Painful arc syndrome etiology pathologenesis signs and symptoms and investigations and evaluation treatment explain in detail with appropriate images illustrations and diagrams
Reading File
Finding Sources
Finding Sources
Searching the Web
painful arc syndrome shoulder etiology pathogenesis signs symptoms investigations treatment
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
I now have all the material needed for a comprehensive, well-illustrated answer. Here it is:
Painful Arc Syndrome (Subacromial Impingement Syndrome)
Painful arc syndrome is the term used specifically for the clinical finding - and the underlying condition responsible for it - where shoulder abduction is painful only through the mid-range (60°-120°), with the extremes of motion being relatively pain-free. It is a subset of subacromial impingement syndrome, which is the most common cause of shoulder pain, accounting for 44-65% of all shoulder complaints.
1. ANATOMY - The Subacromial Space
Understanding the syndrome requires first appreciating the tight corridor through which the rotator cuff must glide.
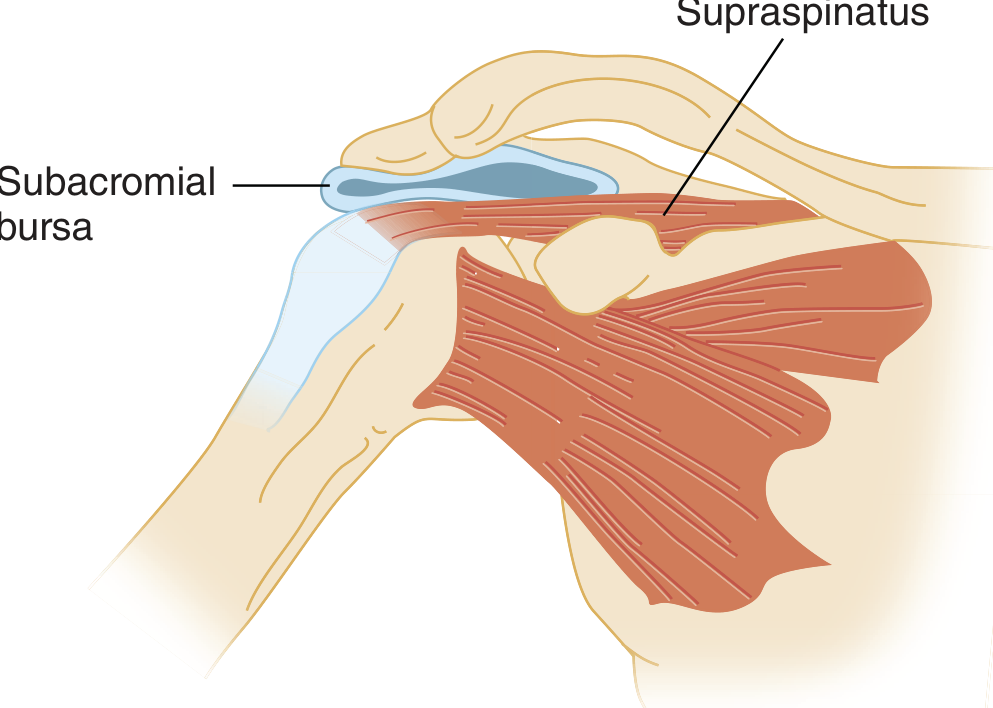
The coracoacromial arch forms the roof of this space and is made up of:
- The acromion process (especially its anterior inferior surface)
- The coracoacromial ligament
- The coracoid process
- The acromioclavicular (AC) joint below
The floor is provided by the humeral head and greater tuberosity. Within this space lie:
- The four rotator cuff tendons (supraspinatus, infraspinatus, teres minor, subscapularis)
- The long head of biceps tendon
- The subacromial/subdeltoid bursa
2. ETIOLOGY
The etiology is best understood as a combination of extrinsic compression and intrinsic degeneration (Miller's Review of Orthopaedics).
Extrinsic (Primary) Causes - Structural narrowing of the subacromial space
| Factor | Details |
|---|---|
| Acromion morphology | Type I (flat) - lowest risk; Type II (curved) - moderate; Type III (hooked) - highest risk for impingement |
| Acromial spur | Osteophyte on anterior acromion reduces subacromial space |
| AC joint hypertrophy | Inferior osteophytes from AC OA narrow the space |
| Coracoacromial ligament thickening | Calcification or hypertrophy of the ligament |
| Os acromiale | Failure of acromial ossification centers to fuse |
| Calcific tendinitis | Calcium hydroxyapatite deposits within the supraspinatus tendon |
Intrinsic (Secondary) Causes - Rotator cuff dysfunction
| Factor | Details |
|---|---|
| Rotator cuff weakness | Weakened cuff fails to depress the humeral head during abduction, causing superior migration into the arch |
| Repetitive overhead activity | Athletes (swimmers, tennis, baseball), laborers, painters |
| Glenohumeral instability | Increased superior translation of the humeral head narrows the space |
| Scapular dyskinesis | Poor scapular upward rotation reduces arch clearance |
| Biceps tendon pathology | Thickening adds to space competition |
| Intrinsic tendon degeneration | Avascular zone of supraspinatus ("critical zone") undergoes mucoid degeneration, disorganized collagen, and eventual tearing |
Risk factors
- Age >40 years (degenerative change)
- Dominant arm affected
- Workers' compensation populations (poor outcomes)
- Overhead sport athletes at any age
3. PATHOGENESIS - Neer's Three Stage Model
The condition follows a progressive three-stage continuum of subacromial space injury (Tintinalli's Emergency Medicine):
Stage I - Edema and Hemorrhage (Age <25 years)
- Reversible edema and hemorrhage around the rotator cuff tendons and bursa
- Caused by excessive overhead use (e.g., competitive swimming, pitching)
- Reversible with rest and activity modification
- Symptoms: dull ache over anterolateral shoulder, worse with activity, improved by rest
Stage II - Fibrosis and Tendinitis (Age 25-40 years)
- Repeated mechanical trauma leads to tendinitis of the rotator cuff
- Fibrosis and thickening of the tendons and bursa develop
- Chronic and recurrent course, often lasting weeks to months
- Night pain becomes prominent (due to relaxation of supporting muscle tone)
- Partially reversible; may require more aggressive treatment
Stage III - Rotator Cuff Tears and Bony Changes (Age >40 years)
- Continued overuse leads to:
- Partial or full-thickness rotator cuff tears (typically supraspinatus first)
- Rupture of the long head of biceps tendon
- Subacromial bone spurs (osteophytes on anterior acromion)
- Progressive and largely irreversible without surgery
- Significant disability and functional limitation
Histologically: Tendinopathy is characterized by disorganized collagen fibers and mucoid degeneration. Importantly, inflammatory cells are typically absent - making "tendinitis" somewhat of a misnomer; "tendinopathy" is the preferred modern term.
4. SIGNS AND SYMPTOMS
Symptoms
Pain is the primary symptom, developing insidiously over weeks to months:
- Located over the anterior to lateral shoulder
- Frequently radiates to the lateral mid-humerus (not below the elbow - differentiates from cervical radiculopathy)
- Night pain - deep, aching, worsened by lying on the affected shoulder or sleeping with arms overhead
- Aggravated by overhead activities - brushing hair, reaching into cupboards, throwing
- Associated weakness and stiffness (usually secondary to pain)
Signs
The Painful Arc - the hallmark sign:
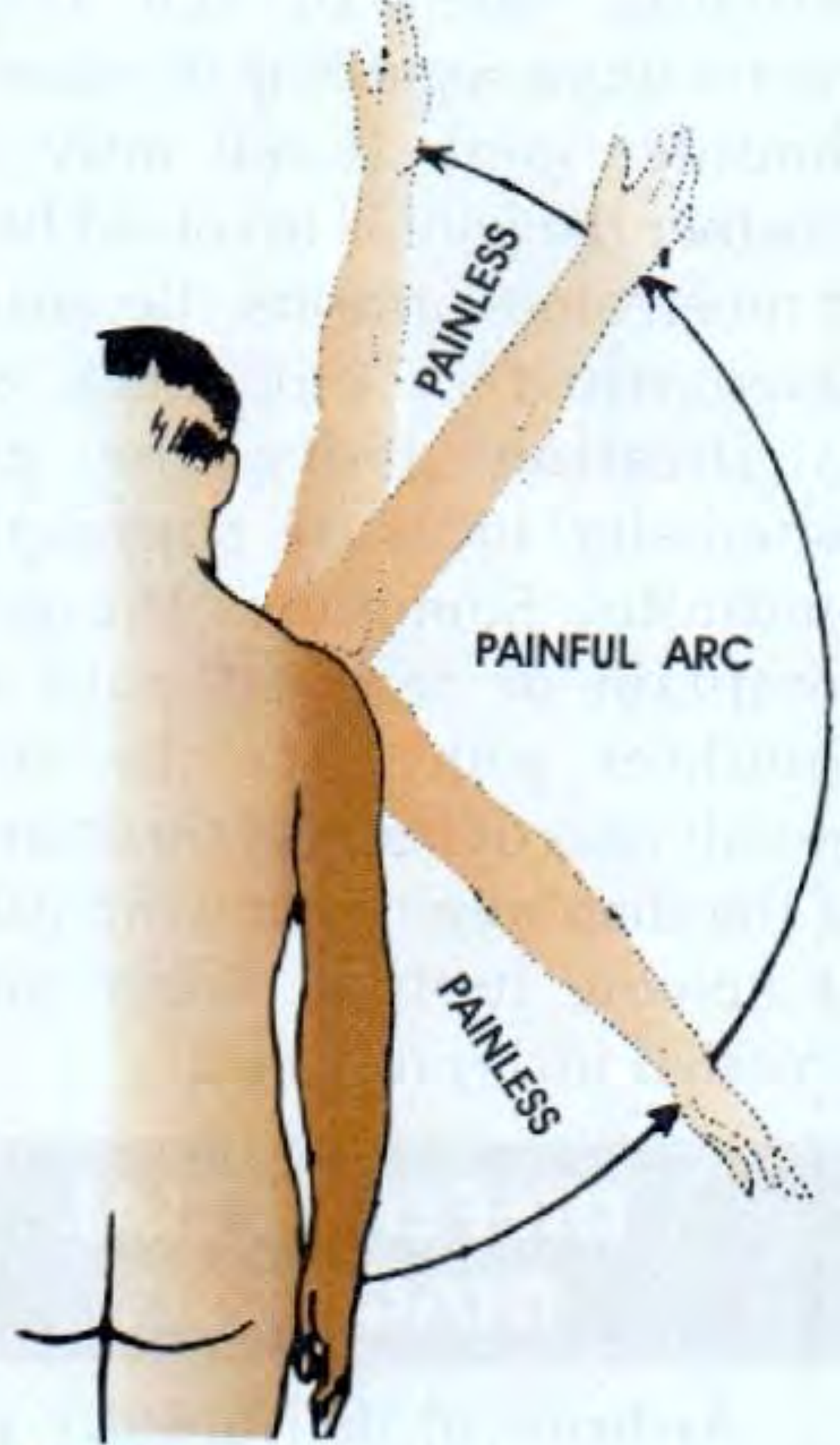
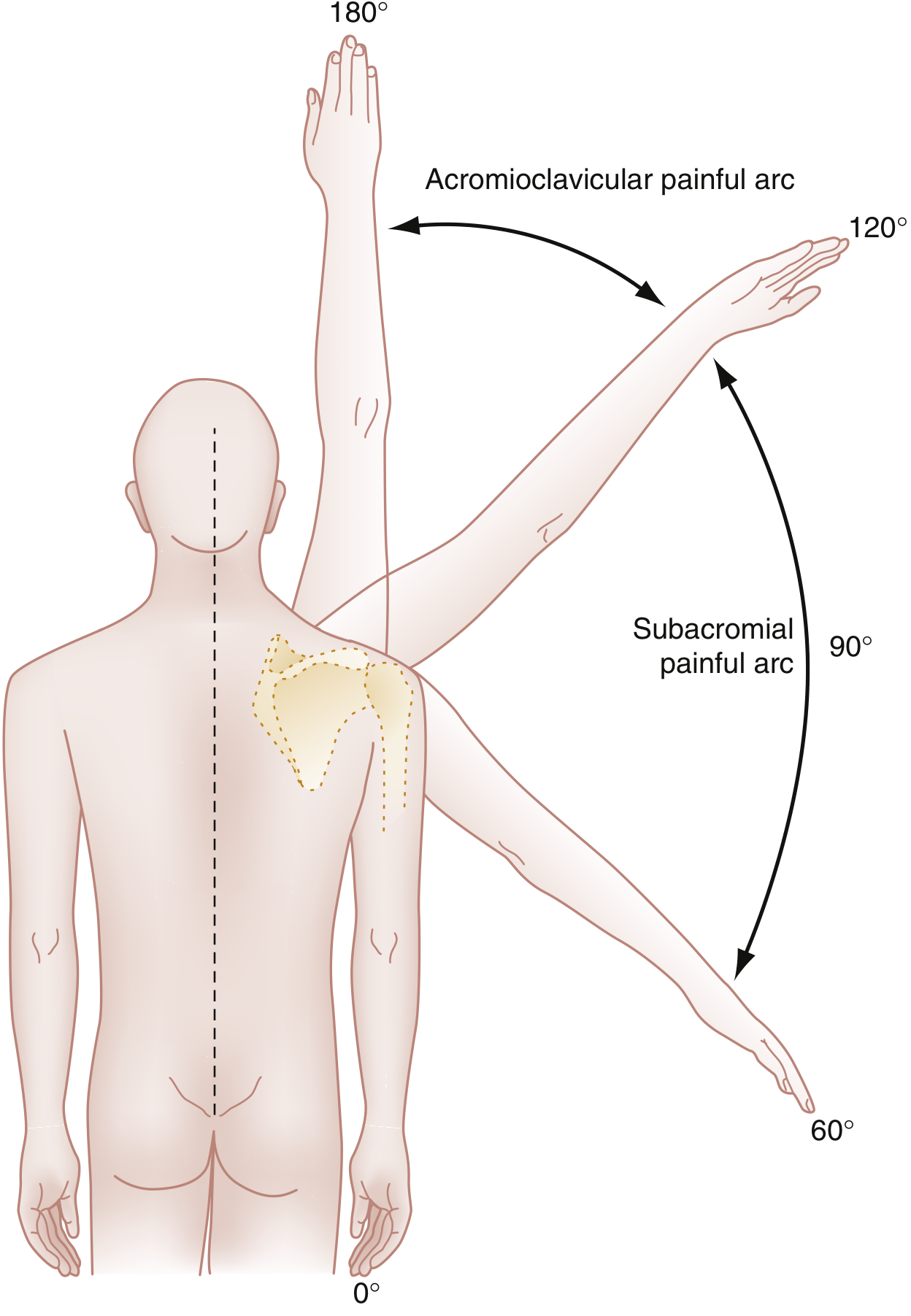

Key distinction by arc location:
- Subacromial painful arc: 60°-120° - Pathology in supraspinatus tendon/subacromial bursa
- AC joint painful arc: 120°-180° - Pathology in acromioclavicular joint
Palpation findings (S. Das Clinical Surgery):
- Tenderness just below the acromion process when the arm is adducted
- The tender spot disappears under the acromion when the arm is abducted (the tendon slips underneath the acromion) - this is a characteristic finding of painful arc syndrome specifically
Other clinical findings:
- Disuse atrophy of shoulder musculature in chronic stages
- Crepitus during range of motion (from fibrosis/scarring trapped under acromion)
- Normal or near-normal passive ROM (differentiates from frozen shoulder which has restricted passive ROM)
- Mild to moderate weakness of abduction and external rotation (supraspinatus, infraspinatus) - secondary to pain
- A "catching" sensation if scar tissue is trapped beneath the acromion
5. INVESTIGATIONS AND EVALUATION
Clinical Examination Tests
Neer Impingement Sign
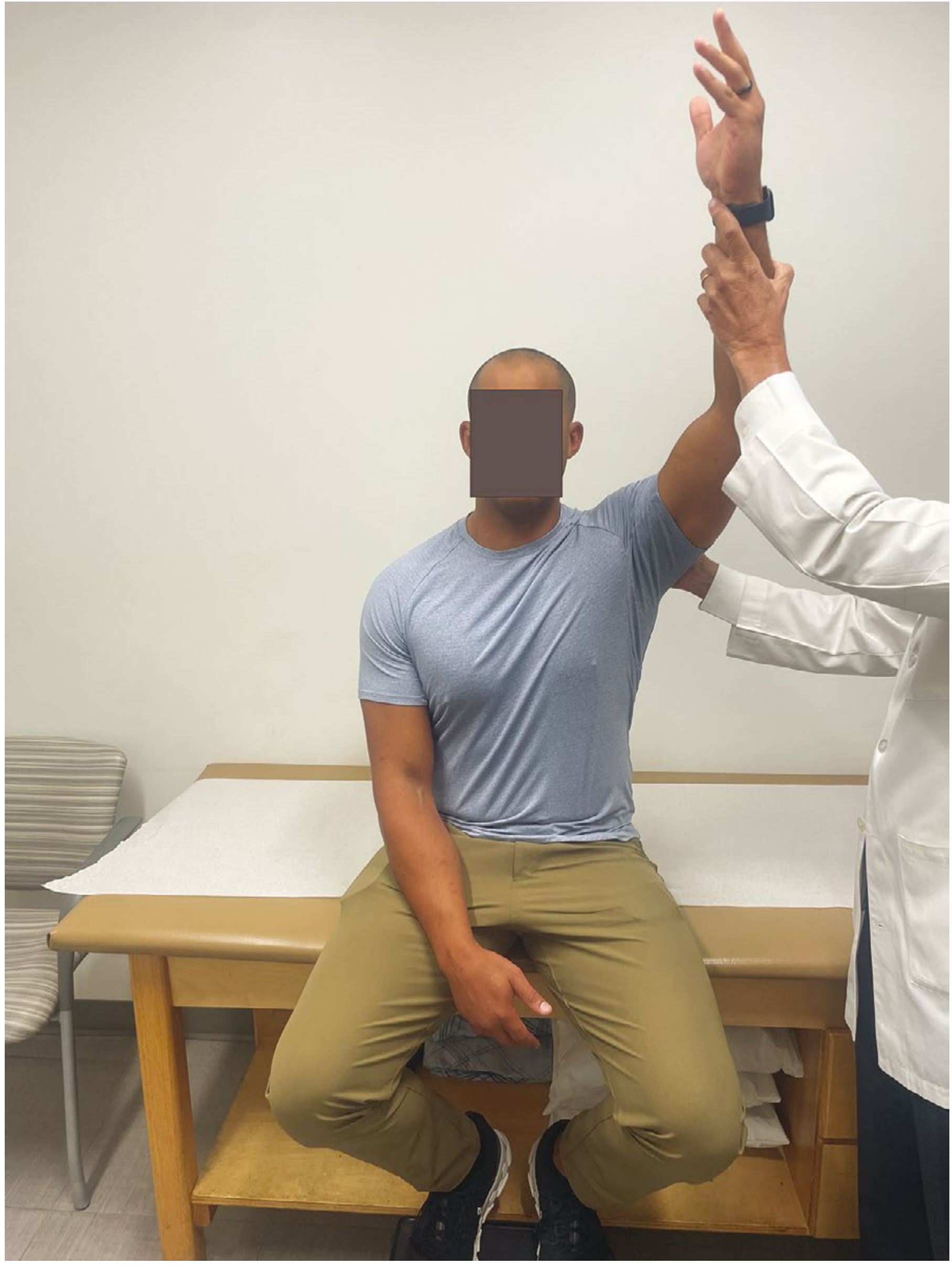
- Examiner prevents scapular rotation with one hand, then raises the patient's straightened arm in forward elevation
- Positive if pain occurs between 70°-120° (greater tuberosity impinges under the acromion)
- Sensitivity: 68%, Specificity: 68.7%
Hawkins-Kennedy Test

- Shoulder at 90° abduction, 90° elbow flexion; examiner internally rotates the shoulder
- This drives the supraspinatus tendon against the coracoacromial ligament
- Sensitivity: 71.5-80%, Specificity: 60-66%
Empty Can Test (Jobe Test)

- Arm at 90° abduction, 30° forward flexion, thumb pointing down ("empty can" position)
- Pain or weakness against resistance suggests supraspinatus injury
- Sensitivity: 44%, Specificity: 89.5%
Clinical Test Accuracy Table (Campbell's Operative Orthopaedics 2026)
| Test | Sensitivity | Specificity | PPV | NPV | Overall Accuracy |
|---|---|---|---|---|---|
| Painful arc sign | 73.5% | 81.1% | 88.2% | 61.5% | 76.1% |
| Hawkins-Kennedy sign | 71.5% | 66.3% | 79.7% | 55.7% | 69.7% |
| Neer sign | 68% | 68.7% | 80.4% | 53.2% | 68.3% |
| Jobe (supraspinatus) test | 44.1% | 89.5% | 88.4% | 46.8% | 60.2% |
| Drop-arm test | 26.9% | 88.4% | 81% | - | - |
Important: If Hawkins-Kennedy sign + painful arc sign + infraspinatus/Jobe test are ALL positive, likelihood of impingement is >95% (Campbell's).
Imaging
Plain X-rays (AP, axillary, outlet/supraspinatus outlet views):
- First-line imaging; usually normal in early stages
- May show:
- Hooked (Type III) acromion on outlet view
- Subacromial spur on anterior acromion
- Sclerosis and subchondral cyst formation of the greater tuberosity
- Calcification above the greater tuberosity (calcific tendinitis)
- Superior migration of the humeral head (suggests chronic large rotator cuff tear - normal AHI is >7mm)
- AC joint osteophytes
Ultrasound (US/POCUS):
- Dynamic, real-time assessment of the rotator cuff
- Shows: thickening of supraspinatus tendon, subacromial bursa fluid/thickening, partial or full-thickness tendon tears
- Operator-dependent but cost-effective
- First-line modality in many centers for soft tissue evaluation
MRI - Gold standard for soft tissue:
- Best delineates extent of tendon disease: tendinopathy vs. partial tear vs. full-thickness tear
- Shows subacromial bursal thickening/fluid
- Demonstrates fatty atrophy of cuff muscles in chronic disease
- Not necessary in acute/early presentation; reserved for surgical planning or when conservative treatment fails
CT/CT-arthrography:
- Useful for bony anatomy assessment (acromion morphology, spurring)
- CT arthrography accurately identifies full-thickness tears
- Less commonly used than MRI for primary evaluation
Blood tests:
- Not diagnostic but used to rule out systemic causes
- FBC, ESR, CRP, uric acid, rheumatoid factor - if inflammatory arthropathy, infection, or gout suspected
6. TREATMENT
Treatment follows a step-up approach, beginning conservatively and escalating to surgery only if conservative management fails after 3-6 months.
Conservative (Non-Operative) Management - First Line
Phase 1 - Acute Phase (Rest and Pain Control):
-
Relative rest and activity modification
- Avoid overhead activities and the painful arc of elevation
- A brief sling may help, but complete immobilization should be avoided (risk of adhesive capsulitis)
-
Analgesics and Anti-inflammatories
- NSAIDs for 7-21 days (mainstay)
- Paracetamol/acetaminophen for milder pain
- Short-term opioid analgesics if severe (3 days only)
-
Cryotherapy
- Ice applied to affected shoulder 10-15 minutes, 3-4 times daily
- Analgesia and reduction of inflammation/edema
-
Range-of-motion exercises (3-4 times daily)
- Pendulum swings: patient slightly bent at waist, arm hanging freely, gentle clockwise and counterclockwise arcs - progressing in size as symptoms allow
- Wall walking: stand sideways arm's length from wall, walk fingers upward to pain tolerance
Phase 2 - Recovery Phase (Stretching and Strengthening):
-
Physical Therapy (supervised)
- Rotator cuff strengthening (particularly supraspinatus, infraspinatus)
- Scapular stabilization exercises
- Postural correction and biomechanical retraining
- Evidence supports exercise therapy as first-line for all patients
-
Subacromial Corticosteroid Injection

- Indicated when pain persists despite rest, NSAIDs, and PT
- Reduces pain and allows better engagement with physical therapy
- Approach: lateral (most common) or posterior route below the acromion
- Agent: methylprednisolone or triamcinolone + local anesthetic (lidocaine)
- Adverse effects: local skin atrophy, tendon weakening, infection risk; direct tendon injection can cause necrosis/rupture
- Limit to 2-3 injections; diminishing returns thereafter
- Platelet-Rich Plasma (PRP) / Prolotherapy:
- Emerging evidence; not yet standard of care
Surgical Management - After 4-6 Months of Failed Conservative Treatment
Subacromial Decompression and Acromioplasty:
- Most common surgical procedure
- Arthroscopic approach is now standard (vs. open)
- Involves:
- Bursectomy - removal of thickened subacromial bursa
- Acromioplasty - resection of the anterior acromion to create a flat Type I profile
- Coracoacromial ligament release
- If needed: rotator cuff repair, distal clavicle resection (for AC joint OA)
Post-operative notes (Bailey & Love's Surgery):
- Surgery restores a flat acromion and creates more room for rotator cuff gliding
- However, evidence does not clearly show surgery improves long-term outcomes versus physical therapy alone
- Poor prognostic factors: workers' compensation claims, chronic symptoms, significant fatty muscle atrophy
Indications for surgery:
- Failure of minimum 4-6 months of non-operative treatment
- Stage III disease with full-thickness rotator cuff tear often requiring repair
- Exception: massive irreparable tears may benefit from debridement with preservation of the coracoacromial arch (to prevent anterosuperior humeral migration)
Treatment Summary Algorithm
Painful Arc Syndrome
|
v
Conservative (0-6 months)
- Rest, NSAIDs, ice
- ROM exercises
- Physical therapy (rotator cuff + scapular strengthening)
|
Not improving at 6-8 weeks?
|
v
Subacromial Corticosteroid Injection
+ Continued PT
|
Not improving at 3-6 months total?
|
v
MRI / Advanced Imaging
to characterize rotator cuff
|
v
Surgical: Arthroscopic Acromioplasty
+/- Rotator Cuff Repair
7. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Frozen shoulder (adhesive capsulitis) | Restricted passive ROM (external rotation especially); no painful arc |
| AC joint arthropathy | Pain at 120°-180° abduction (not 60°-120°); tenderness directly over AC joint |
| Rotator cuff complete tear | Weakness that persists after lidocaine injection; inability to maintain arm at 90° (drop-arm sign) |
| Calcific tendinitis | Often more acute onset; calcification visible on plain X-ray |
| Cervical radiculopathy | Pain radiates below the elbow; neurological signs; Spurling test positive |
| Glenohumeral OA | Reduced passive AND active ROM; bony end-feel; radiographic changes |
| Biceps tendinopathy | Tenderness over the bicipital groove; Speed's test positive |
Key Teaching Points
- Painful arc = subacromial pathology (60°-120°) - this is the defining clinical hallmark
- The syndrome encompasses subacromial bursitis, supraspinatus tendinitis, and biceps tendon involvement - these are not separate diagnoses
- Histologically, it is tendinopathy (collagen disorganization), not true inflammation
- The combination of painful arc sign + Hawkins-Kennedy + Jobe test gives >95% likelihood of impingement if all three are positive
- Conservative management works in 60-90% of patients when pursued for 3-6 months
- Workers' compensation status is an independent predictor of poor surgical outcome
Sources: Tintinalli's Emergency Medicine (Comprehensive Study Guide), Miller's Review of Orthopaedics 9th Ed, Bailey and Love's Short Practice of Surgery 28th Ed, Campbell's Operative Orthopaedics 15th Ed 2026, S. Das Manual on Clinical Surgery 13th Ed, Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.