Tell me step by step what all shud be checked in ecg strip with all leads and what are normal levels for interpretation for everything
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the content needed to write a thorough, well-organized answer. Here is the complete step-by-step ECG interpretation guide:
Complete Step-by-Step ECG Interpretation Guide
Normal 12-lead ECG (Goldman-Cecil Medicine):
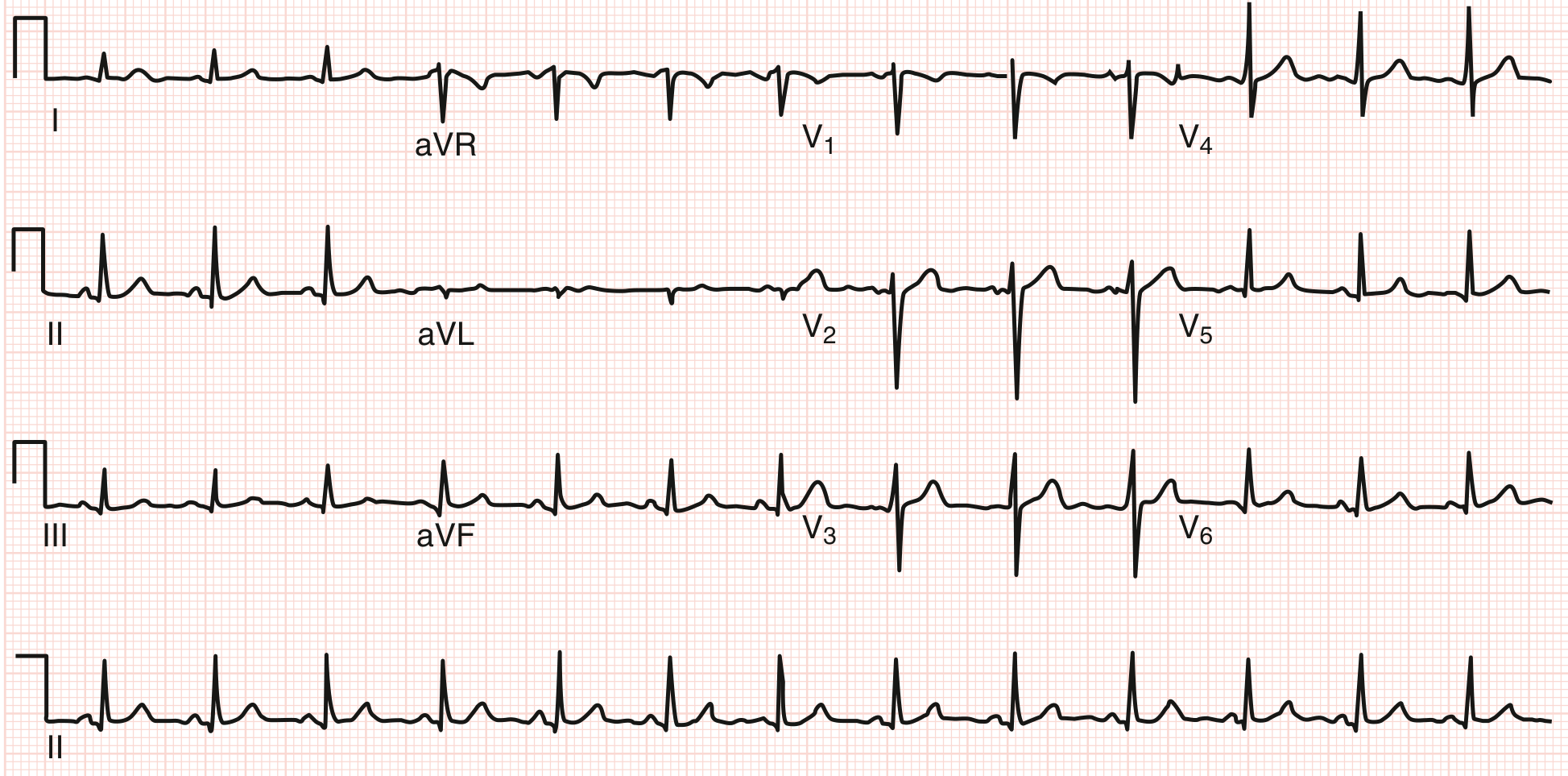
Heart rate ~78 bpm. Axis ~+60°. PR ~140 ms, QRS ~90 ms, QT ~360 ms. Sinus arrhythmia present. Transition at V3/V4.
Harrison's Principles of Internal Medicine (22E) lists 14 parameters to analyze systematically on every ECG. Work through them in order - errors in ECG reading are nearly always errors of omission.
STEP 1 - Standardization and Technical Quality
Before reading the tracing, check the paper itself.
Paper speed: Standard = 25 mm/sec
- 1 small box = 0.04 sec (40 ms)
- 1 large box (5 small) = 0.20 sec (200 ms)
Calibration (gain): Standard = 10 mm/mV (1 mV = 10 mm tall)
- Check for the calibration pulse at the start of the strip - it should be exactly 10 mm tall and 1 large box wide
- If half-standard (5 mm/mV) was used due to large voltages, all amplitude values must be doubled
Lead placement artifacts: Check for reversed leads, wandering baseline, muscle tremor artifact, 60 Hz AC interference. Limb lead reversal (e.g., LA/RA swap) is the most common technical error - suspect it when lead I shows a completely negative P and QRS.
STEP 2 - Rhythm
Ask three questions: Is it regular? Is there a P wave before every QRS? Is there a QRS after every P wave?
Normal sinus rhythm (NSR) criteria:
- P waves present, upright in leads I, II, aVF; inverted in aVR
- Each P wave followed by a QRS
- Rate 60-100 bpm
- Regular RR intervals (minor variability = sinus arrhythmia, normal)
P wave axis: Should be between 0° and +75° in the frontal plane, meaning positive in I and II, negative in aVR.
Key rhythm abnormalities to identify:
| Rhythm | Clue |
|---|---|
| Atrial fibrillation | No discrete P waves, irregularly irregular RR |
| Atrial flutter | Sawtooth flutter waves ~300 bpm, usually 2:1 or 4:1 block |
| Junctional rhythm | Retrograde P (negative II, III, aVF) or absent P, rate 40-60 |
| Ventricular rhythm | Wide QRS >120 ms, no P-QRS relationship, rate 20-40 |
| SVT | Narrow QRS, rate 150-250, P often buried in QRS or just after |
STEP 3 - Heart Rate
Method 1 (Regular rhythm): 300 ÷ number of large boxes between two consecutive R waves
- 1 large box = 300 bpm; 2 = 150; 3 = 100; 4 = 75; 5 = 60; 6 = 50
Method 2 (Irregular rhythm): Count QRS complexes in a 10-second strip and multiply by 6.
Normal: 60-100 bpm
Bradycardia: <60 bpm
Tachycardia: >100 bpm
Bradycardia: <60 bpm
Tachycardia: >100 bpm
STEP 4 - PR Interval
Measured from onset of P wave to onset of QRS complex.
Normal: 120-200 ms (3-5 small boxes)
| Finding | Interval | Meaning |
|---|---|---|
| Short PR | <120 ms | Pre-excitation (WPW), junctional rhythm, LGL |
| 1st degree AV block | >200 ms | Prolonged but consistent - every P conducts |
| 2nd degree AV block (Mobitz I) | Progressively lengthening PR until a QRS drops (Wenckebach) | |
| 2nd degree AV block (Mobitz II) | Fixed PR, then sudden dropped QRS without warning | |
| 3rd degree AV block | P and QRS completely dissociated |
STEP 5 - QRS Duration
Measured from the first deflection of the QRS to the end of the last deflection, in the widest lead.
Normal: 60-100 ms (<3 small boxes); upper limit of normal = 110 ms
| Finding | Duration | Meaning |
|---|---|---|
| Incomplete BBB | 100-119 ms | Delayed but not complete block |
| Complete LBBB | ≥120 ms | Broad, notched R in I, aVL, V5, V6; QS or rS in V1 |
| Complete RBBB | ≥120 ms | RSR' ("rabbit ears") in V1; broad S in I, V5, V6 |
| IVCD | >110 ms | Non-specific intraventricular conduction delay |
| Ventricular rhythm/WPW | Often ≥120 ms | Delta wave in WPW |
Left anterior fascicular block (LAFB): QRS <120 ms, axis -45° to -90°, small q in I/aVL, small r in III/aVF
Left posterior fascicular block (LPFB): QRS <120 ms, axis +90° to +180°, rS in I/aVL, qR in III/aVF
Left posterior fascicular block (LPFB): QRS <120 ms, axis +90° to +180°, rS in I/aVL, qR in III/aVF
STEP 6 - QT and QTc Interval
Measured from onset of QRS to end of T wave. Use lead II or V5 (clearest T wave offset). Measure the longest QT across all leads.
Normal QT: Roughly half the RR interval (Bazett's rule of thumb)
Corrected QT (QTc) using Bazett's formula: QTc = QT ÷ √(RR interval in seconds)
| Sex | Normal QTc | Borderline | Prolonged |
|---|---|---|---|
| Male | <430 ms | 430-450 ms | >450 ms |
| Female | <440 ms | 440-460 ms | >460 ms |
| Alarming (torsades risk) | - | - | >500 ms |
Short QT: <340 ms - associated with short QT syndrome (sudden death risk)
Common causes of prolonged QT: Hypokalemia, hypomagnesemia, hypocalcemia, drugs (amiodarone, sotalol, haloperidol, macrolides, fluoroquinolones), congenital long QT syndromes, hypothyroidism.
STEP 7 - Mean QRS Axis (Frontal Plane)
The axis describes the average direction of ventricular depolarization in the frontal plane.
Normal axis: -30° to +90° (some sources say -30° to +100°)
Quick method: Look at leads I and aVF:
- Both positive → Normal axis (roughly 0° to +90°)
- I positive, aVF negative → check lead II; if II positive = normal; if II negative = LAD
- I negative, aVF positive → Right axis deviation
- Both negative → Extreme/indeterminate axis
| Axis | Degrees | Causes |
|---|---|---|
| Normal | -30° to +90° | Healthy |
| Left axis deviation (LAD) | More negative than -30° | LAFB, inferior MI, LVH, LBBB |
| Right axis deviation (RAD) | More positive than +90° | RVH, LPFB, lateral MI, PE, COPD, normal in children |
| Extreme/NW axis | -90° to ±180° | LPFB + LAFB, severe RVH, ventricular tachycardia |
STEP 8 - P Waves
Normal P wave:
- Duration: <120 ms (3 small boxes) in adults; <90 ms in children
- Amplitude: <2.5 mm (0.25 mV) in limb leads; <1.5 mm in V1
- Morphology: Upright (positive) in I, II, aVF, V4-V6; biphasic in V1 (small positive then small negative deflection); inverted in aVR
Abnormal P waves:
| Finding | Description | Meaning |
|---|---|---|
| P mitrale | Wide (>120 ms), notched P in II, wide terminal negative in V1 | Left atrial enlargement |
| P pulmonale | Tall (>2.5 mm), peaked P in II, III, aVF | Right atrial enlargement |
| Absent P waves | - | Atrial fibrillation, hyperkalemia |
| Retrograde P | Inverted in II, III, aVF | Junctional/ectopic atrial rhythm |
| Variable P morphology | - | Wandering pacemaker, multifocal atrial tachycardia |
STEP 9 - QRS Voltages (Amplitude)
Normal R wave amplitudes:
- Lead I: ≤13 mm; Lead aVL: ≤11-13 mm
- Lead II, III, aVF: variable; tall R in aVF normal
- V1: R wave normally small (≤6-7 mm); S wave dominant
- V5/V6: R wave ≤25-27 mm
Left ventricular hypertrophy (LVH) criteria (adults):
- Sokolow-Lyon: S in V1 + R in V5 or V6 >35 mm
- Cornell: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- R in aVL alone >11-13 mm
- LVH is often accompanied by LV "strain" pattern: ST depression + T wave inversion in lateral leads (I, aVL, V5, V6)
Right ventricular hypertrophy (RVH):
- R > S in V1 (normally S dominates V1)
- R in V1 >7 mm; S in V5/V6 >7 mm
- RAD (>+90°)
- RV "strain": ST depression + T inversion in V1-V3, II, III, aVF
Low voltage: QRS amplitude <5 mm in all limb leads AND <10 mm in all precordial leads
- Causes: Pericardial effusion, hypothyroidism, COPD (emphysema), obesity
STEP 10 - Precordial R-Wave Progression
As you move from V1 to V6, R waves should increase in size and S waves should decrease.
Transition zone: The lead where R = S in amplitude; normally V3 or V4.
Poor R-wave progression (PRWP): R wave fails to grow or grows very slowly V1 → V4
- Causes: Anterior MI (especially if Q waves accompany), LVH, LBBB, COPD, lead misplacement
Early transition (before V3): Posterior MI, RVH, normal variant
Tall R in V1 (R > S): RVH, RBBB, posterior MI, WPW (type A), HCM, normal variant in young
STEP 11 - Abnormal Q Waves
A small septal q wave is normal in I, aVL, V5, V6 (reflecting left-to-right septal depolarization). These are narrow (<30 ms) and shallow (<25% of R wave height).
Pathological Q waves (sign of prior full-thickness or transmural infarction):
- Width ≥40 ms (1 small box) OR
- Depth ≥25% of the height of the R wave in the same lead
Q wave location and territory:
| Leads with Q waves | Infarct territory | Artery |
|---|---|---|
| V1-V4 | Anterior / anteroseptal | LAD |
| I, aVL, V5-V6 | Lateral | LCx or diagonal |
| II, III, aVF | Inferior | RCA (or LCx in left-dominant) |
| V1-V2 tall R (posterior MI) | Posterior | RCA / LCx |
Important: Q waves in aVR are normal. Q in III alone (without II) is often a normal variant (especially with deep inspiration).
STEP 12 - ST Segments
The ST segment runs from the J point (end of QRS) to the onset of the T wave.
Normal: Isoelectric (flat, at baseline). Slight J-point elevation up to 1 mm is normal in limb leads; up to 2-3 mm early repolarization variant is common in young men in precordial leads.
ST Elevation - significant if:
- ≥1 mm (0.1 mV) in 2 or more contiguous limb leads
- ≥2 mm (0.2 mV) in 2 or more contiguous precordial leads (≥2.5 mm in men <40 years in V2-V3)
- ≥1.5 mm in women in V2-V3
Causes of ST elevation:
| Pattern | Description | Cause |
|---|---|---|
| STEMI | Focal, convex (tombstone) elevation with reciprocal depression | Acute transmural MI |
| Pericarditis | Diffuse concave ("saddle shape") elevation in most leads + PR depression | Inflammation |
| Early repolarization | Concave ST elevation, J-point notching, mainly V2-V5 | Benign variant |
| Osborn (J) waves | Positive notch at J point | Hypothermia |
| Brugada pattern | Coved ST elevation V1-V2 | Brugada syndrome |
ST Depression - significant if:
- ≥0.5-1 mm in 2 or more contiguous leads
Causes: Subendocardial ischemia, reciprocal change in STEMI, LVH strain, digoxin effect (scooped/sagging), LBBB.
STEP 13 - T Waves
Normal T waves:
- Upright in I, II, V3-V6; aVF usually upright
- Inverted (negative) in aVR - always; often inverted in V1 and III (normal variants)
- Amplitude: < ⅔ of R wave height in the same lead; usually <6 mm in limb leads, <10 mm in precordial leads
- Asymmetric: gradual upstroke, faster downstroke
T wave changes:
| Finding | Meaning |
|---|---|
| Peaked/tall symmetric T waves ("hyperacute") | Early acute MI, hyperkalemia |
| Diffuse T inversion | Myocarditis, Takotsubo, raised intracranial pressure |
| Deep symmetric T inversion V1-V4 | Anterior ischemia, Wellens syndrome (critical LAD stenosis) |
| T inversion I, aVL, V5-V6 | Lateral ischemia or LVH strain |
| T inversion II, III, aVF | Inferior ischemia or RVH strain |
| T-QRS discordance in LBBB | Expected; concordant changes suggest ischemia (Sgarbossa criteria) |
| Flattened or biphasic T | Nonspecific, hypokalemia, early ischemia |
T wave alternans (beat-to-beat amplitude variation): sign of electrical instability, may precede ventricular tachyarrhythmias.
STEP 14 - U Waves
A small deflection after the T wave, best seen in V2-V3.
Normal U wave:
- Same direction as T wave
- Amplitude <25% of T wave amplitude (usually <1-2 mm)
Prominent U waves (>2 mm):
- Hypokalemia (most common cause)
- Hypomagnesemia
- Bradycardia
- Some antiarrhythmic drugs
Inverted U waves: Abnormal; associated with LVH, ischemia, hypertension.
Note: If T and U waves merge, the apparent QT may look prolonged. If they separate, the true QT is actually normal.
Lead-by-Lead Normal Morphology Reference
| Lead | Normal P | Normal QRS | Normal T | Notes |
|---|---|---|---|---|
| I | Upright | Upright (net positive) | Upright | aVR mirror image |
| II | Upright, tall | Upright, tall R | Upright | Best lead for rhythm strip |
| III | Upright or biphasic | Variable (Q in III alone can be normal) | Variable | |
| aVR | Inverted | Inverted/all negative | Inverted | "Cavity" lead |
| aVL | Upright or biphasic | R or rS | Upright or flat | rS normal especially in young |
| aVF | Upright | Upright | Upright | Inferior wall |
| V1 | Biphasic (+ then -) | rS (small r, big S) | Inverted or flat (normal) | Right sided; RSR' = RBBB |
| V2 | Upright | rS or RS | Variable, often inverted | |
| V3 | Upright | Transitional (RS) | Upright | Transition zone starts here |
| V4 | Upright | RS or Rs | Upright | Transition completes here |
| V5 | Upright | Rs (tall R) | Upright | Septal q normal |
| V6 | Upright | Rs (tall R, small s) | Upright | Septal q normal |
Quick Normal Values Summary Table
| Parameter | Normal Range |
|---|---|
| Heart rate | 60-100 bpm |
| PR interval | 120-200 ms (0.12-0.20 sec) |
| QRS duration | 60-110 ms (<3 small boxes) |
| QRS axis | -30° to +90° |
| QTc (male) | <440-450 ms |
| QTc (female) | <460 ms |
| P wave duration | <120 ms adults; <90 ms children |
| P wave amplitude | <2.5 mm in limb leads |
| ST elevation | <1 mm limb leads; <2 mm precordial |
| T wave direction | Concordant with QRS in most leads |
| U wave amplitude | <2 mm; same direction as T |
| Transition zone (V1-V6) | R = S at V3 or V4 |
Systematic Memory Aid: "SR-HPQQ-RSTУ"
A quick mnemonic for bedside reading:
- Standardization/technical quality
- Rhythm (P before every QRS?)
- Heart rate
- PR interval
- QRS duration
- QT/QTc
- Axis
- P-wave morphology
- Voltage (QRS amplitude / LVH/RVH)
- R-wave progression (V1→V6)
- Q waves (pathological?)
- ST segments
- T waves
- U waves
- Compare with prior ECG - always the final step
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine International Edition; Harriet Lane Handbook 23rd Ed.
Always compare with a prior ECG when available - changes over time often matter more than a single reading in isolation.
This is a shared conversation. Sign in to Orris to start your own chat.