65 yr old complaint knee pain no history
Reading File
Finding Sources
Finding Sources
Searching PubMed
knee pain elderly osteoarthritis management
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Here is a complete clinical approach to a 65-year-old with knee pain and no significant history:
Knee Pain in a 65-Year-Old - Clinical Approach
Most Likely Diagnosis: Osteoarthritis (OA)
Age 65 + knee pain with no prior trauma or systemic illness makes primary osteoarthritis the leading diagnosis. It is the most common musculoskeletal condition in this age group.
Differential Diagnosis
The first step is to determine whether the pain is articular vs. periarticular, and inflammatory vs. non-inflammatory.
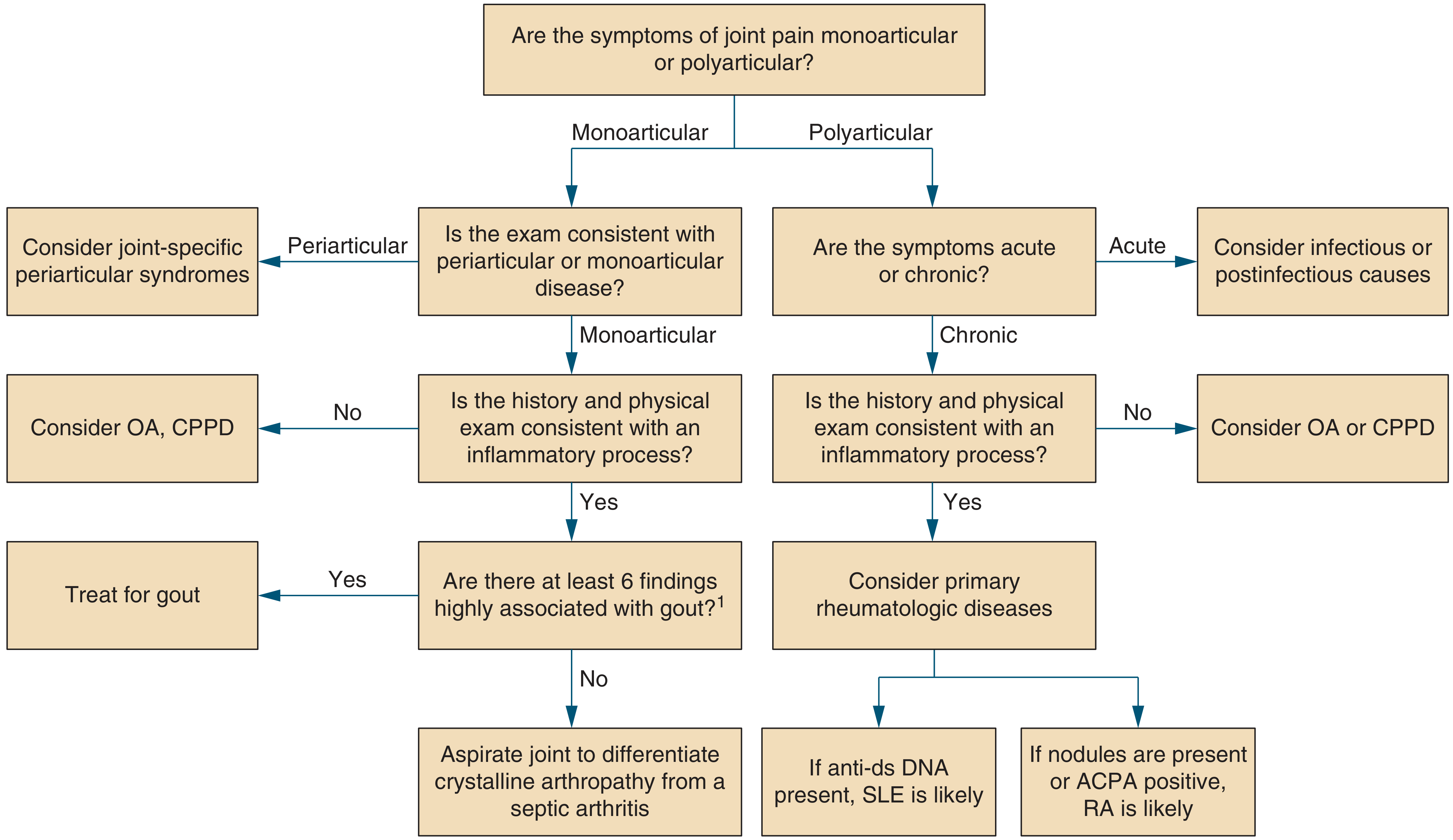
| Condition | Key Features |
|---|---|
| Osteoarthritis (most likely) | Gradual onset, worse with activity, crepitus, bony enlargement, no morning stiffness >30 min |
| CPPD / Pseudogout | Common in elderly knees, may cause acute flares, chondrocalcinosis on X-ray |
| Gout | Acute onset, severe, high uric acid, can affect knee |
| Septic arthritis | Must not miss - fever, hot/red/swollen joint, limited ROM, systemic signs |
| Rheumatoid arthritis | Bilateral, morning stiffness >1 hr, systemic features |
| Periarticular causes | Bursitis (pes anserine, prepatellar), tendinopathy, ligament injury |
| Meniscal tear | Pain at joint line, may lock or click |
| Referred pain | Hip OA commonly refers pain to the knee |
History to Elicit
- Onset - gradual (OA) vs. sudden (gout, septic, trauma)
- Character - aching, worse on stairs/standing (OA) vs. throbbing at rest (inflammatory/infective)
- Stiffness - brief morning stiffness <30 min (OA) vs. prolonged >1 hr (RA)
- Swelling - effusion vs. bony enlargement
- Locking/giving way - meniscal or ligamentous pathology
- Systemic features - fever, weight loss, rash (inflammatory/septic)
- Bilateral involvement - consider systemic disease
- BMI/obesity - major risk factor for OA
Physical Examination
- Gait - antalgic gait, varus/valgus deformity
- Inspection - effusion (bulge sign, patellar tap), swelling, erythema, muscle wasting
- Palpation - joint line tenderness (medial = OA/meniscus), warmth, bony enlargement (osteophytes)
- Range of motion - crepitus on flexion/extension (OA)
- Special tests:
- Valgus/varus stress test (ligament laxity)
- McMurray's/Apley's (meniscal tear)
- Patellar grind test (patellofemoral OA)
- Steinmann test (meniscal - pain on forced rotation at 90° flex)
Investigations
| Test | Purpose |
|---|---|
| X-ray knee (AP + lateral, weight-bearing) | First-line: joint space narrowing, osteophytes, subchondral sclerosis, chondrocalcinosis |
| CBC, ESR, CRP | Elevated in inflammatory/septic arthritis |
| Serum uric acid | Gout (note: may be normal during acute attack) |
| RF, anti-CCP | If RA suspected |
| Joint aspiration | If septic arthritis or crystal disease suspected - synovial fluid analysis (WBC count, crystals, culture) |
| MRI | If meniscal tear, ligament injury, or osteonecrosis suspected |
X-ray OA findings: joint space narrowing, osteophytes, subchondral sclerosis, subchondral cysts.
Management of Knee OA (Most Likely Diagnosis)
Non-Pharmacological (First Line - Strong Evidence)
- Physical activity and strengthening exercises (quadriceps strengthening)
- Low-impact aerobic exercise (swimming, cycling)
- Weight loss if BMI >25 - slows disease progression
- Ambulatory aids (cane in contralateral hand)
- Physiotherapy
Per AAOS guidelines, the following have strong evidence: physical activity, low-impact aerobics, and NSAIDs. (Campbell's Operative Orthopaedics, 15th Ed 2026)
Pharmacological
- NSAIDs (oral or topical) - strong evidence; use with gastroprotection (PPI) in elderly
- Paracetamol/Acetaminophen - modest effect
- Intra-articular corticosteroids - for acute flares with effusion
- Intra-articular hyaluronic acid - inconclusive/evidence against per AAOS
- Glucosamine/chondroitin - evidence against per AAOS
- Avoid opioids if possible in elderly (falls risk)
Surgical (When Nonoperative Fails)
- High tibial osteotomy - younger patients with unicompartmental disease + malalignment
- Unicompartmental knee arthroplasty - single compartment disease
- Total knee arthroplasty (TKA) - definitive; patients >70 yrs are 5x more likely to need TKA within 1 year of debridement than those <60
- Arthroscopic debridement - not recommended by AAOS for OA; short-duration placebo effect only
Cautions in the Elderly
- Use NSAIDs with caution (GI, renal, cardiovascular risks)
- Avoid opioids as first-line (falls, cognitive effects)
- Screen for comorbidities (HTN, CKD, peptic ulcer disease) before prescribing
Red Flags - Do Not Miss Septic Arthritis
If the knee is hot, red, swollen, and the patient has fever or systemic signs - aspirate the joint immediately. Septic arthritis is a joint emergency that leads to rapid cartilage destruction if untreated. Synovial WBC >50,000/mm³ strongly suggests infection.
Summary
In a 65-year-old with knee pain and no history, osteoarthritis is the most likely diagnosis. Start with weight-bearing X-rays and a thorough history/exam to rule out inflammatory, crystal, or infective causes. First-line management is exercise, weight loss, and NSAIDs (with gastroprotection). Reserve surgery for cases failing 3-6 months of conservative therapy.
Recent evidence note: A 2024 Cochrane systematic review (PMID 39625083) confirms that exercise is beneficial for knee OA, supporting it as a cornerstone of management.
This is a shared conversation. Sign in to Orris to start your own chat.