Vkc from basics to clinical
Reading File
Finding Sources
Finding Sources
Searching PubMed
vernal keratoconjunctivitis
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have all the material needed for a comprehensive, well-illustrated response on VKC. Let me compile it:
Vernal Keratoconjunctivitis (VKC) - From Basics to Clinical
1. Definition and Overview
Vernal keratoconjunctivitis (VKC) is a recurrent, bilateral, chronic allergic inflammation of the conjunctiva involving both IgE-mediated and cell-mediated (Type IV) immune mechanisms. The name "vernal" (Latin: spring) reflects its seasonal predilection, though perennial forms exist.
- Predominantly affects boys (M:F ratio ~3:1)
- Onset typically from age 5 years onward
- Spontaneous remission in ~95% by late teens; the remainder may transition to atopic keratoconjunctivitis (AKC)
- More prevalent in warm, dry climates: Mediterranean, sub-Saharan Africa, Middle East
- In temperate regions, >90% of patients have co-existing atopic disease (asthma, eczema) and two-thirds have a family history of atopy
(Kanski's Clinical Ophthalmology, 10th ed.)
2. Pathogenesis / Immunology
VKC is a mixed Th2-driven allergic response:
| Phase | Mechanism |
|---|---|
| Sensitization | Allergen exposure leads to IgE production, bound to mast cells on conjunctival surface |
| Early phase (minutes) | Re-exposure triggers mast cell degranulation → histamine, tryptase, prostaglandins → immediate itch, hyperemia |
| Late phase (hours) | Eosinophil, basophil, and T-lymphocyte recruitment; cytokine release (IL-4, IL-5, IL-13) |
| Chronic phase | Th2 cell activation, eosinophil accumulation, fibroblast activation → papillary hypertrophy and tissue remodeling |
Key mediators:
- Histamine - itch, vasodilation
- Eosinophil-derived toxins (MBP, ECP) - epithelial damage, Trantas dots
- IgE - immediate hypersensitivity
- Mast cell mediators - mucus hypersecretion, chemotaxis
- TGF-β, fibroblast growth factor - subepithelial fibrosis
3. Classification
VKC is classified into three forms based on anatomical involvement:
3a. Palpebral (Tarsal) VKC
- Primarily involves the upper tarsal conjunctiva
- More prone to corneal complications due to close mechanical contact between inflamed tarsal conjunctiva and corneal epithelium
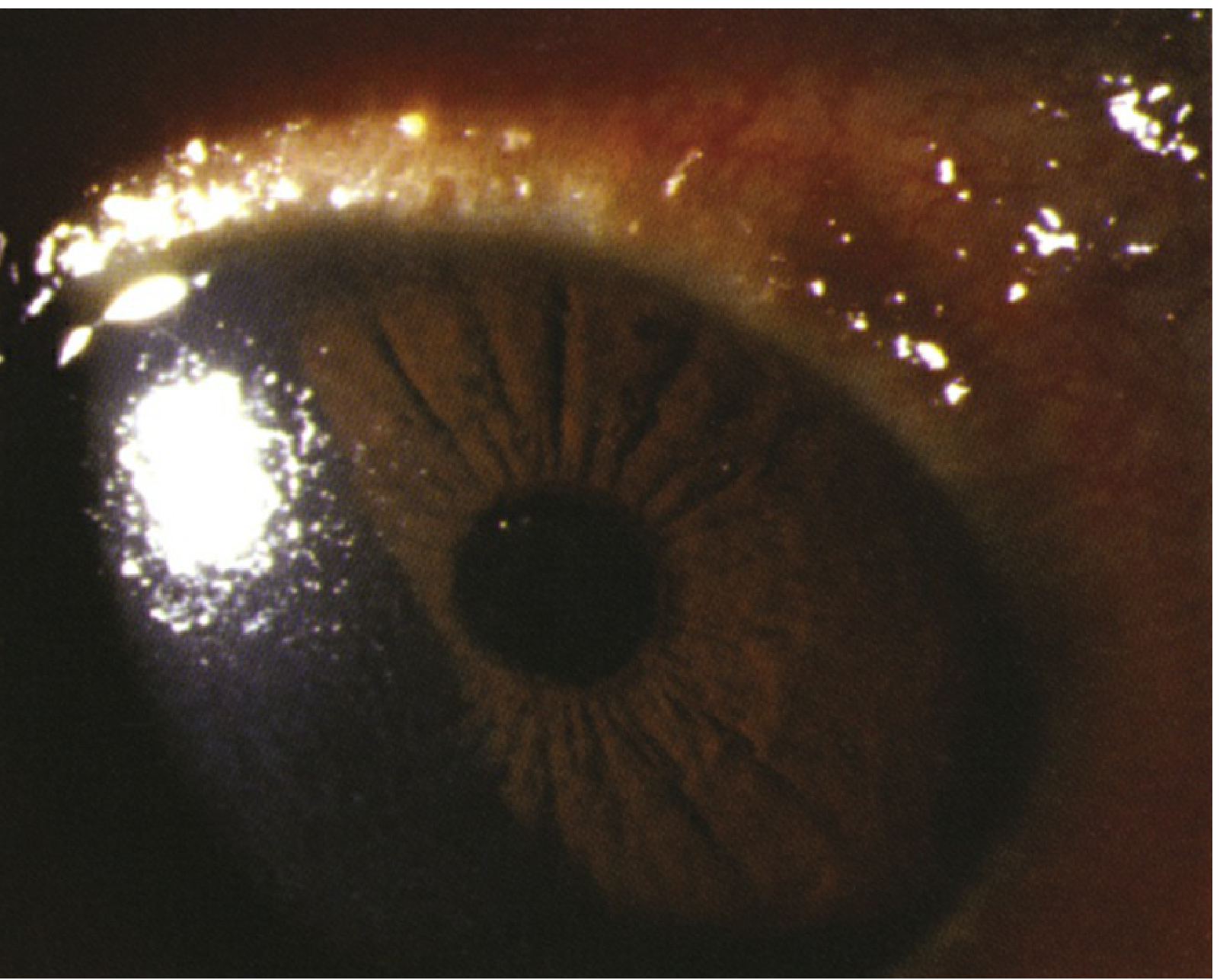
3b. Limbal VKC
- Affects the limbus (corneoscleral junction)
- Typically seen in Black and Asian patients
- Characterized by gelatinous limbal papillae with Horner-Trantas dots
3c. Mixed VKC
- Features of both palpebral and limbal forms
4. Clinical Features
Symptoms
- Intense itching - the cardinal symptom
- Lacrimation, photophobia, foreign body sensation, burning
- Thick, ropy/stringy mucoid discharge (characteristic)
- Increased blinking; nocturnal rubbing worsens disease
Signs - Palpebral Disease
Early/mild:
- Conjunctival hyperemia
- Diffuse velvety papillary hypertrophy on the superior tarsal plate
Macropapillae (<1 mm):
- Flat-topped, polygonal "cobblestone" appearance
- May have focal or diffuse whitish inflammatory infiltrates
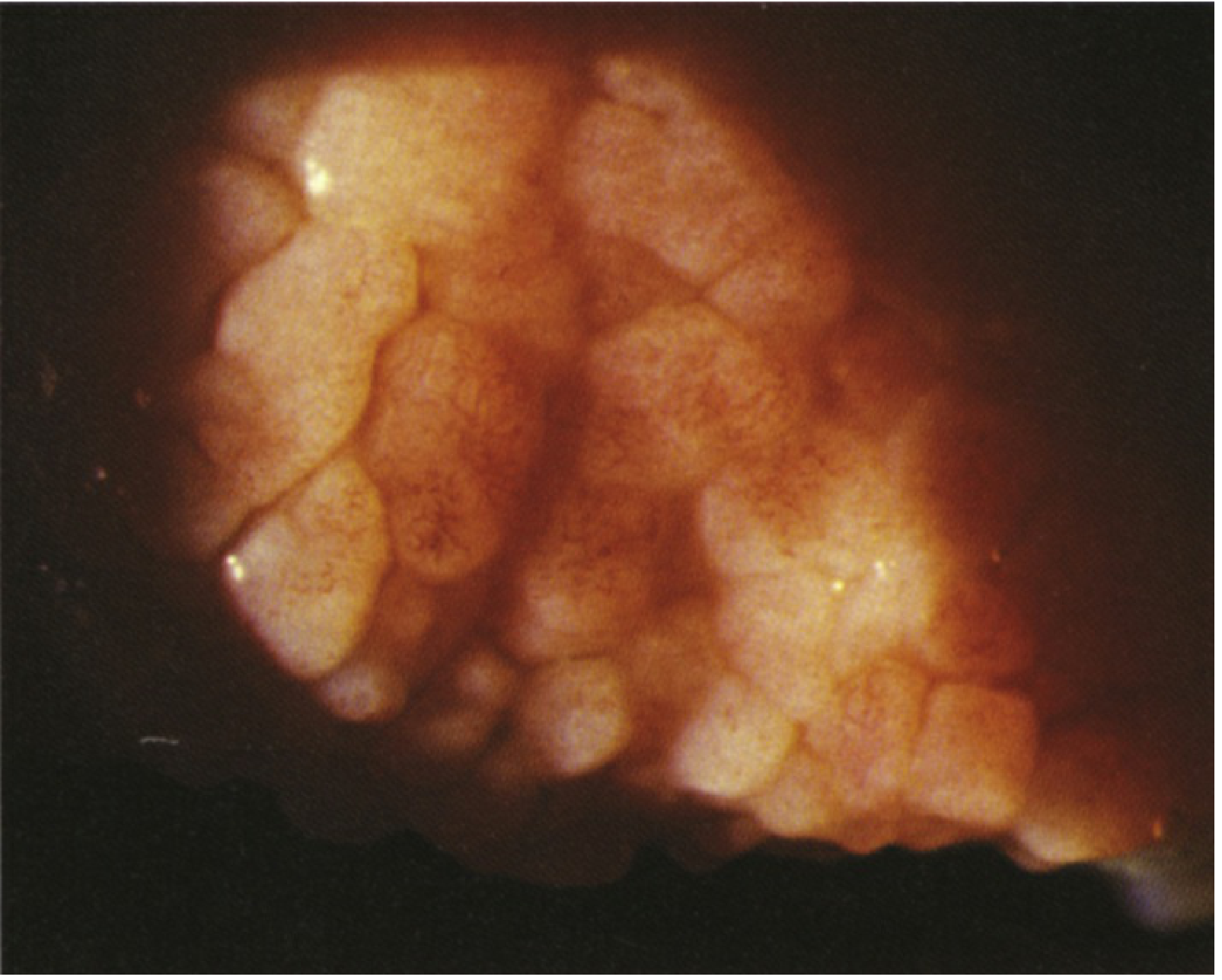
Giant papillae (>1 mm):
- Form when adjacent macropapillae coalesce as dividing septa rupture
- Mucus deposition between papillae is common in intense disease

Signs - Limbal Disease
- Gelatinous limbal papillae - raised, translucent swellings at the limbus
- Horner-Trantas dots - white/chalky dots at the apex of limbal papillae, composed of degenerated eosinophils and epithelial debris
5. Corneal Complications (Keratopathy)
Keratopathy is more frequent in palpebral VKC. Forms include:
| Complication | Description |
|---|---|
| Superficial punctate erosions (SPE) | Superior punctate epithelial erosions, often with mucus staining positive on rose Bengal |
| Epithelial macroerosions | Larger erosions from combined epithelial toxicity (inflammatory mediators) + mechanical trauma from papillae |
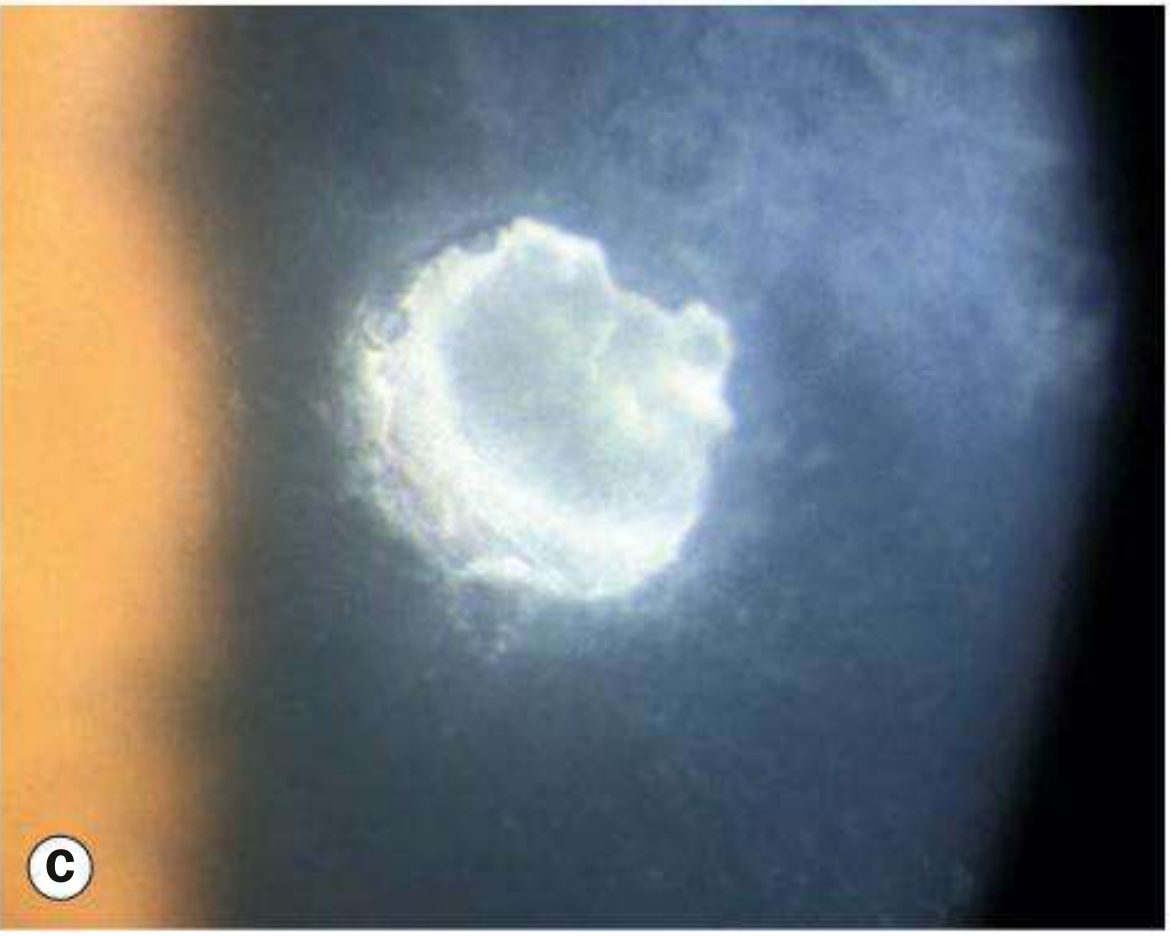
| Shield ulcer | Sterile, well-delineated, gray-white epithelial defect in the superior cornea - pathognomonic; caused by mechanical trauma + toxic mediators; does NOT involve stroma initially |
| Corneal plaque | Calcified mucous/protein deposit overlying shield ulcer; impedes re-epithelialization |
| Pseudogerontoxon | Arcus-like lipid deposition near the limbus, resembling gerontoxon (arcus senilis) |
Additional complications:
- Predisposition to secondary bacterial and fungal infections
- Aggressive herpes simplex keratitis (possibly steroid-related)
- Keratoconus - occurs in ~15% of VKC patients; thought to be secondary to chronic eye rubbing
- Presenile anterior or posterior subcapsular cataract (may be disease-related or steroid-induced)
- Retinal detachment risk is higher than the general population
6. Palpebral VKC vs Limbal VKC - Summary
| Feature | Palpebral VKC | Limbal VKC |
|---|---|---|
| Location | Upper tarsal conjunctiva | Corneoscleral limbus |
| Papillae | Cobblestone/giant | Gelatinous |
| Population | All ethnicities | Black, Asian |
| Corneal disease | More frequent | Less frequent |
| Trantas dots | No | Yes (pathognomonic) |
7. Diagnosis
VKC is a clinical diagnosis; investigations are usually not required.
Useful investigations:
- Conjunctival scraping - eosinophilia (eosinophils abundant) is confirmatory
- Tear IgE levels elevated
- Total serum IgE may be elevated
- Skin prick tests / allergen-specific IgE (RAST) - identify triggering allergens in atopic cases
Key diagnostic signs on slit-lamp exam:
- Giant papillae on eversion of upper lid (mandatory step)
- Horner-Trantas dots at limbus
- Shield ulcer / corneal plaque superiorly
- Thick ropy mucus in fornix
8. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Atopic keratoconjunctivitis (AKC) | Adults, perennial, periorbital eczema, worse in winter |
| Giant papillary conjunctivitis (GPC) | Contact lens wearers, exposed sutures |
| Allergic conjunctivitis (seasonal/perennial) | No giant papillae, no corneal involvement |
| Trachoma | Cicatrizing, upper lid follicles/scarring, pannus, Arlt's line |
| Superior limbic keratoconjunctivitis (SLK) | Hyperemia limited to superior bulbar conjunctiva, filamentary keratitis |
9. Treatment
General Measures
- Allergen avoidance where possible
- Cool compresses - symptomatic relief
- Avoid eye rubbing - reduces keratoconus risk
- Lid hygiene for associated staphylococcal blepharitis
- Bandage contact lens for persistent epithelial defects
Step-Up Pharmacological Approach
Step 1 - Mast Cell Stabilizers (First-line, prophylactic)
- Sodium cromoglicate, nedocromil, lodoxamide (most potent), pemirolast
- Require several days to weeks for effect; used prophylactically 2-3 weeks before season
- Lodoxamide 0.1% QID
- Seldom effective in isolation during acute flares
Step 2 - Dual-Action Antihistamine/Mast-Cell Stabilizers (Preferred for active disease)
- Olopatadine 0.1% BD or 0.2%/0.7% once daily
- Alcaftadine 0.25% once daily
- Ketotifen 0.1% BD
- Best for both prophylaxis and acute symptom control
Step 3 - Topical Steroids (For moderate-severe or acute exacerbations)
- Prednisolone acetate 1%, loteprednol 0.5%, dexamethasone 0.1%
- Use short courses only; always monitor IOP
- Steroid-induced glaucoma and cataract are significant risks with prolonged use
Step 4 - Immunomodulators (Steroid-sparing)
- Cyclosporin A 0.05-2% eyedrops 2-6x daily - effective when steroids are inadequate or poorly tolerated; takes weeks to work
- Verkazia (cyclosporin 0.1% cationic emulsion) - licensed specifically for VKC in children ≥4 years, QID
- Tacrolimus 0.1% ointment - effective for shield ulcers and eyelid disease; useful without steroids
Step 5 - Supratarsal Steroid Injection
- For severe palpebral disease or non-compliant patients
- 0.1 ml betamethasone/dexamethasone/triamcinolone injected under the upper eyelid via everted conjunctival surface
Systemic Treatment
- Oral antihistamines (e.g., loratadine - non-sedating; diphenhydramine - sedating, useful at night to reduce nocturnal rubbing)
- Aspirin has shown benefit in VKC - but avoid in children/adolescents due to Reye syndrome risk
- Doxycycline / azithromycin - for blepharitis-aggravated disease
- Immunosuppressives (cyclosporin, tacrolimus, azathioprine) for refractory cases
- Allergen desensitization
- Plasmapheresis in patients with extremely high serum IgE
Mucolytic Therapy
- Acetylcysteine eye drops - dissolves mucus filaments and deposits; useful for plaque prevention/management
10. Management of Shield Ulcer
Shield ulcer requires specific management:
- Topical steroid (prednisolone acetate 1% or loteprednol 0.5%) 4-6x/day
- Topical antibiotic (trimethoprim/polymyxin B QID) - prophylaxis against secondary infection
- Mast cell stabilizer/antihistamine continued
- Bandage contact lens if healing is delayed
- Acetylcysteine for mucous plaque
- Tacrolimus 0.1% ointment - effective alternative to steroids
- Surgical debridement (superficial keratectomy) if plaque prevents re-epithelialization
- Excimer laser phototherapeutic keratectomy (PTK) is an alternative
11. Surgical Options
- Superficial keratectomy - removes corneal plaques; debrides shield ulcers
- Excimer laser PTK - alternative to mechanical keratectomy
- Amniotic membrane overlay grafting - surface restoration
- Lamellar keratoplasty - for severe corneal scarring
- Botulinum toxin-induced ptosis - to reduce mechanical trauma from lid on cornea in refractory cases
12. Prognosis and Follow-up
- Spontaneous remission in ~95% by late teens - VKC is largely a self-limiting disease
- Remaining 5% may progress to AKC (perennial, more severe, adult)
- Corneal scarring from shield ulcers or plaques can cause permanent visual impairment
- Keratoconus risk (~15%) warrants periodic corneal topography
- If topical steroids used: monitor IOP every 4-6 weeks
- Follow-up: Every 2 weeks during acute flares; less frequent in remission
Quick Clinical Summary Card
| Feature | VKC |
|---|---|
| Age | Children/adolescents |
| Sex | Male > Female |
| Laterality | Bilateral |
| Season | Spring/summer (perennial in tropics) |
| Cardinal symptom | Intense itching |
| Discharge | Thick, ropy mucus |
| Key sign 1 | Giant cobblestone papillae (upper lid) |
| Key sign 2 | Horner-Trantas dots (limbus) |
| Corneal sign | Shield ulcer (superior) |
| Diagnosis | Clinical; conjunctival eosinophilia |
| First-line Rx | Mast cell stabilizer + dual antihistamine |
| Steroid-sparing | Cyclosporin A / Tacrolimus |
| Remission | ~95% by late teens |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | The Wills Eye Manual, 8th ed. | The Harriet Lane Handbook, 23rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.