RAE tube in anesthesia
Reading File
Finding Sources
Finding Sources
Searching the Web
RAE tube anesthesia endotracheal tube types uses
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
RAE tube oral nasal preformed endotracheal anesthesia
Loading Image
Reading File
Here is a comprehensive overview of the RAE tube in anesthesia, sourced from major anesthesia textbooks:
RAE Tube (Ring-Adair-Elwyn Tube)
What Is It?
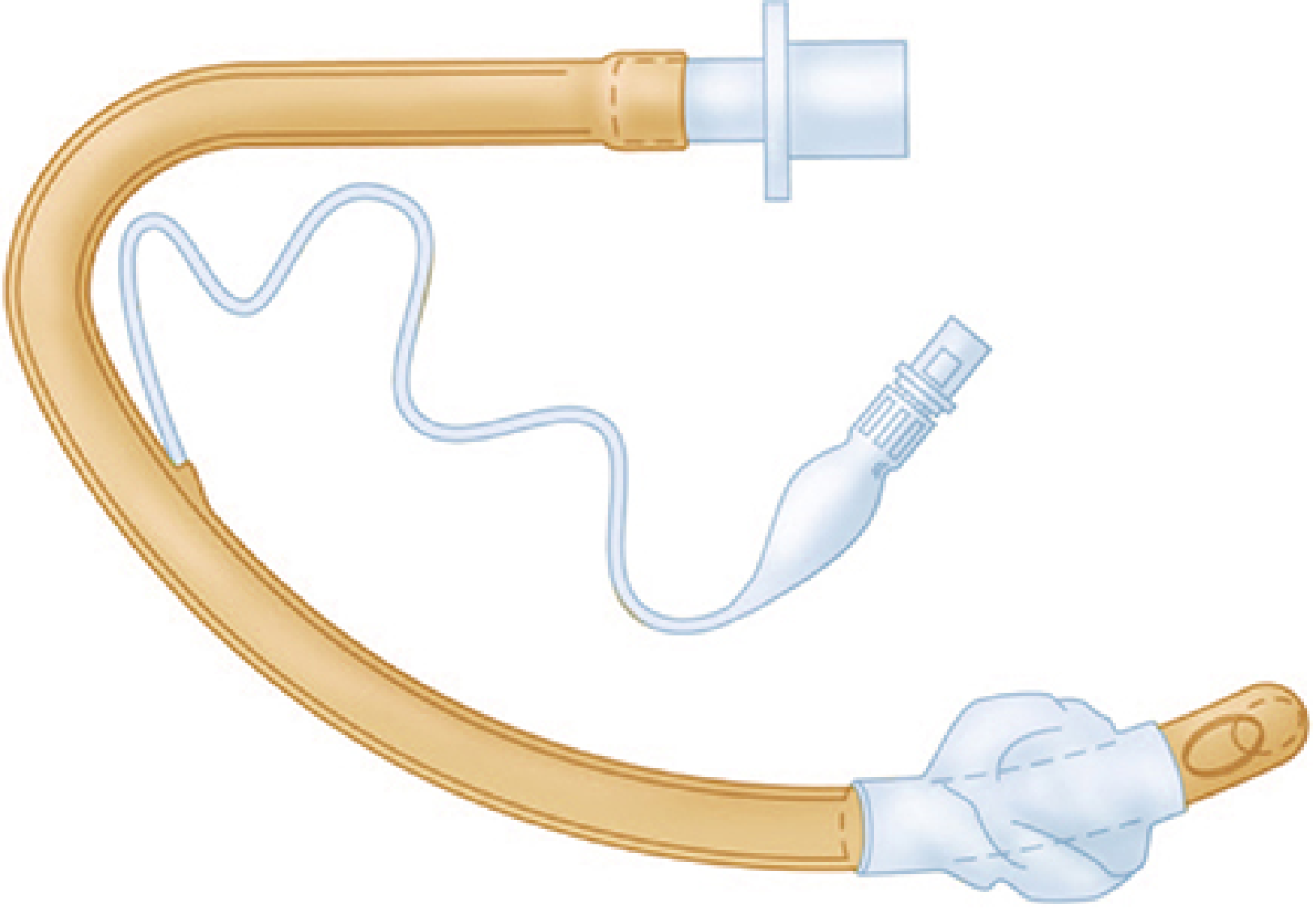
The RAE tube is a preformed, right-angle-bend endotracheal tube named after its inventors Ring, Adair, and Elwyn. It is made from clear polyvinyl chloride (PVC) and has a fixed contour designed to keep the proximal end of the tube and the breathing circuit away from the surgical field.
Two variants exist:
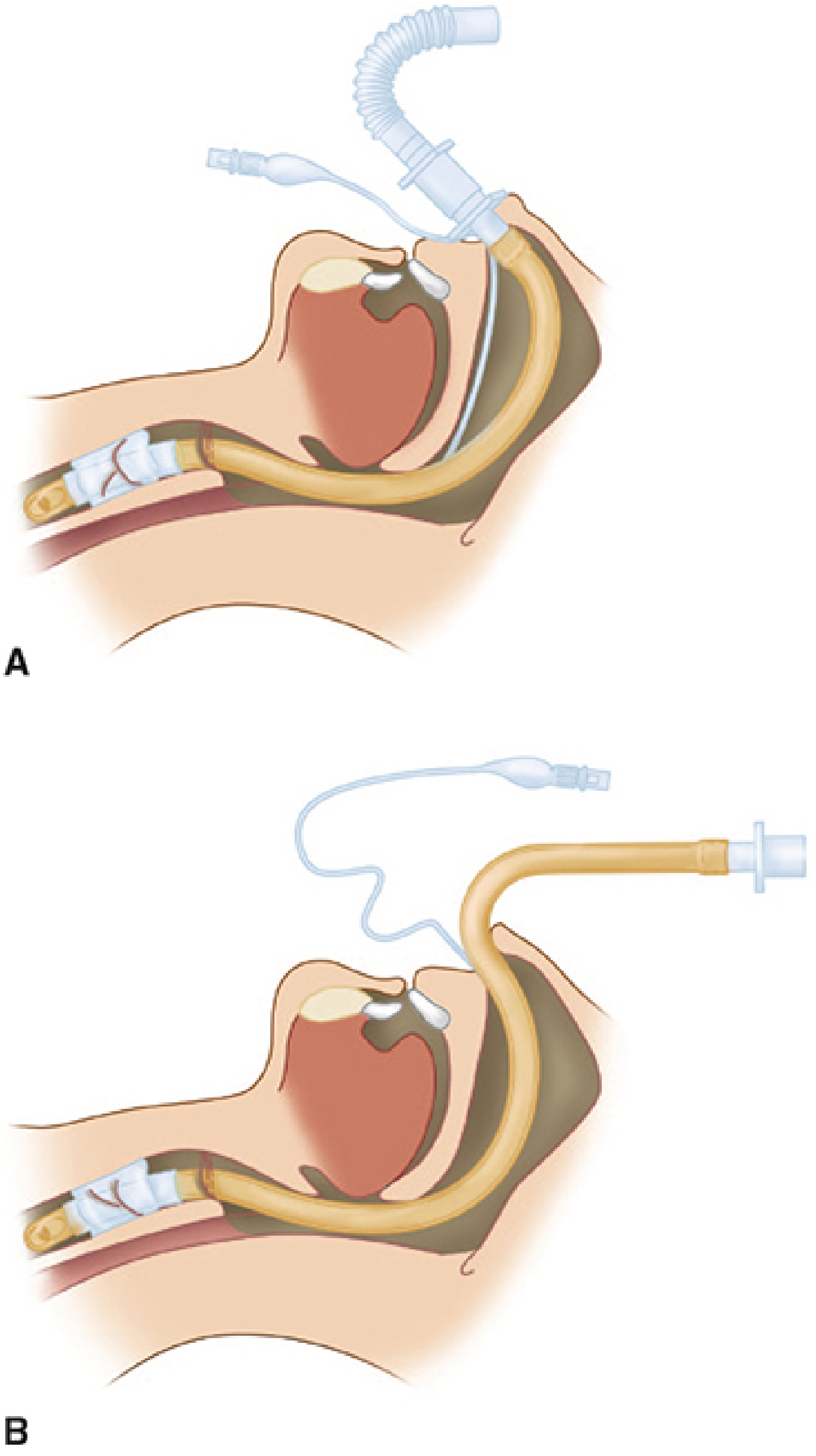
- Oral RAE (South-facing / "south-pole") — The preformed bend sits at the level of the teeth; the tube exits downward to rest on the patient's chin.
- Nasal RAE (North-facing / "north-pole") — The preformed bend sits at the level of the nares; the tube is directed upward over the patient's forehead.
Indications / Surgical Applications
| Type | Primary Uses |
|---|---|
| Oral RAE | Ophthalmic surgery, tonsillectomy & adenoidectomy, nasal surgery, oral surgery, any case where the circuit must exit away from the face |
| Nasal RAE | Dental surgery, oral & maxillofacial surgery (orthognathic surgery, Le Fort osteotomies), cleft palate repair — tube directed over the forehead |
Key Properties & Design Features
- Preformed contour maintains a low profile and prevents surgical interference.
- The proximal segment connects to the breathing circuit while the distal segment intubates the trachea — the bend keeps both ends clear of the operative site.
- Equipped with a high-volume, low-pressure cuff and pilot balloon.
- Standard 15 mm male connector for circuit attachment.
- Most are PVC — this is both a practical and a safety consideration (see Limitations below).
Clinical Considerations
Sizing / Depth:
- For nasal RAE tubes, the bend is fixed at a set depth for each tube size — size selection must be careful to ensure the tube reaches far enough into the trachea without being too shallow. Nasal tubes are typically positioned 20–30% deeper than the equivalent oral tube.
- For oral RAE tubes, the bend should sit at the level of the teeth; if too shallow, accidental extubation is a risk; if the tube is too long, endobronchial intubation may occur. This is particularly critical in pediatric patients, where glottis-to-carina distance is very small.
Ophthalmic surgery:
"The risk of endotracheal tube kinking and obstruction can be minimized by using a preformed oral RAE (Ring-Adair-Elwyn) endotracheal tube." — Morgan & Mikhail's Clinical Anesthesiology, 7e
Because the anesthesiologist is often positioned away from the airway during eye surgery, kinking of the circuit at the face is a real hazard, and the oral RAE eliminates it.
Maxillofacial / oral surgery:
"Nasal intubation with a straight tube with a flexible angle connector or a preformed nasal RAE tube is usually preferred in dental and oral surgery. The endotracheal tube can then be directed cephalad over the patient's forehead." — Morgan & Mikhail's Clinical Anesthesiology, 7e
Nasal intubation should be used with caution in Le Fort II and III fractures because of possible coexisting basilar skull fracture.
Tonsillectomy/Adenoidectomy:
Oral RAE tubes are commonly used. The groove in most tongue blades of mouth gags accommodates the oral-down RAE to prevent compression and keep the tube clear of the field. (Barash's Clinical Anesthesia, 9e; Miller's Anesthesia, 10e)
A reinforced (armored) tube is preferred when tube kinking from surgical retraction or head rotation is a greater risk (e.g., ear surgery with head rotation, tonsillectomy with heavy retraction). The RAE tube is not kink-resistant because of its PVC construction.
Limitations & Hazards
- Fixed bend depth — cannot be adjusted; wrong size → risk of endobronchial intubation (too long) or extubation (too short). Critical in pediatric patients.
- Kinking / compression risk — PVC construction makes it susceptible to kinking, especially if compressed by surgical instruments or retractors. Armored tubes are preferred when kinking is a major concern.
- Fire risk — PVC is combustible. RAE tubes are relatively high risk for airway fire in transoral laser or electrocautery surgery. Laser-resistant tubes should be used when high-energy devices are used near the airway. (Cummings Otolaryngology, 6e)
- Nasal tissue pressure — with prolonged nasal intubation, the preformed nasal RAE must be positioned carefully to avoid pressure necrosis at the naris.
- Nasotracheal RAE severed by surgical instruments — case reports exist of the tube being cut by osteotomes during Le Fort I osteotomies.
RAE vs. Other Specialized Tubes
| Feature | Oral/Nasal RAE | Armored (Reinforced) | Laser-Resistant |
|---|---|---|---|
| Kink resistance | Low (PVC) | High (spiral wire) | Variable |
| Fire resistance | Low | Low–moderate | High |
| Best for | Surgical field clearance | Head rotation, retraction | Laser/electrocautery cases |
| Fixed depth | Yes (limitation) | No | No |
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Chapters 36 & 37
- Miller's Anesthesia, 10e, Chapter on Tracheal Intubation
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, Chapter on Endotracheal Tubes
- Cummings Otolaryngology Head & Neck Surgery, Chapter 97
This is a shared conversation. Sign in to Orris to start your own chat.