Guidelines):
- Long upper incisors
- Prominent overbite
- Inability to protrude mandible
- Small mouth opening (< 3 cm interincisor distance)
- Mallampati classification III or IV
- High, arched palate
- Short thyromental distance (< 6 cm)
- Short, thick neck
- Limited cervical mobility
Pre-operative assessment using the LEMON mnemonic (Look externally, Evaluate 3-3-2 rule, Mallampati, Obstruction, Neck mobility) helps predict difficulty.
10. Complications
Immediate
| Complication | Mechanism |
|---|---|
| Dental trauma | Levering on upper incisors - most common complication |
| Lip/tongue laceration | Soft tissue impingement between blade and teeth |
| Esophageal intubation | Unrecognized - most dangerous; causes hypoxia, death |
| Right mainstem bronchus intubation | ETT advanced too far |
| Laryngospasm | Stimulation of superior laryngeal nerve (more with Miller blade) |
| Bronchospasm | Airway stimulation in reactive airways |
| Hypoxia | Prolonged attempt; failed intubation |
| Hypertension/tachycardia | Sympathetic stimulation from laryngoscopy |
| Aspiration | Loss of airway protective reflexes, regurgitation |
Airway Trauma
- Arytenoid dislocation
- Vocal cord hematoma or laceration
- Subglottic edema
- Pharyngeal/laryngeal perforation (rare)
- Tracheal mucosal trauma (from stylet)
Delayed
- Hoarseness or voice changes (vocal cord trauma)
- Sore throat (common, usually resolves in 48-72 h)
- Subglottic stenosis (rare, from prolonged or traumatic intubation)
- Tracheal stenosis
- Tracheitis
Cardiovascular
- Significant hypertension and tachycardia - can precipitate myocardial ischemia in susceptible patients
- Raised intracranial pressure (ICP) - relevant in head injury patients (lidocaine pre-treatment may attenuate)
11. Special Considerations
Pediatric Patients
- Straight blades (Miller) are preferred because the large, floppy epiglottis is best directly lifted
- The large tongue is more easily displaced with a straight blade
- Blade size is determined by placing the handle joint at the upper incisors - tip should reach the angle of the mandible (±1 cm)
- Uncuffed tubes are used in young children (< 8 years) to avoid subglottic injury; if cuffed, use 0.5 mm smaller
- Miller 0 or MacIntosh 1 only for premature newborns
Obese Patients
- Ramped position required (shoulders elevated)
- External auditory meatus aligned with sternal notch confirms adequate elevation
- Consider video laryngoscopy as first-line alternative
C-Spine Injury
- In-line stabilization (MILS) by assistant
- Sniffing position avoided; neutral position with MILS used
- OELM still applied as needed
12. Differences: Direct vs. Video Laryngoscopy (Brief Comparison)
| Feature | Direct Laryngoscopy | Video Laryngoscopy |
|---|---|---|
| View | Direct line of sight | Camera-assisted, indirect |
| Axis alignment | Required (sniffing position essential) | Less critical |
| Skill requirement | High (requires experience) | Easier to learn |
| Difficult airway | More challenging | Improved first-pass success |
| Cost | Low | Higher |
| Availability | Universal | Not always available |
13. Summary Points
- Direct laryngoscopy requires a laryngoscope held in the left hand, patient in the sniffing position, with blade inserted into the right side of the mouth sweeping tongue left
- The Macintosh blade tip goes into the vallecula; the Miller blade goes under the epiglottis
- Lift, never lever - force is directed at 45° toward the ceiling-wall junction
- OELM (backward-upward-rightward pressure on the larynx) improves the view
- Cormack-Lehane Grade 3-4 = difficult view; use bougie, change blade, or switch to video laryngoscopy
- Capnography is mandatory to confirm tracheal placement (No Trace = Wrong Place)
- Dental injury is the most common complication; unrecognized esophageal intubation is the most dangerous
- The maximum number of attempts should be limited to 3 (with each attempt optimized); failure triggers the difficult airway algorithm
Sources:
- Miller's Anesthesia, 10e (Vol. 2, Chapter 40)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, 7e (Chapter 4)
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9e (Chapter 113)
- Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia. 1984;39:1105
- ASA Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118:251-270
I want it in ENT context not anaesthesia
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive ENT-specific content. Here is the full ENT-focused essay on direct laryngoscopy:
Direct Laryngoscopy - ENT Essay
1. Introduction and Definition
Direct laryngoscopy (DL) in the ENT context refers to the transoral examination and surgical access to the larynx using a rigid laryngoscope passed perorally under general anaesthesia, providing unobstructed, magnified, binocular visualization of the entire endolarynx. Unlike the anaesthetic context where the primary goal is endotracheal intubation, the ENT surgeon uses direct laryngoscopy principally for:
- Detailed diagnostic assessment of laryngeal pathology
- Surgical treatment of laryngeal and hypopharyngeal lesions (microlaryngoscopy)
- Staging of head and neck malignancy
- Combined endoscopy of the upper aerodigestive tract
The procedure is performed in the operating theatre, typically as a day-case procedure under general anaesthesia, and requires close cooperation between the otolaryngologist and the anaesthetist on the shared airway.
"Accurate assessment of the larynx under general anaesthetic requires a systematic approach involving cooperative work on the shared airway between the otolaryngologist and the anaesthetist."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
2. Historical Background
The history of direct laryngoscopy is rich and ENT-specific:
- Claudius Galen (2nd century CE) - first recognized the larynx as the organ of voice production
- Avicenna (10th century) - described the muscular control of laryngeal cartilages
- Giovanni Morgagni (1700s) - connected vocal fold pathology to dysphonia
- Bozzini - first reported mirror visualization of the larynx (often wrongly credited to Manuel Garcia)
- Horace Green - described the first direct laryngeal surgical case: removal of a laryngeal polyp in an 11-year-old girl using a bent tongue spatula and sunlight
- Chevalier Jackson - formalized the position (cervicothoracic flexion with atlantooccipital extension) for laryngoscopic access, still used today
- Oskar Kleinsasser - pioneered adaptation of the operating microscope to direct laryngoscopy, establishing modern microlaryngoscopy and phonosurgery
3. Indications in ENT Practice
A. Diagnostic Indications
- Dysphonia - assessment of vocal fold lesions (nodules, polyps, cysts, sulcus vocalis, papillomatosis) when flexible laryngoscopy is inconclusive or surgical biopsy is needed
- Suspected laryngeal malignancy - biopsy for histological diagnosis and staging
- Stridor - in adults or children when the cause is unclear or requires operative intervention
- Dysphagia - combined pharyngoscopy and laryngoscopy
- Failed or incomplete outpatient examination - due to strong gag reflex, trismus, bulky or obstructive lesion, or poor patient cooperation
- Subglottic/tracheal assessment - in conjunction with bronchoscopy
B. Staging of Head and Neck Cancer
A specific, structured indication in ENT:
- Assessment of vocal cord mobility (mobile/impaired/fixed) - directly influences operability and choice of conservation surgery vs. total laryngectomy
- Assessment of subsites: vallecula, pyriform sinus apex, cricoarytenoid joint, interarytenoid region, anterior commissure, subglottis, postcricoid, cricopharynx
- Determining resectability and tumour extent - extent of involvement of the pre-epiglottic space, paraglottic space, pyriform apex, and cricoarytenoid joint are all recorded systematically during endoscopy (Scott-Brown's Endoscopy Table 16.1)
C. Therapeutic / Operative Indications
| Indication | Procedure |
|---|---|
| Vocal fold polyp, nodule, cyst | Microlaryngoscopic excision |
| Laryngeal papillomatosis (RRP) | CO₂ laser vaporization or microdebrider excision |
| Laryngeal carcinoma (early T1/T2) | Translaryngeal microsurgery (TLM) with CO₂ laser |
| Subglottic / glottic stenosis | Dilatation, laser division, steroid injection |
| Vocal fold paralysis / atrophy | Injection laryngoplasty (fat, Radiesse, hyaluronic acid) |
| Reinke's oedema | Microlaryngoscopic decompression |
| Granuloma / contact ulcer | Excision |
| Foreign body larynx | Removal under direct vision |
| Arytenoid dislocation | Manipulation |
| Subglottic haemangioma (paediatric) | Laser or propranolol treatment monitoring |
4. Contraindications
Absolute:
- Unstable atlantoaxial joint (e.g. rheumatoid arthritis, Down syndrome, odontoid peg fracture) - cervical extension required for laryngoscopy could cause cord injury
- Severe trismus that prevents mouth opening (relative)
Relative:
- Compromised or obstructed airway where general anaesthesia risks complete loss of airway - awake fibreoptic intubation or awake tracheostomy to be considered first
- High-risk patients (ASA III-IV) for tubeless/jet ventilation techniques
- Coagulopathy (for operative procedures)
- Active systemic infection
5. Pre-operative Assessment
Before performing direct laryngoscopy, the surgeon must assess:
- Airway patency - degree of obstruction guides anaesthetic technique
- Cervical mobility - full atlantooccipital extension must be possible; C-spine pathology must be excluded
- Dental assessment - note prominent upper incisors, loose or crowned teeth, dentures; dental guard must be used
- Mouth opening - sufficient interincisor distance
- Neck length and habitus - obesity, short bull neck, or micrognathia may predict difficult laryngoscopy
- Previous laryngoscopy records - any documented difficulty
- Outpatient laryngoscopy findings - fibreoptic or stroboscopic assessment prior to theatre provides a surgical roadmap
The checklist for direct laryngoscopy under anaesthesia (Scott-Brown's Table 16.1) includes systematic recording of every ENT subsite examined.
6. Equipment
A. Rigid Laryngoscopes
The ENT surgeon requires a set of rigid laryngoscopes of different sizes and designs:
- Standard laryngoscope - wide bore, used for initial exposure; passes perorally in the midline
- Anterior commissure laryngoscope (Kleinsasser) - narrower, angled design specifically to maximize view of the anterior glottis and anterior commissure; essential when this subsite is involved
- Distending laryngoscope - spring-loaded; holds the larynx open for bilateral access
- Subglottoscope - for examination of the subglottis and upper trachea
- Benjamin paediatric laryngoscopes - sized for children
"The widest laryngoscope to maximize vision is passed perorally in the midline and the tongue is negotiated in order to visualize the epiglottis. Different telescopes can be utilized to inspect the subsites of the endolarynx, such as the anterior commissure scope, which is designed to maximize the view of the anterior glottis."
- Scott-Brown's ORL HNS
B. Hopkins' Rod Telescopes (Rigid Endoscopes)
After laryngoscope insertion, rigid Hopkins' rod telescopes are introduced through the laryngoscope lumen to provide magnified, high-definition views:

Hopkins' rod endoscopes for laryngoscopy: 0°, 30°, and 70° - Scott-Brown's ORL
| Telescope | Use |
|---|---|
| 0° (straight forward) | Standard view of glottis and supraglottis |
| 30° | Ventricles, free edge and undersurface of vocal cord |
| 70° | Subglottis, anterior commissure from below |
These angled scopes allow inspection of areas not visible with straight-line vision.
C. Operating Microscope
The Carl Zeiss or Leica operating microscope is coupled to the laryngoscope via the suspension arm to provide:
- Binocular stereoscopic vision
- Variable magnification (typically ×6 to ×25)
- Both hands free for surgery
- CO₂ laser coupling via micromanipulator
D. Suspension System
- A fulcrum suspension bar is attached to the operating table or chest support
- The laryngoscope is suspended from this bar, freeing both hands for bimanual microsurgery
- External laryngeal counter-pressure (using an assistant's fingers or gauze and elastic tape) is applied to improve exposure
E. Other Equipment
- Microlaryngeal instruments: fine atraumatic forceps (Bouchayer), microscissors, microsuction
- Microlaryngeal tube (MLT): 16-22 French gauge; small-diameter cuffed ETT placed in the posterior glottis
- If laser: laser-resistant tube (non-combustible, non-reflective); indicator dye in cuff
- Suction and irrigation
- Photo-documentation system (high-definition still and video recording)
7. Anaesthetic Techniques for ENT Direct Laryngoscopy
In ENT, the shared airway creates a conflict between the need for ventilation and the need for an unobstructed surgical field. Options include:
A. Microlaryngoscopy Tube (MLT)
- Small-diameter cuffed ETT (16-22 French)
- Placed in the posterior glottis, leaving the anterior glottis, vocal folds, and anterior commissure accessible
- Safest option for high-risk patients
- For laser cases: laser-resistant tube mandatory; FiO₂ kept ≤ 30%
B. Total Intravenous Anaesthesia (TIVA) - Tubeless
- Propofol TIVA + topical lidocaine; patient breathes spontaneously
- No ETT in the field - ideal for fine anterior commissure work
- Not recommended for high-risk patients (ASA III/IV) or obstructed airways
- Requires specialist expertise
C. High-Frequency Jet Ventilation (HFJV)
- High-pressure jet (Venturi) ventilation administered via a catheter:
- Supraglottic - above the larynx
- Glottic - through the laryngoscope
- Transtracheal - via cricothyroidotomy
- Advantages: no combustible material in airway (safe for laser), completely clear operative field, allows deep anaesthesia
- Complications: pneumothorax (~1%), hypoventilation (~2%), surgical emphysema (~8%) in large multicentre series
- Contraindications: unstable or obstructed airway, emphysematous bullae, difficult access (micrognathia, overhanging teeth)
8. Patient Positioning
The position described by Chevalier Jackson remains standard:
- Patient supine
- Cervicothoracic junction flexed - aligns the pharyngeal and laryngeal axes
- Atlantooccipital joint fully extended - opens the laryngeal inlet and aligns the oral axis
This combination achieves the "sniffing position", bringing the three axes (oral, pharyngeal, laryngeal) into alignment to provide a direct line of sight from the mouth to the glottis.
Additional ENT considerations:
- Eye cover is applied (to prevent corneal injury from instruments or light)
- Dental protection (guard) is placed over the upper teeth before introducing the laryngoscope
- Antiseptic draping is applied
- External laryngeal counter-pressure may be needed for difficult or anterior larynges
- Bed height should allow the surgeon to work comfortably with the microscope
9. Operative Technique
Step 1: Initial Exposure
- Patient positioned, eye cover and dental guard applied
- Laryngoscope introduced perorally in the midline
- Tongue is swept aside and the epiglottis identified
- The laryngoscope elevates the epiglottis to visualize the larynx
- The widest appropriate laryngoscope is used to maximize the surgical field
Step 2: Suspension
- The laryngoscope is fixed to the suspension bar over the chest support
- This frees both the surgeon's hands for bimanual microsurgery
Step 3: Visualization
- Microscope is positioned above the laryngoscope for magnified binocular view
- Hopkins' rod telescopes (0°, 30°, 70°) are passed through the laryngoscope to inspect different subsites
- The entire endolarynx is examined systematically: supraglottis (epiglottis, aryepiglottic folds, arytenoids, ventricles), glottis (vocal folds, anterior and posterior commissure), and subglottis
Step 4: Documentation
- Site, extent, dimensions, shape, colour, and surface characteristics of any lesion are defined and recorded
- Vocal cord mobility and airway patency are recorded
- Printed operative diagrams and high-definition digital photo/video documentation are used
Step 5: Surgery
Microsurgical principles (Kleinsasser/Hirano):
- Instruments: fine, sharp, atraumatic microlaryngeal forceps (e.g. Bouchayer forceps); microscissors; microsuction
- Surgery should be as superficial as possible - limited to the mucosa and superficial lamina propria for benign disease
- Vocal ligament must be preserved for benign lesions - no mucosal stripping
- Deep extent of surgery should be limited to what is absolutely necessary
- Biopsies taken from suspicious lesion margins and base
10. Systematic Endoscopic Examination in ENT
In ENT cancer staging, the following subsites are assessed at direct laryngoscopy (Scott-Brown's checklist):
| Region | Subsite | Key Clinical Question |
|---|---|---|
| Oropharynx | Vallecula/base of tongue | Lateralized vs. crossing midline - impacts glossectomy decision |
| Oropharynx | Inferior tonsil pole | Resectable vs. parapharyngeal spread |
| Hypopharynx | Pyriform apex | Conservation laryngeal surgery feasibility |
| Hypopharynx | Cricoarytenoid joint | Joint mobility and phonosurgical planning |
| Hypopharynx | Cricopharynx | Circumferential resection vs. reconstruction |
| Hypopharynx | Posterior pharyngeal wall | Midline crossing - determines reconstruction |
| Glottis | Vocal cords | Mobile/impaired/fixed - defines T stage and treatment |
| Glottis | Anterior commissure | Pre-epiglottic space involvement |
| Glottis | Paraglottic space | Organ preservation feasibility |
| Subglottis | Extent | >1 cm anteriorly or >5 mm posteriorly - precludes conservation surgery |
| Interarytenoid | Involvement | Precludes conservation surgery and near-total laryngectomy |
11. Microlaryngoscopy Setup

Microlaryngoscopy setup: patient in cervical flexion/extension position; laryngoscope suspended by fulcrum bar freeing both hands; operating microscope positioned - Scott-Brown's ORL HNS
12. New Techniques in Laryngeal Endoscopy
Adjuncts used during or alongside direct laryngoscopy in ENT practice:
- Contact endoscopy - Hopkins' rod touched to mucosal surface under topical methylene blue; allows in-vivo histological assessment of the mucosa at cellular level
- Narrow band imaging (NBI) - enhances visualization of mucosal vascular pattern; helps distinguish benign from malignant lesions intraoperatively
- Autofluorescence endoscopy - detects dysplastic/malignant tissue by detecting differences in fluorescence from normal mucosa
- Optical coherence tomography (OCT) - cross-sectional subsurface imaging; assesses depth of mucosal invasion
- Laser microsurgery (CO₂, KTP, Nd:YAG) - used for precise tissue excision, vaporization, or coagulation; CO₂ laser is most widely used in ENT laryngeal surgery
13. Complications
Immediate (Intraoperative)
| Complication | Comments |
|---|---|
| Dental trauma | Most common; prevented by dental guard; upper incisors at risk |
| Lip/tongue laceration | Soft tissue impingement between laryngoscope and teeth |
| Laryngospasm | On extubation or during light anaesthesia; treat with deepening anaesthesia, succinylcholine if severe |
| Haemorrhage | From biopsies or laser; usually controllable endoscopically |
| Airway fire | Rare but catastrophic; occurs with laser + oxygen + flammable ETT; prevented by laser-safe tube, FiO₂ ≤ 30%, saline-filled cuffs |
| Failed exposure / difficult laryngoscopy | Prominent teeth, obesity, rigid neck, anterior larynx - have multiple laryngoscopes available |
Immediate (Physiological)
- Sympathetic stress response - up to 4% of patients show signs of cardiovascular ischaemia post-operatively (Scott-Brown's)
- Hypertension and tachycardia - from laryngoscopy stimulation; relevant in cardiac patients
Postoperative
| Complication | Comments |
|---|---|
| Sore throat / odynophagia | Common, resolves in 48-72 h |
| Hoarseness | May be new or worsened from vocal fold manipulation |
| Laryngeal oedema | Risk minimized by perioperative dexamethasone 8 mg IV |
| Post-operative airway obstruction | Due to oedema; may require reintubation or tracheostomy |
| Vocal fold scar / synechia | Most significant long-term complication of phonosurgery; permanent dysphonia from damage to the lamina propria |
| Anterior glottic web | Bilateral anterior commissure surgery; prevented by staged procedures or keel placement |
| Jet ventilation complications | Pneumothorax (1%), surgical emphysema (8%), hypoventilation (2%) |
| Arytenoid dislocation | Rare; from forceful laryngoscopy |
14. Comparison of Laryngoscopy Techniques in ENT
| Feature | Mirror Laryngoscopy | Flexible Nasoendoscopy | Rigid Laryngoscopy (Outpatient) | Direct Laryngoscopy (GA) |
|---|---|---|---|---|
| Setting | Outpatient | Outpatient | Outpatient | Theatre under GA |
| Anaesthesia | Topical/none | Topical/none | Topical | General |
| Light source | Reflected | Built-in | Fiberoptic | Fiberoptic + microscope |
| Image quality | Low | Good | High-definition | Best (magnified) |
| Stroboscopy | Limited | Yes | Yes | Limited |
| Bimanual surgery | No | No | No | Yes |
| Vocal cord mobility during phonation | Possible | Yes (best) | Yes | No (under GA) |
| Biopsy | No | No | No | Yes |
| Disadvantages | Gag reflex; no record | Cannot biopsy | Gag reflex; no biopsy | Requires GA; dental risk |
15. Special Considerations in ENT
Paediatric Laryngoscopy
- Children under 5-6 years usually cannot cooperate with flexible laryngoscopy for full structural assessment - microlaryngoscopy under GA required
- The paediatric larynx is high and anterior; this is why Green was able to perform the first direct laryngoscopic surgery in a child using a tongue spatula and sunlight
- A 2.2 mm fibreoptic endoscope is used from infancy; 4 mm if possible
- Vocal cord mobility assessment on awakening from GA is still performed but is crude - awake assessment is preferred when feasible
- Age 1-5: Compliance limited; microlaryngoscopy often necessary
- Age >6: Rigid laryngoscopy for stroboscopy gives excellent detail
Recurrent Respiratory Papillomatosis (RRP)
- Requires repeated direct laryngoscopy sessions (often every 3-6 months) for disease control
- CO₂ laser or microdebrider excision under suspension microlaryngoscopy
- Jet ventilation preferred to avoid seeding papilloma virus into distal airway via tube
Transoral Laser Microsurgery (TLM)
- CO₂ laser delivered through a micromanipulator coupled to the operating microscope
- Used for T1/T2 laryngeal carcinoma; also supraglottic cancers
- Advantages over open surgery: no neck incision, preservation of laryngeal function, day-case or short stay, repeatable
- Requires full endolaryngeal exposure for access
16. Key Points Summary
- Direct laryngoscopy in ENT = operative/diagnostic laryngoscopy under GA in the theatre, not intubation
- The primary goal is diagnostic assessment and/or therapeutic endolaryngeal surgery, not airway control
- The Chevalier Jackson position (cervicothoracic flexion + atlantooccipital extension) is standard
- The laryngoscope is suspended by a fulcrum bar to free both hands for bimanual microsurgery
- Hopkins' rod telescopes (0°, 30°, 70°) + operating microscope provide high-magnification assessment of all endolaryngeal subsites
- Anaesthetic technique is a shared decision - MLT, TIVA tubeless, or HFJV depending on the lesion and risk
- For laser surgery: laser-resistant tube, FiO₂ ≤ 30%, saline-filled cuffs - to prevent airway fire
- Benign phonosurgery: stay superficial, preserve the vocal ligament, no mucosal stripping
- Perioperative dexamethasone reduces post-operative laryngeal oedema
- Photo-documentation is standard practice for medicolegal and clinical record purposes
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8e (Chapters 61, 67; Tables 16.1, 16.2)
- Cummings Otolaryngology Head & Neck Surgery, 7e (Chapters 60, 184)
- Bailey and Love's Short Practice of Surgery, 28e (Chapter 52)
- Scott-Brown's ORL HNS - Vol 1 (Chapter on Laryngeal Microsurgery)
This is a shared conversation. Sign in to Orris to start your own chat.