Minimally invasive glaucoma surgeries
Reading File
Finding Sources
Finding Sources
Searching PubMed
"minimally invasive glaucoma surgery" MIGS
Reading File
Reading File
Searching Images
minimally invasive glaucoma surgery MIGS trabecular stent iStent
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I now have comprehensive information to compose a detailed answer. Let me compile everything.
Minimally Invasive Glaucoma Surgery (MIGS)
MIGS refers to a group of implants and techniques designed to lower intraocular pressure (IOP) with a significantly lower risk profile than traditional glaucoma surgery (trabeculectomy or tube shunts). MIGS is commonly combined with cataract surgery and is most suitable for mild-to-moderate glaucoma where the rate of visual field loss is slow and a modest target pressure (15–17 mmHg) is acceptable.
Classification by Mechanism
MIGS procedures are grouped into three broad categories based on their anatomical target:
1. Schlemm Canal–Based (No Bleb) — Trabecular Outflow Route
These procedures target the trabecular meshwork (TM) or Schlemm canal directly. They do not create a filtering bleb, which avoids the hypotony and infection risks of bleb-dependent surgery.
| Procedure | Mechanism | Approach |
|---|---|---|
| Trabectome | Electrocautery ablation/excision of TM | Ab interno |
| Kahook Dual Blade (KDB) | Mechanical excision of TM strips | Ab interno |
| iStent inject (Gen 2) | Titanium micro-bypass stent through TM into Schlemm canal | Ab interno |
| Hydrus Microstent | 8 mm nitinol scaffold that dilates and stents Schlemm canal across 3 clock hours | Ab interno |
| Ab-interno canaloplasty (ABiC) with iTrack | Viscodilation + dilation of Schlemm canal 360° | Ab interno |
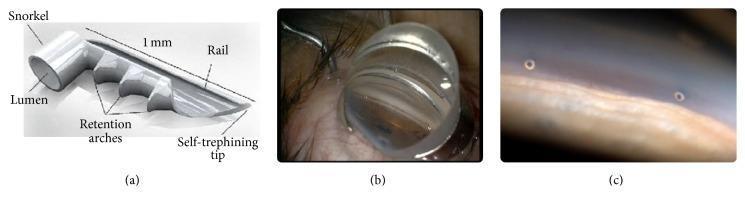
iStent — The 1 mm titanium stent has a self-trephining tip, retention arches, and a rail (see image below). Meta-analysis of stand-alone iStent implantation shows ~30% IOP reduction from baseline sustained up to 5 years.
Hydrus Microstent — The Horizon RCT demonstrated that the Hydrus stent, implanted at the time of phacoemulsification, was safer, less likely to result in visual field loss, and more effective at lowering IOP with fewer medications compared to phacoemulsification alone at 5 years.
2. Subconjunctival / Bleb-Forming Micro-Stents
These devices drain aqueous from the anterior chamber through a micro-stent into the subconjunctival or sub-Tenon space, forming a low-lying, diffuse bleb. Mitomycin C (0.02%, 0.1 mL subconjunctival) is typically co-administered to reduce bleb fibrosis. Bleb needling is often required postoperatively.
| Device | Design | Notes |
|---|---|---|
| Xen Gel Stent | 6 mm porcine gelatin tube, 45 µm lumen | Ab interno; self-titrating resistance |
| Preserflo MicroShunt | SIBS polymer tube (8.5 mm) | Ab externo approach; similar to Xen in outcomes |
| InnFocus MicroShunt | Precursor to Preserflo | Historical |
Stand-alone Xen implantation at 2 years shows ~30% IOP reduction and ~1 fewer medication on average compared to baseline.
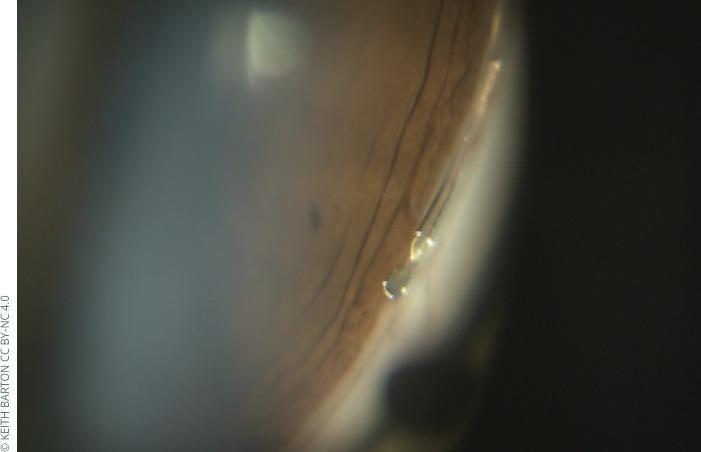
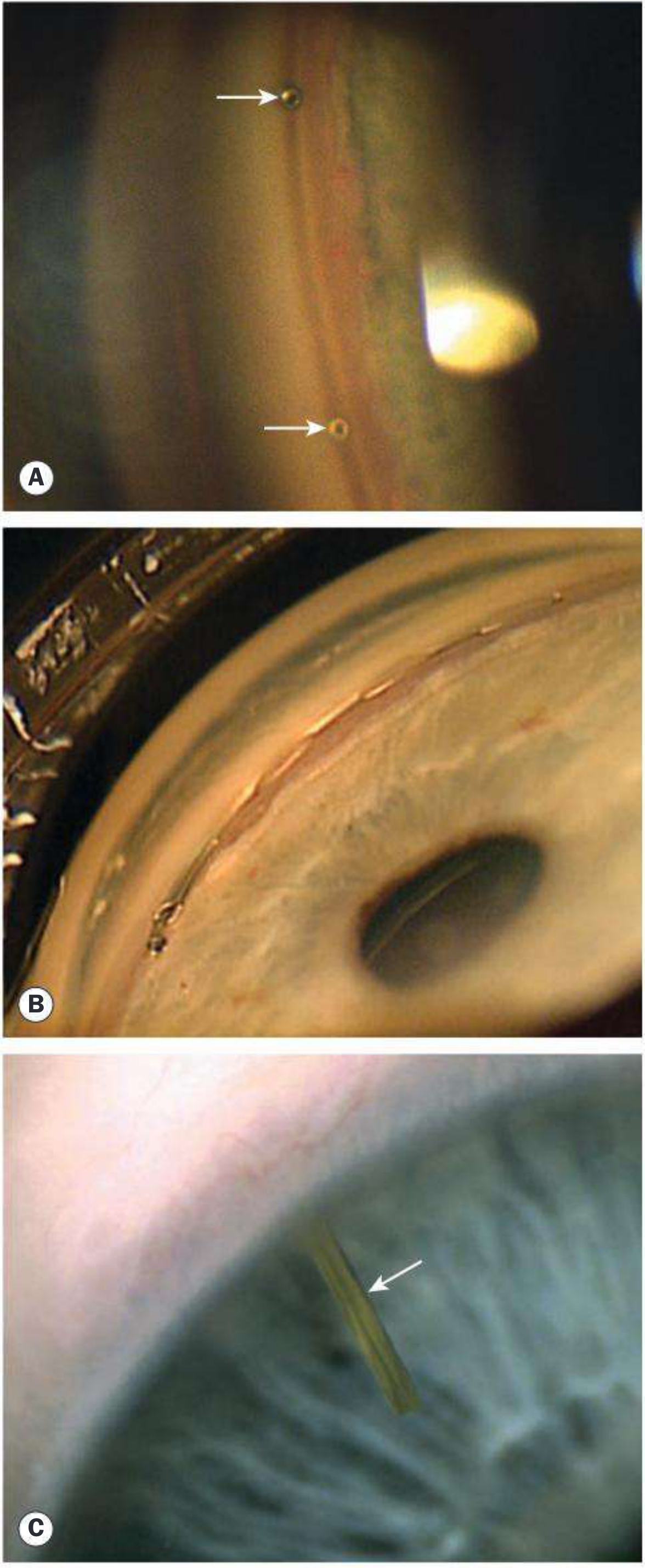
Gonioscopic views of all three main MIGS implant types (iStent, Hydrus, Xen):
3. Supraciliary / Suprachoroidal Route
These procedures augment uveoscleral outflow by placing an implant into the supraciliary space, avoiding bleb formation entirely.
| Device | Design | Notes |
|---|---|---|
| MINIject | 5 mm silicone implant (Star platform) with interconnected hollow spheres | Ab interno; protrudes 0.5 mm into AC; no antimetabolite used |
| CyPass (withdrawn 2018) | Supraciliary microstent | Withdrawn due to long-term corneal endothelial cell loss |
The MINIject carries a small risk of late corneal endothelial cell loss given proximity to the anterior chamber.
Indications
- Primary: Mild-to-moderate open-angle glaucoma (OAG) with a modest target IOP (15–17 mmHg)
- Combined with phacoemulsification/IOL — most common scenario; reduces need for topical medications postoperatively
- Not appropriate as stand-alone surgery for advanced glaucoma with aggressive target pressures (<12 mmHg)
Advantages Over Traditional Surgery
| Feature | MIGS | Trabeculectomy / Tube Shunt |
|---|---|---|
| IOP-lowering magnitude | Moderate (20–35%) | Greater (40–50%) |
| Recovery time | Short | Prolonged |
| Hypotony risk | Very low | Significant |
| Bleb-related complications | None (most procedures) | Blebitis, bleb dysesthesia |
| Repeat surgery options | Preserved | Conjunctival scarring limits options |
| Antimetabolite requirement | Rarely needed | Usually MMC-augmented |
Complications
Schlemm canal procedures:
- Implant malposition
- Hyphema (transient; from blood reflux into Schlemm canal)
- Infection
- Late corneal decompensation
Bleb-forming procedures (Xen, Preserflo):
- Same bleb-related complications as trabeculectomy (blebitis, hypotony, dysesthesia)
- Stent malposition or erosion
Supraciliary procedures:
- Small risk of late corneal endothelial cell loss (CyPass, MINIject)
Important long-term consideration: Late failure of MIGS — particularly bleb-forming variants — increases the risk of fibrosis if trabeculectomy is subsequently required.
Results Summary
| Procedure | IOP Reduction | Duration of evidence |
|---|---|---|
| Stand-alone iStent inject | ~30% | Up to 5 years |
| Hydrus (with phaco) | More effective than phaco alone | 5 years (Horizon study) |
| Xen (stand-alone) | ~30% + ~1 fewer medication | 2 years |
Note: Results are biased because MIGS is often combined with cataract surgery, which independently lowers IOP by ~15%.
Recent Evidence (2023–2025)
Recent systematic reviews and meta-analyses support and refine MIGS use:
- Angle-based MIGS in normal tension glaucoma (Oo et al., Clin Exp Ophthalmol 2024) — Systematic review/meta-analysis confirming efficacy of trabecular MIGS in NTG. [PMID 38853535]
- MIGS + phaco in primary angle-closure glaucoma (Fang et al., BMC Ophthalmol 2025) — TM/Schlemm canal-based MIGS combined with phacoemulsification is effective in PACG. [PMID 40181304]
- MIGS in normal tension glaucoma (Yu et al., BMC Ophthalmol 2025) — Microinvasive glaucoma surgery alone or combined with phaco is effective in NTG. [PMID 40340860]
- Microcatheter-assisted MIGS network meta-analysis (Han et al., Surv Ophthalmol 2025) — Network meta-analysis of canaloplasty/viscodilation-based procedures in OAG. [PMID 40484184]
- Minimally invasive bleb surgery health technology assessment (Ontario Health 2024) — Comprehensive HTA comparing Xen and Preserflo vs. trabeculectomy. [PMID 38332948]
Sources: Kanski's Clinical Ophthalmology, 10th ed., p. 439; Wills Eye Manual, 7th ed., p. 556; Miller's Anesthesia, 10th ed.
This is a shared conversation. Sign in to Orris to start your own chat.