How to send ecg to rule out diagnosis
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "electrocardiography"[MeSH Terms]
Reading File
Searching PubMed
"pulmonary embolism" AND "electrocardiogram" AND diagnosis
Reading File
Loading Image
I now have detailed textbook content and the ECG scoring table. Here is a thorough answer:
ECG in Pulmonary Embolism (PE): How to Use It for Diagnosis
The ECG is not sensitive or specific enough to confirm or exclude PE on its own, but it plays a supporting role in the diagnostic workup. Here's what you need to know:
Key Point: ECG Cannot "Rule Out" PE
A normal ECG does not exclude PE. The ECG in PE is generally nonspecific, and most findings reflect acute right heart strain from the obstructed pulmonary vasculature. Computer interpretations of ECGs frequently miss these subtle PE patterns - they require manual clinical review.
Classic ECG Findings in PE (suggest, not confirm)
These findings increase the probability of PE when present:
| Finding | What it represents |
|---|---|
| Sinus tachycardia (HR >100 bpm) | Most common finding (~50% of PE cases) |
| S1Q3T3 pattern | Deep S wave in lead I, Q wave + inverted T wave in lead III - right ventricular strain |
| T-wave inversion in V1-V4 | Right ventricular ischemia/strain pattern |
| Incomplete or complete right bundle branch block (RBBB) | Acute right heart pressure overload |
| Right axis deviation | Right ventricular strain |
| Atrial fibrillation or flutter | Less common but can occur with acute cor pulmonale |
The S1Q3T3 pattern is the "classic" teaching point, though it appears in only ~20% of PE cases and is not pathognomonic.
ECG Severity Scoring (G Score)
A clinical ECG score can assess severity once PE is diagnosed (higher score = higher mortality):
| ECG Characteristic | Score |
|---|---|
| Tachycardia (>100 bpm) | 2 |
| Incomplete right bundle branch block | 2 |
| Complete right bundle branch block | 3 |
| T-wave inversion in leads V1-V4 | 4 |
| T-wave inversion in V1: 1-2 mm | 1; >2 mm: 2 |
| T-wave inversion in V2: 1-2 mm | 2; >2 mm: 3 |
- Tintinalli's Emergency Medicine, p. 432-433
Example ECG in Severe PE
Here is a 12-lead ECG showing multiple PE features - tachycardia, incomplete RBBB, S1Q3T3 pattern, and anterior T-wave inversions:
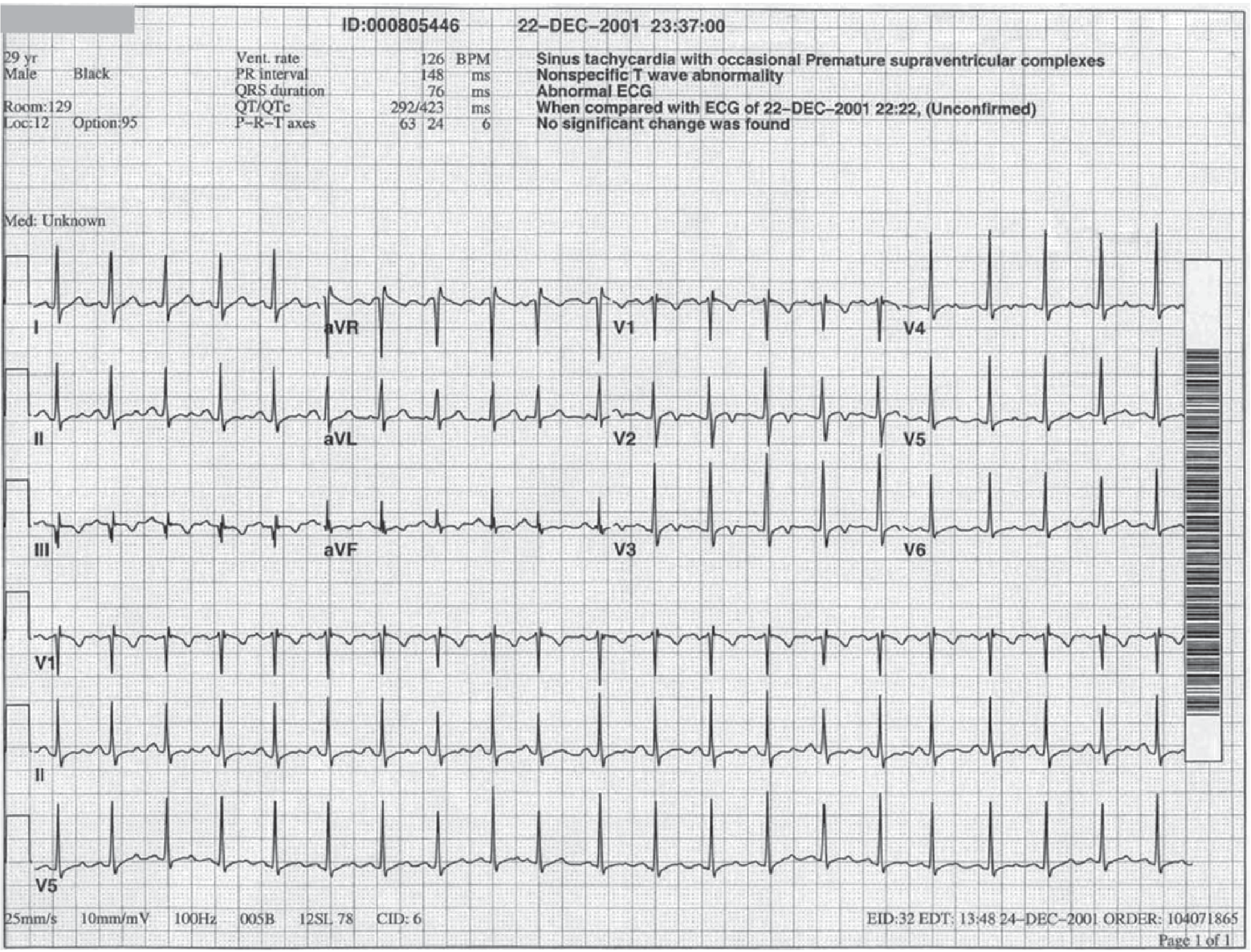
ECG shows: tachycardia, incomplete RBBB, S1Q3T3, and T-wave inversion in anterior leads - contributed by Department of Emergency Medicine, Wake Forest Baptist Hospital.
What the ECG IS Useful For in Suspected PE
- Ruling out competing diagnoses - The ECG helps exclude acute MI (ST elevations, Q waves in coronary territories), pericarditis, and arrhythmias that could explain the patient's symptoms.
- Raising suspicion - Multiple right strain findings together increase pre-test probability.
- Guiding further workup - In a patient with dyspnea + pleuritic chest pain + normal or right-strain ECG, this should trigger further PE evaluation (Wells score + D-dimer, or CT pulmonary angiography).
Diagnostic Algorithm (PE context)
ECG is used alongside - not instead of - validated tools:
- Wells score (clinical pre-test probability)
- D-dimer: if low probability + negative D-dimer → PE effectively excluded
- CT Pulmonary Angiography (CTPA): gold standard imaging
- V/Q scan: alternative when CTPA contraindicated
- Echo: bedside assessment of right ventricular dysfunction in high-risk patients
Bottom Line
| Situation | Meaning |
|---|---|
| Normal ECG | Does NOT rule out PE |
| Sinus tachycardia alone | Mildly raises concern, nonspecific |
| S1Q3T3 + anterior T inversions + RBBB | Strongly suggests significant PE with RV strain |
| ECG findings of STEMI pattern | Points away from PE, toward ACS |
The ECG is best used in PE workup as a tool to raise suspicion and exclude other diagnoses - never as a standalone rule-out test. A structured clinical probability assessment combined with D-dimer and/or CTPA remains the validated approach for ruling out PE.
This is a shared conversation. Sign in to Orris to start your own chat.