Stemi ecg changes
Reading File
Finding Sources
Searching Images
STEMI ECG changes ST elevation myocardial infarction
Finding Sources
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive, well-illustrated answer.
STEMI: ECG Changes
Pathophysiology of ST Changes
Transmural (full-thickness) ischemia creates a current of injury between normal and ischemic myocardium. The ST vector shifts outward (toward the epicardium), producing ST elevation in leads overlying the affected zone and reciprocal ST depression in opposite leads.

Diagnostic ECG Criteria for STEMI
The standard criteria require new ST elevation at the J-point in ≥2 contiguous leads:
- ≥1 mm in all leads except V2–V3
- ≥2 mm in V2–V3 in men ≥40 years; ≥2.5 mm in men <40 years; ≥1.5 mm in women
Lead Localisation by Territory
| Territory | ST Elevation Leads | Likely Vessel |
|---|---|---|
| Anteroseptal | V1, V2 (±V3) | LAD (proximal) |
| Anterior | V1–V4 | LAD |
| Anterolateral | V1–V6, I, aVL | LAD (proximal) or LCx |
| Lateral | I, aVL | Diagonal / LCx |
| Inferior | II, III, aVF | RCA (80%) or LCx (20%) |
| Inferolateral | II, III, aVF, V5–V6 | RCA or LCx |
| True posterior | Tall R in V1–V2 (R/S ≥1); ST depression V1–V3 | LCx or posterior RCA |
| Right ventricular | II, III, aVF + V3R–V6R elevation | Proximal RCA |
From Tintinalli's Emergency Medicine, Table 49-4
Clinical pearl: In inferior STEMI, always obtain right-sided lead V4R — ST elevation ≥1 mm in V4R is highly specific for right ventricular infarction.
Sequential ECG Evolution
STEMI produces characteristic time-dependent changes:
| Phase | Timing | ECG Finding |
|---|---|---|
| Hyperacute | Minutes | Tall, peaked (hyperacute) T waves |
| Acute | Hours | Convex ("tombstone") ST elevation; ST merges with T wave |
| Early evolving | Hours–days | ST begins to fall; T-wave inversion develops |
| Late evolving | Days–weeks | Pathological Q waves form; T inversions deepen |
| Chronic/old MI | Weeks–months | Q waves persist; ST normalises; T may remain inverted or normalise |
Key Individual ECG Findings
1. ST Elevation
- Convex (coved) morphology is classic — the "tombstone" pattern
- Must be measured at the J-point
- Reciprocal ST depression in opposing leads confirms STEMI and indicates larger injury zone, more severe CAD, and higher mortality
2. Hyperacute T Waves
- Broad-based, symmetrically tall T waves
- Earliest sign — may precede ST elevation by minutes
- Prominent in V2–V4 in anterior STEMI
3. Pathological Q Waves
- Width ≥0.04 s (1 mm) or depth ≥25% of R wave
- Indicate myocardial necrosis (not always transmural)
- Develop within hours to days
- May persist permanently or regress with smaller infarcts
4. T-Wave Inversions
- Follow the ST elevation phase
- Deep symmetric inversions in precordial leads (V1–V4 with or without I, aVL) = Wellens pattern → suggests high-grade LAD stenosis

5. Reciprocal Changes
- ST depression in leads "opposite" the infarct zone
- Example: Inferior STEMI (II, III, aVF) → reciprocal ST depression in I and aVL
- Example: Anterior STEMI → reciprocal ST depression in II, III, aVF
- Their presence increases the probability of true STEMI and correlates with worse outcomes
Example ECGs
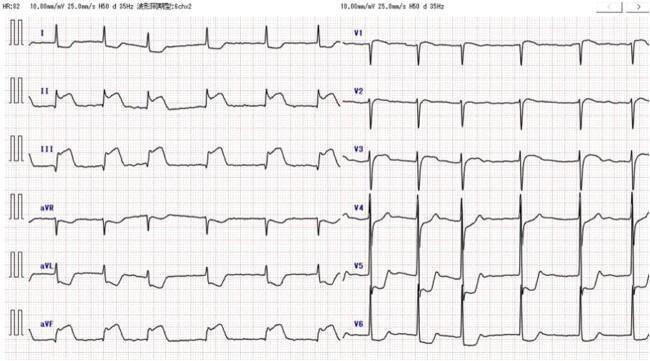
Anterolateral STEMI (LAD occlusion) — convex ST elevation V1–V6, I, aVL with reciprocal inferior depression:

Inferior STEMI (RCA occlusion) — ST elevation II, III, aVF; reciprocal depression in I, aVL, V4–V6:
STEMI Equivalents (No Classic STE)
These patterns should trigger the same urgent reperfusion response:
| Pattern | Significance |
|---|---|
| New LBBB | Sgarbossa criteria to identify STEMI underneath |
| De Winter pattern | Upsloping ST depression + tall T waves in V1–V6 → proximal LAD occlusion |
| Posterior STEMI | ST depression V1–V3 + tall R waves (mirror image) |
| Right ventricular STEMI | ST elevation V3R–V6R |
| aVR elevation | ST elevation in aVR ≥1 mm with diffuse ST depression → left main or proximal LAD occlusion |
ECG Limitations
- A single normal ECG does not exclude STEMI — repeat at 15–30 min intervals if symptoms persist
- LBBB, ventricular pacing, and WPW can mask ischemic changes
- Posterior MI shows no direct ST elevation in standard leads — posterior leads (V7–V9) are required
- <10% of patients with new LBBB actually have AMI
Sources: Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine, Comprehensive Study Guide
This is a shared conversation. Sign in to Orris to start your own chat.