Normal distal femur anatomy for total knee Arthroplasty
Reading File
Finding Sources
Finding Sources
Searching the Web
distal femur anatomy total knee arthroplasty surgical landmarks condyles
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from Campbell's Operative Orthopaedics 15th Ed (2026) and the Imaging Anatomy atlas. Let me compile the complete answer.
Normal Distal Femur Anatomy for Total Knee Arthroplasty
Overview
The distal femur is the key bony landmark that determines femoral component positioning in TKA. It terminates in medial and lateral condyles of unequal size and shape - they do not demonstrate parallel sagittal architecture, which directly complicates knee biomechanics and component orientation decisions.
The knee is composed of three articulations formed by the distal femur, proximal tibia, and patella: the medial femorotibial, lateral femorotibial, and patellofemoral compartments, all contained within a communicating synovial capsule.
- Imaging Anatomy Text and Atlas, Vol. 3 (p. 751)
Key Anatomical Axes of the Distal Femur
These four axes form the backbone of distal femoral component alignment in TKA:
1. Anteroposterior (AP) Axis - "Whiteside's Line"
A line drawn from the deepest point of the trochlear groove anteriorly to the center of the posterior intercondylar notch. It runs perpendicular to the epicondylar axis. Making the posterior femoral cut perpendicular to this line places the femoral component in the correct rotational position.
2. Transepicondylar Axis (TEA)
A line connecting the medial and lateral femoral epicondyles. This is considered the most reliable rotational landmark. The posterior femoral cut is made parallel to the TEA, which results in a cut that is approximately 3 degrees externally rotated relative to the posterior condylar axis in a normal male femur.
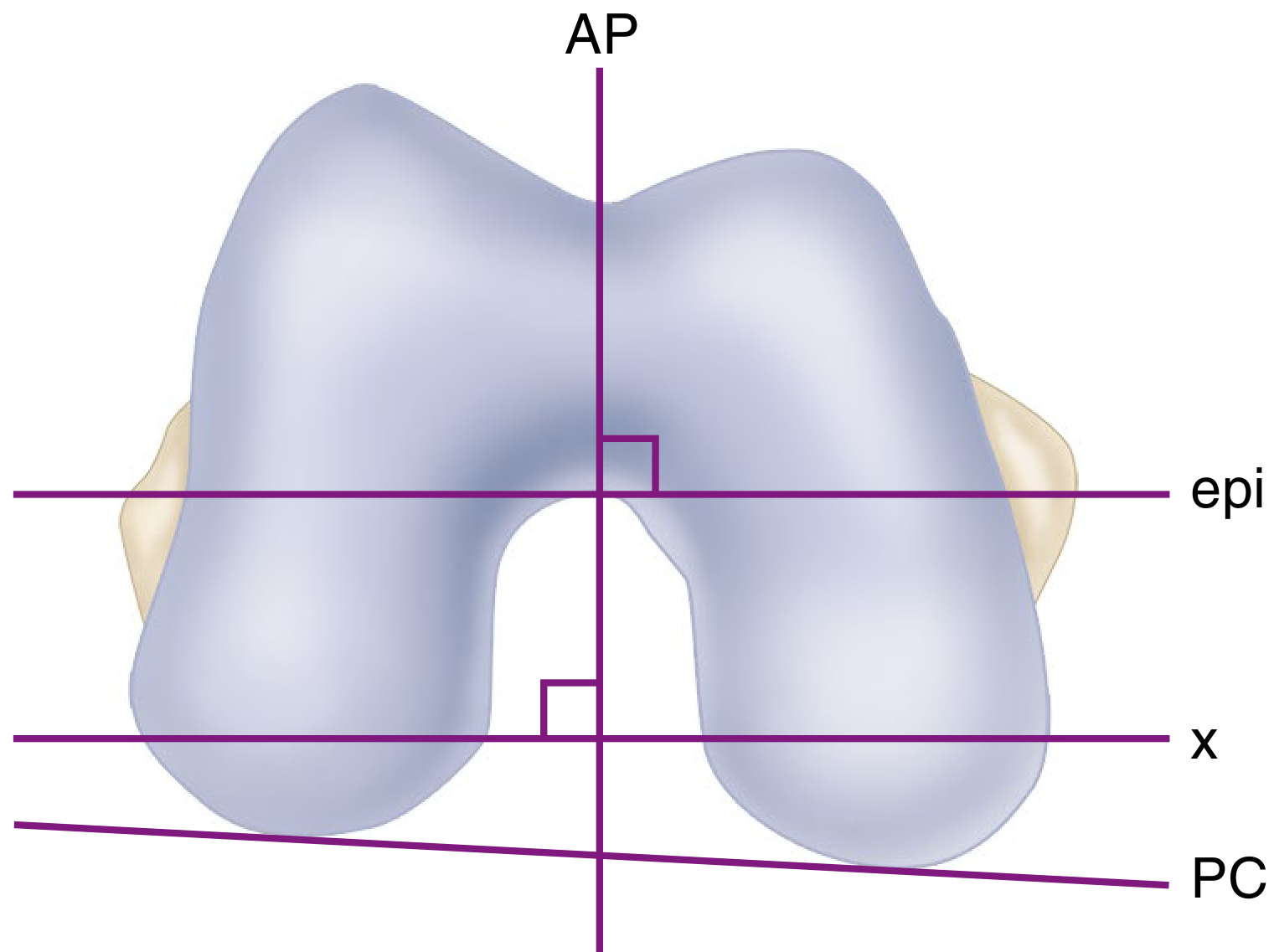
FIGURE: Inferior view showing the AP axis (vertical), epicondylar axis (epi), resection line (x), and posterior condylar axis (PC) - resection perpendicular to the AP axis or parallel to the epi axis produces a line ~3 degrees externally rotated from the PC axis. - Campbell's Operative Orthopaedics 15th Ed, Fig. 8.36
3. Posterior Condylar Axis (PCA)
A line along the posterior surfaces of the medial and lateral condyles. In a normal femur, making the posterior cut in 3 degrees of external rotation relative to this line approximately parallels the epicondylar axis and creates a rectangular flexion gap.
Critical caveat: In valgus knees with a hypoplastic lateral femoral condyle, relying solely on the posterior condylar axis leads to internal rotation of the femoral component - a major source of patellofemoral complications.
4. Mechanical vs. Anatomic Axis
- The mechanical axis runs from the center of the femoral head to the center of the knee
- The anatomic axis runs along the femoral diaphysis
- These form an angle of 5-7 degrees valgus - this is the angle used for the distal femoral cut to restore a neutral limb mechanical axis
Distal Femoral Cuts in TKA
| Cut | Purpose | Key Angle/Parameter |
|---|---|---|
| Distal femoral cut | Restores extension gap, joint line height | 5-7° valgus to mechanical axis |
| Anterior femoral cut | Sets anterior flange position, prevents notching | Based on anterior cortex (anterior referencing) |
| Posterior femoral cut | Determines flexion gap height | Thickness = posterior condyle of component |
| Anterior/posterior chamfer cuts | Transition cuts between resection planes | Match component geometry |
Distal Cut Depth
The amount of bone resected from the distal femur equals the distal condylar thickness of the femoral component. If a posterior cruciate-substituting (PS) prosthesis is used, an additional 2 mm of distal femoral resection may be performed to compensate for the increased flexion gap from PCL sacrifice. Elevation of joint line more than 4 mm should be avoided.
Femoral Component Rotation - Determining References
This is intraoperatively determined using multiple landmarks:
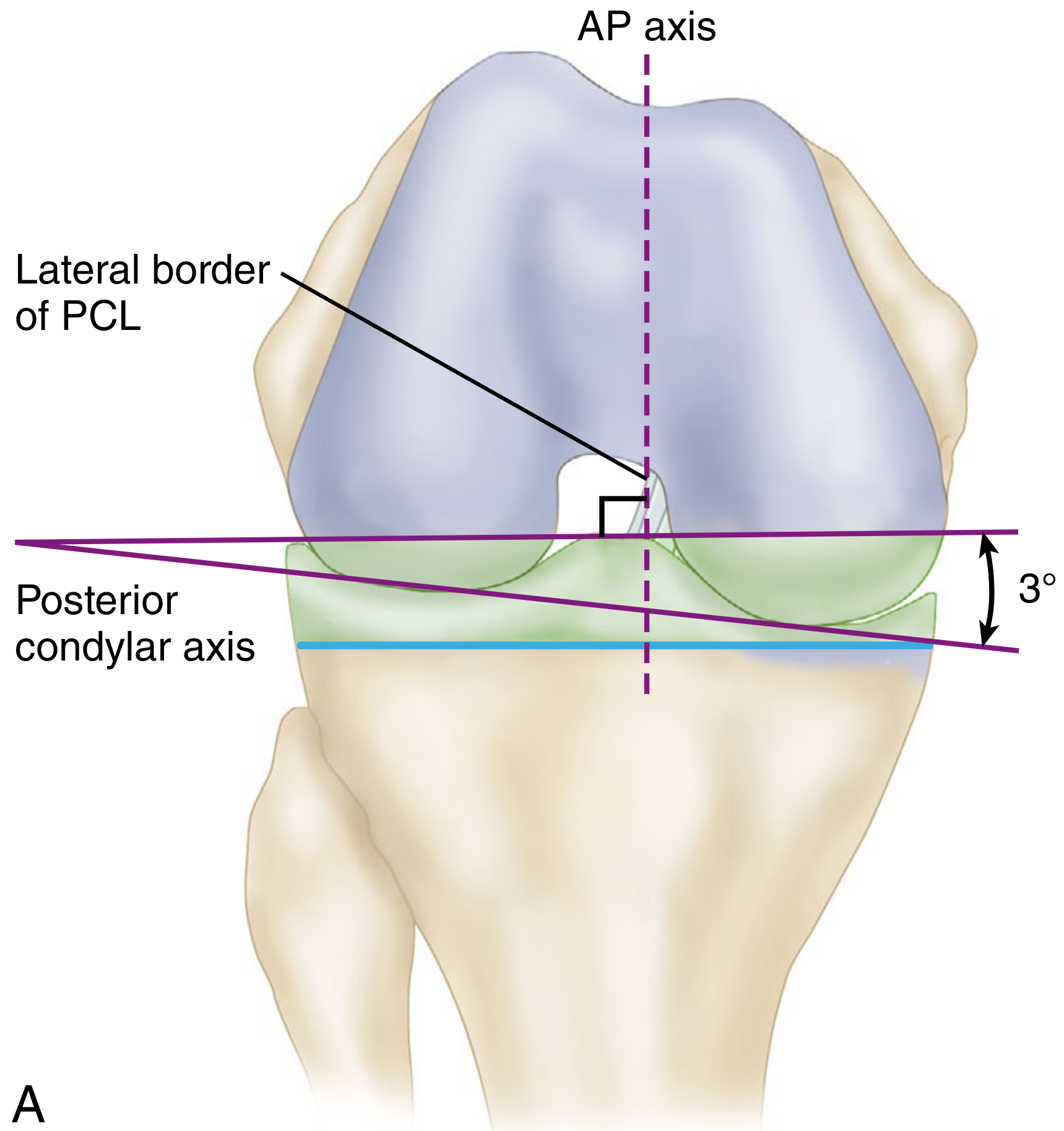
FIGURE: Posterior view showing the AP axis (perpendicular to tibial cut = 90°) and the relationship between the epicondylar axis and posterior condylar axis (3° difference). Lateral border of the PCL is also visible. - Campbell's Operative Orthopaedics 15th Ed, Fig. 8.17A
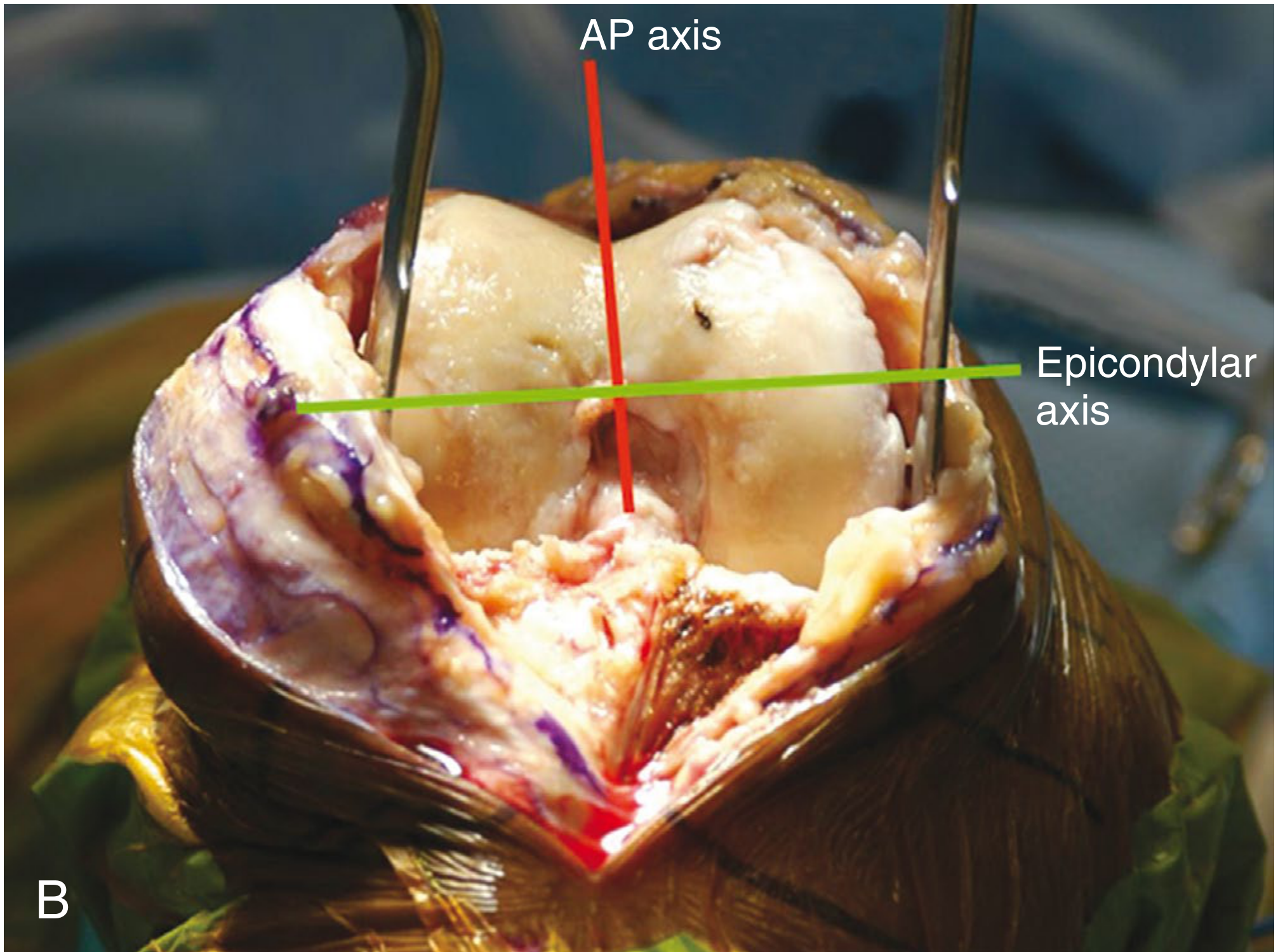
FIGURE: Intraoperative photo showing the AP axis (red line) and epicondylar axis (green line) identified on the flexed distal femur. - Campbell's Operative Orthopaedics 15th Ed, Fig. 8.17B
Method 1 - Transepicondylar Axis: Cut parallel to a line between the medial and lateral epicondyles. Most reliable, but can be difficult to identify intraoperatively.
Method 2 - AP Axis (Whiteside's Line): Cut perpendicular to this line. Useful when epicondyles are difficult to palpate.
Method 3 - Posterior Condylar Axis + 3° ER: Standard default method in most systems. Unreliable in valgus knees with hypoplastic lateral condyle - will produce internal rotation.
Method 4 - Gap balancing / proximal tibial cut reference: Posterior femoral cut made parallel to the tibial cut after soft-tissue balancing in extension. Often used for mobile-bearing (rotating platform) TKA.
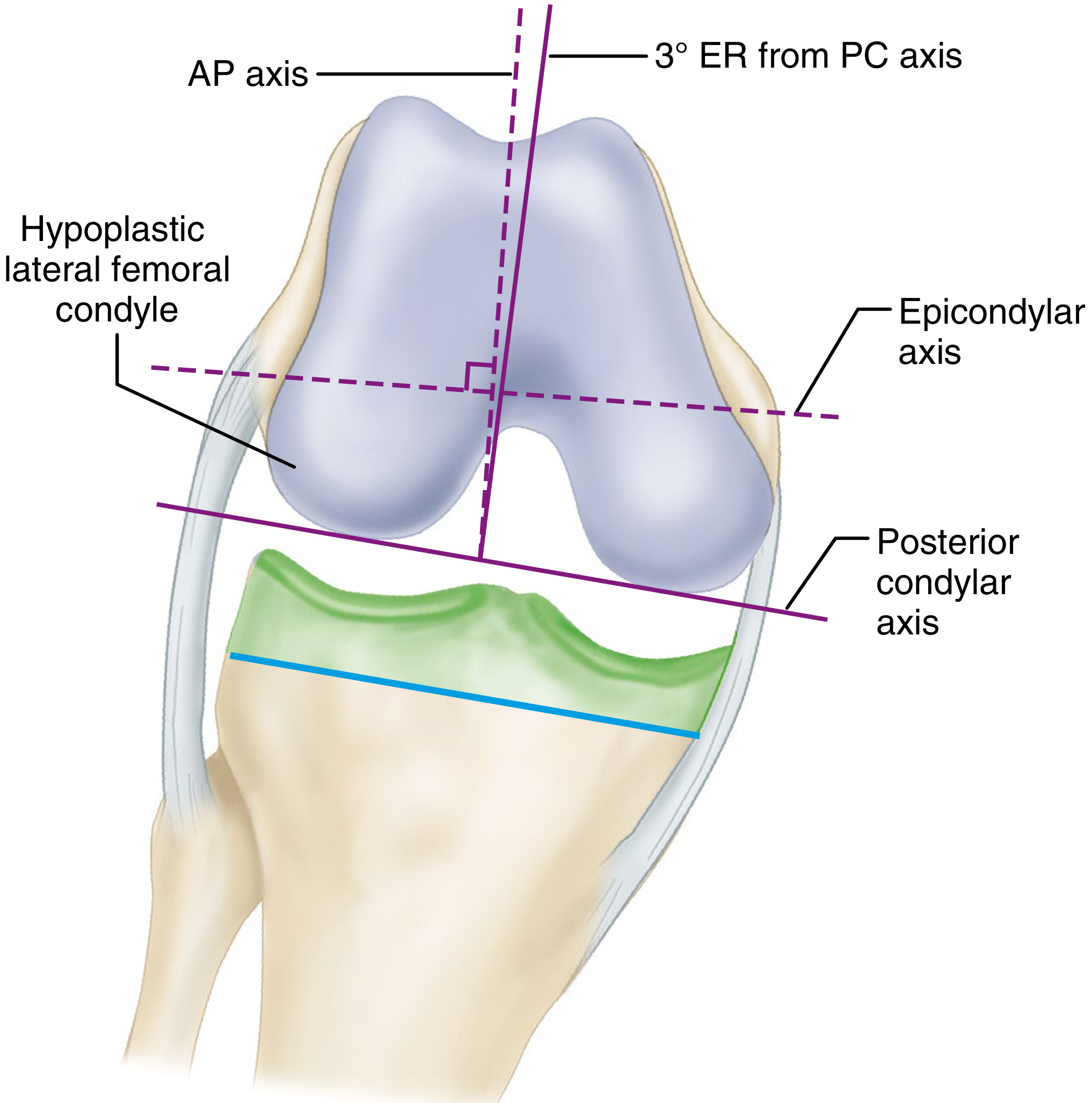
FIGURE: Hypoplastic lateral condyle - relying on posterior condylar axis alone internally rotates the femoral component, while the AP axis correctly guides external rotation (3° ER from PC axis). - Campbell's Operative Orthopaedics 15th Ed, Fig. 8.37
Key principle from Campbell's: "Knowledge of each of these techniques is necessary because arthritic deformity or previous surgery may obscure one or more of these landmarks. In revision TKA, the epicondylar axis usually is the only native landmark left to ensure proper femoral component rotation."
Anterior Referencing vs. Posterior Referencing
| Anterior Referencing | Posterior Referencing | |
|---|---|---|
| Reference point | Anterior femoral cortex | Posterior condylar surface |
| Advantage | Less risk of anterior cortex notching | More accurately recreates original distal femur dimensions |
| Disadvantage | May over-resect posteriorly (flexion tightness) | Risk of notching anterior cortex if component is too large |
| Component sizing | AP dimension of condyle from anterior cortex to posterior articular surface | Thickness of posterior condylar resection must equal posterior condyle of component |
Condylar Geometry - Key Asymmetries
- The medial femoral condyle is larger and extends more distally than the lateral
- The medial condyle has a more uniform sagittal radius of curvature; the lateral condyle's radius diminishes from extension to flexion (J-curve anatomy)
- The trochlear groove (patellar groove) runs anteroposteriorly in the distal femur - its deepest point is the anterior reference for the AP axis
- The intercondylar notch separates the condyles posteriorly and houses the cruciate ligaments - its lateral border marks the PCL origin
Practical Surgical Pearls (Campbell's Operative Orthopaedics, 15th Ed)
- Intramedullary femoral alignment is the standard for coronal alignment; entry point is ~1 cm anterior to the PCL femoral attachment, just medial to center of the intercondylar notch
- Proper distal valgus angle (5-7°) should be confirmed from a long-standing hip-to-knee radiograph - not assumed
- Kinematic alignment advocates a slightly increased distal valgus cut (>7°) with a 3° varus tibial joint line - a valid alternative but with higher failure rates when tibial varus outliers exceed 4°
- Rotational malalignment effects:
- Internal rotation → lateral patellar tilt, patellofemoral instability, asymmetric flexion gap
- Excessive external rotation → widens medial flexion gap, flexion instability
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Techniques 8.1 & 8.2, pp. 518-521
- Imaging Anatomy Text and Atlas Vol. 3, Chapter 21 - Distal Femur, pp. 751-758
This is a shared conversation. Sign in to Orris to start your own chat.