Anatomy - boundaries and contents of orbits and extraocular muscles
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have thorough material from Gray's Anatomy, Kanski's Clinical Ophthalmology, KJ Lee's Essential Otolaryngology, and Neuroanatomy through Clinical Cases. I can now compose a comprehensive, well-structured answer.
Anatomy of the Orbits and Extraocular Muscles
1. Overview
The orbits are paired pyramidal cavities in the upper half of the face, below the anterior cranial fossa and anterior to the middle cranial fossa. Each orbit contains the eyeball, optic nerve, extraocular muscles, lacrimal apparatus, adipose tissue, fascia, and the vessels and nerves supplying these structures.
The orbit has the shape of a four-sided pyramid, with its wide base opening anteriorly onto the face and its apex directed posteromedially toward the optic canal.
- Gray's Anatomy for Students
2. Bony Boundaries
Seven bones contribute to each orbit: frontal, zygomatic, maxilla, lacrimal, ethmoid, sphenoid, and palatine.
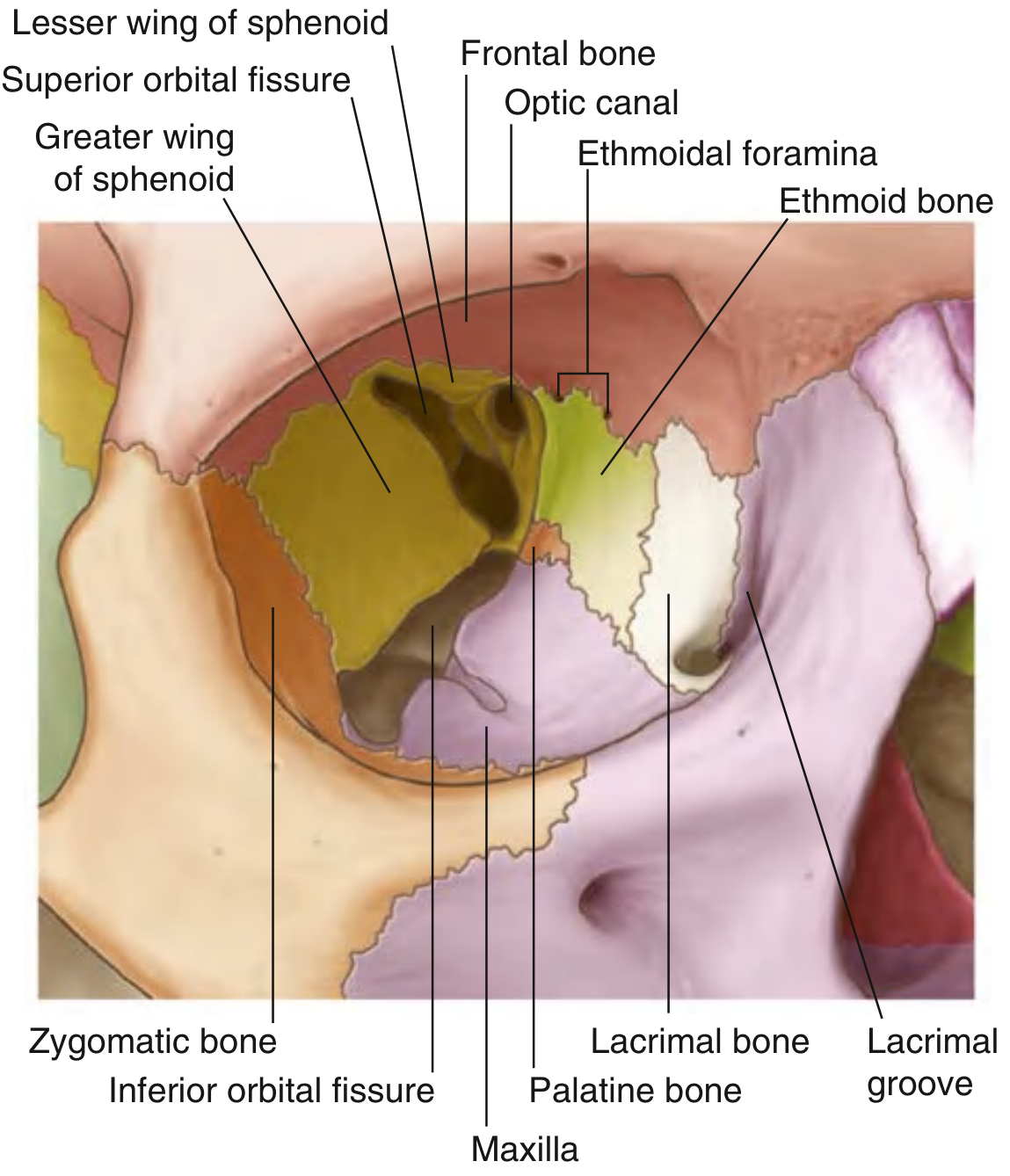
Fig. 8.79 — Bones of the Orbit (Gray's Anatomy for Students)
Orbital Rim (Base)
| Side | Bone(s) |
|---|---|
| Superior | Frontal bone |
| Medial | Frontal process of maxilla |
| Inferior | Zygomatic process of maxilla + zygomatic bone |
| Lateral | Zygomatic bone + zygomatic process of frontal bone |
Four Walls
Roof (Superior wall)
- Orbital part of the frontal bone (main contributor) + lesser wing of sphenoid posteriorly
- Features: trochlear fovea anteromedially (attachment for the superior oblique pulley) and lacrimal fossa anterolaterally (for the orbital part of lacrimal gland)
- Separates orbit from the anterior cranial fossa
Medial wall
- Maxilla (frontal process), lacrimal bone, ethmoid (orbital plate - the largest contributor, contains ethmoidal air cells), sphenoid (posteriorly)
- Thinnest wall (lamina papyracea of ethmoid) - fractures here allow air into the orbit
- Contains the lacrimal groove (bounded by anterior lacrimal crest of maxilla and posterior lacrimal crest of lacrimal bone)
- Anterior and posterior ethmoidal foramina are at the junction of medial wall and roof (transmit anterior/posterior ethmoidal nerves and vessels)
- The two medial walls are parallel to each other
Floor (Inferior wall)
- Orbital surface of maxilla (main contributor) + small parts of zygomatic and palatine bones
- Also forms the roof of the maxillary sinus
- The inferior orbital fissure runs along the posterolateral boundary of the floor
- Most susceptible to blowout fractures, often trapping the inferior rectus and inferior oblique muscles
Lateral wall
- Anteriorly: zygomatic bone; posteriorly: greater wing of sphenoid
- Thickest, strongest wall
- The superior orbital fissure lies between the greater and lesser wings of sphenoid (between the roof and lateral wall)
- Gray's Anatomy for Students; KJ Lee's Essential Otolaryngology
3. Key Openings
Superior Orbital Fissure (SOF)
- Located between the greater and lesser wings of the sphenoid, between the roof and lateral wall
- Transmits: CN III (oculomotor), CN IV (trochlear), CN V1 (ophthalmic - lacrimal, frontal, nasociliary branches), CN VI (abducens), superior ophthalmic vein, orbital branch of the middle meningeal artery, recurrent branch of lacrimal artery
- SOF syndrome: ophthalmoplegia + ptosis + fixed dilated pupil, WITHOUT vision loss
Inferior Orbital Fissure (IOF)
- Between the greater wing of sphenoid, orbital surface of maxilla, and orbital process of palatine bone
- Transmits: CN V2 branches (infraorbital nerve + zygomatic nerve), branches from sphenopalatine ganglion to lacrimal gland, infraorbital artery and vein, ophthalmic vein branch
Optic Canal
- Formed by the lesser wing of sphenoid
- Runs from the middle cranial fossa to the orbital apex
- Transmits: optic nerve (CN II) + ophthalmic artery
- Orbital apex syndrome: complete ophthalmoplegia + ptosis + fixed dilated pupil + visual loss (due to CN II, III, IV, V1, VI involvement)
- KJ Lee's Essential Otolaryngology; Gray's Anatomy for Students
4. Contents of the Orbit
| Structure | Details |
|---|---|
| Eyeball | Globe resting in orbital fat |
| Optic nerve (CN II) | From globe to optic canal |
| 6 extraocular muscles | See Section 5 |
| Lacrimal gland | In lacrimal fossa (anterolateral roof) |
| Lacrimal sac | In lacrimal groove (anteromedial wall) |
| Ophthalmic artery | Branch of internal carotid, enters via optic canal |
| Ophthalmic veins (superior and inferior) | Drain to cavernous sinus |
| CN III, IV, VI | Motor nerves to extraocular muscles |
| CN V1 branches | Lacrimal, frontal (supraorbital, supratrochlear), nasociliary |
| Ciliary ganglion | Parasympathetic relay for pupillary constriction |
| Orbital fat | Cushions globe, facilitates movement |
| Periorbita | Periosteum lining the bony orbit |
The orbit is lined by the periorbita (fibrous periosteum), loosely attached to the orbital walls except at the orbital margin, suture lines, fissures, and trochlear fossa. Orbital fat fills remaining spaces, cushioning the globe.
- Scott-Brown's Otorhinolaryngology; Gray's Anatomy for Students
5. Extraocular Muscles
There are six extraocular muscles per eye. The lateral, medial, superior and inferior recti arise from the annulus of Zinn (common tendinous ring) at the orbital apex. The obliques have different origins.
The Six Muscles
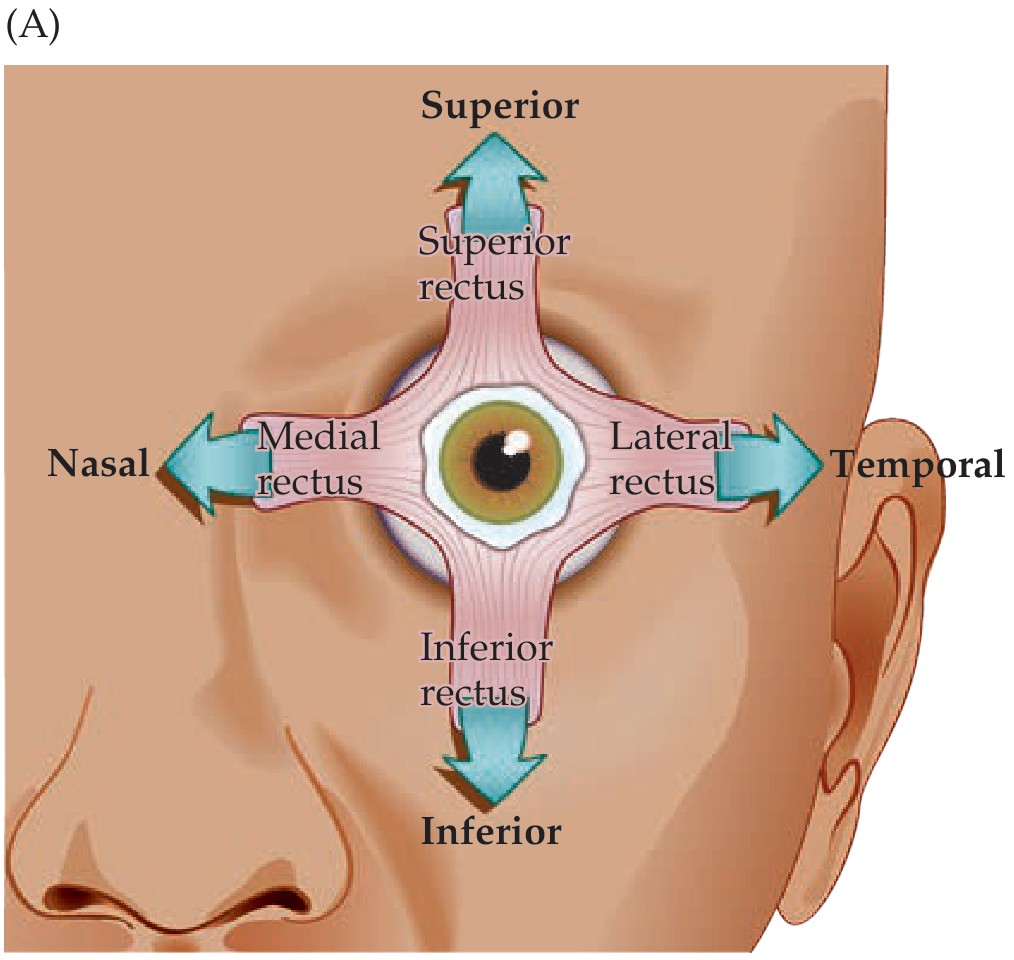
Rectus muscles and primary pull directions (Neuroanatomy through Clinical Cases)
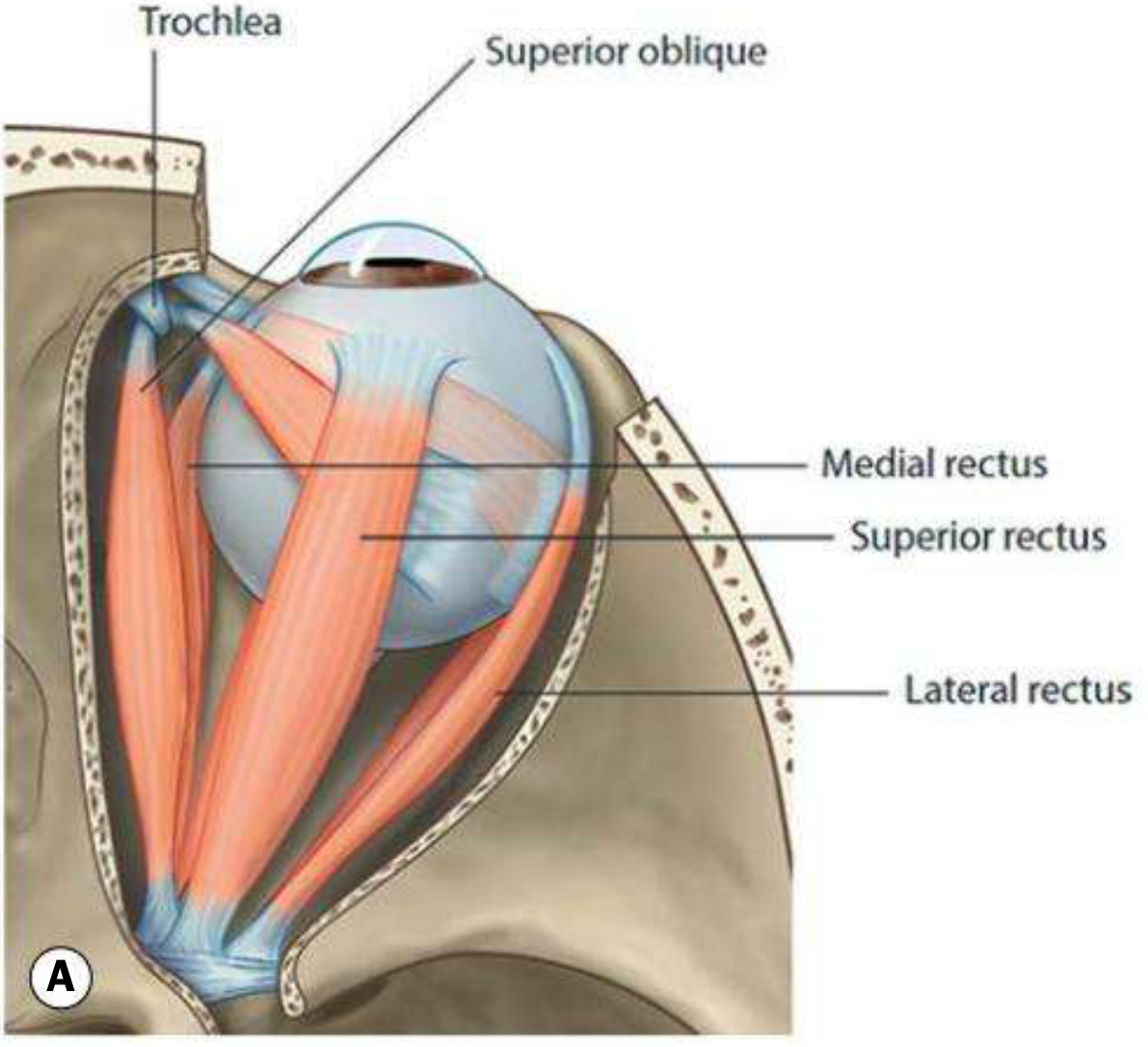
Superior view of orbital muscles (Kanski's Clinical Ophthalmology)
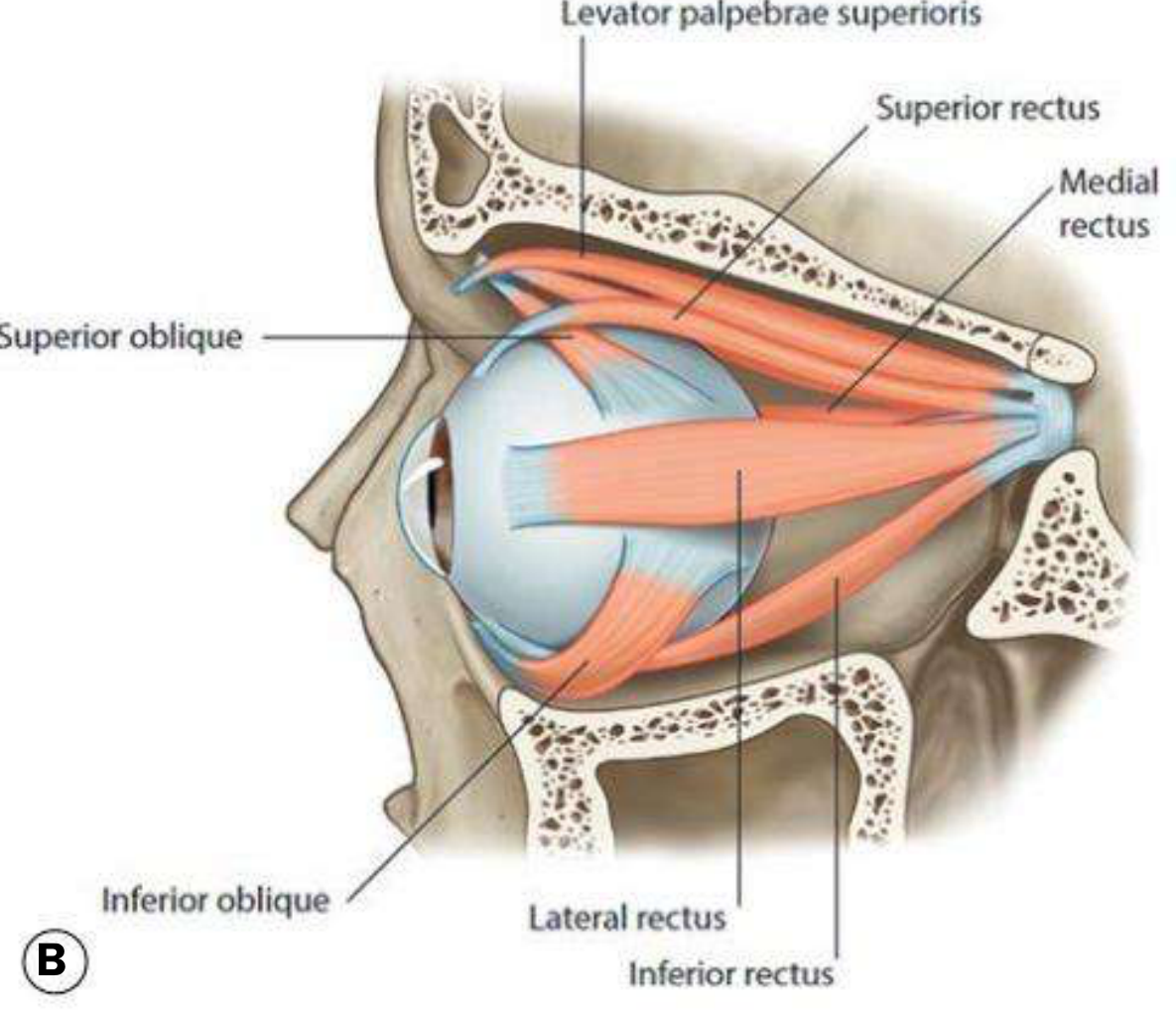
Lateral view of orbital muscles (Kanski's Clinical Ophthalmology)
Detailed Muscle Table
| Muscle | Origin | Insertion (from limbus) | Nerve | Primary action | Secondary actions |
|---|---|---|---|---|---|
| Medial rectus | Annulus of Zinn | 5.5 mm (nasal limbus) | CN III | Adduction | None |
| Lateral rectus | Annulus of Zinn | 6.9 mm (temporal limbus) | CN VI | Abduction | None |
| Superior rectus | Annulus of Zinn | 7.7 mm (superior limbus) | CN III (superior div.) | Elevation | Adduction, intorsion |
| Inferior rectus | Annulus of Zinn | 6.5 mm (inferior limbus) | CN III (inferior div.) | Depression | Adduction, extorsion |
| Superior oblique | Sphenoid (superomedial to optic foramen) | Posterior upper temporal quadrant (via trochlea) | CN IV | Intorsion | Depression, abduction |
| Inferior oblique | Anterior medial orbital floor (not from apex) | Posterior inferior surface | CN III (inferior div.) | Extorsion | Elevation, abduction |
Mnemonic for nerve supply: LR6(SO4)3 - Lateral Rectus = CN VI; Superior Oblique = CN IV; all others = CN III.
- Kanski's Clinical Ophthalmology; KJ Lee's Essential Otolaryngology
The Annulus of Zinn
The four recti and the levator palpebrae superioris originate from the annulus of Zinn at the orbital apex. Together, the four recti form the muscle cone (intraconal space), which is important surgically and radiologically.
Spiral of Tillaux
The insertions of the four recti follow a spiral pattern with increasing distance from the limbus:
MR (5.5 mm) → IR (6.5 mm) → LR (6.9 mm) → SR (7.7 mm)
This is a key surgical landmark.
The Trochlea
- Located at the angle between the superior and medial walls of the orbit
- Only cartilage in the orbit
- The tendon of the superior oblique passes through it, changing direction to insert on the posterior upper temporal quadrant of the globe
- A displaced trochlea causes diplopia on downward gaze
- Trochleitis causes peritrochlear pain without extraocular movement deficit
6. Muscle Actions and Eye Positions
The orbital axis forms a 22.5° (approximately 23°) angle with both the lateral and medial walls. In primary gaze position, the visual axis is 23° from the orbital axis.
- When the eye is abducted 23°: visual axis aligns with superior/inferior rectus - these act as pure elevators/depressors
- When the eye is adducted 51°: visual axis aligns with superior/inferior oblique - these act as pure depressors/elevators
This is why:
- Superior rectus is best tested with eye abducted (looking out)
- Superior oblique is best tested with eye adducted (looking in)
Cardinal Directions of Gaze (Yoke Muscles)
| Gaze direction | Right eye muscle | Left eye muscle |
|---|---|---|
| Right | Lateral rectus | Medial rectus |
| Left | Medial rectus | Lateral rectus |
| Up-right | Superior rectus | Inferior oblique |
| Down-right | Inferior rectus | Superior oblique |
| Up-left | Inferior oblique | Superior rectus |
| Down-left | Superior oblique | Inferior rectus |
- KJ Lee's Essential Otolaryngology
7. Levator Palpebrae Superioris
Though not a formal extraocular muscle, the levator palpebrae superioris is always considered with the orbital muscles:
- Origin: Lesser wing of sphenoid
- Insertion: Superior tarsal plate and skin of upper lid
- Innervation: CN III (oculomotor nerve)
- Action: Elevates the upper eyelid
- Horner's syndrome (loss of sympathetic innervation to superior tarsal muscle/Muller's muscle) gives partial ptosis; complete ptosis implies CN III lesion
8. Clinical Correlates
| Condition | Muscles/Structures | Key Feature |
|---|---|---|
| CN III palsy | SR, IR, MR, IO, levator | Eye "down and out," ptosis, dilated pupil |
| CN IV palsy | Superior oblique | Vertical diplopia, worse on downward gaze; head tilt |
| CN VI palsy | Lateral rectus | Medial deviation (convergent squint), horizontal diplopia |
| SOF syndrome | CN III, IV, V1, VI | Ophthalmoplegia + ptosis + no vision loss |
| Orbital apex syndrome | CN II + SOF structures | As above + vision loss |
| Blowout fracture (floor) | IR, IO entrapment | Upward gaze restriction, diplopia; more common in young patients |
| Medial wall fracture | Orbital emphysema | Air on imaging; worse on nose-blowing |
| Trochleitis | Superior oblique trochlea | Peritrochlear pain, no EOM deficit |
Sources: Gray's Anatomy for Students; Kanski's Clinical Ophthalmology 10th ed.; KJ Lee's Essential Otolaryngology; Neuroanatomy through Clinical Cases 3rd ed.; Scott-Brown's Otorhinolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.