Mandibular nerve 5 mark answer bds 1st year RGUHS
Reading File
Finding Sources
Searching the Web
mandibular nerve anatomy BDS 1st year RGUHS 5 mark answer
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a complete, exam-quality 5-mark answer. Here it is:
Mandibular Nerve (V3) - 5 Mark Answer (BDS 1st Year, RGUHS)
Introduction
The mandibular nerve (V3) is the largest of the three divisions of the trigeminal nerve (CN V). Unlike the ophthalmic (V1) and maxillary (V2) nerves, which are purely sensory, the mandibular nerve is both motor and sensory - it is the only division of the trigeminal nerve that carries a motor root.
Origin
- The sensory root originates from the trigeminal (Gasserian) ganglion in the middle cranial fossa.
- The motor root passes medial to the trigeminal ganglion and does not relay in it.
- Both roots exit the skull through the foramen ovale and unite in the infratemporal fossa to form the main trunk.
Course
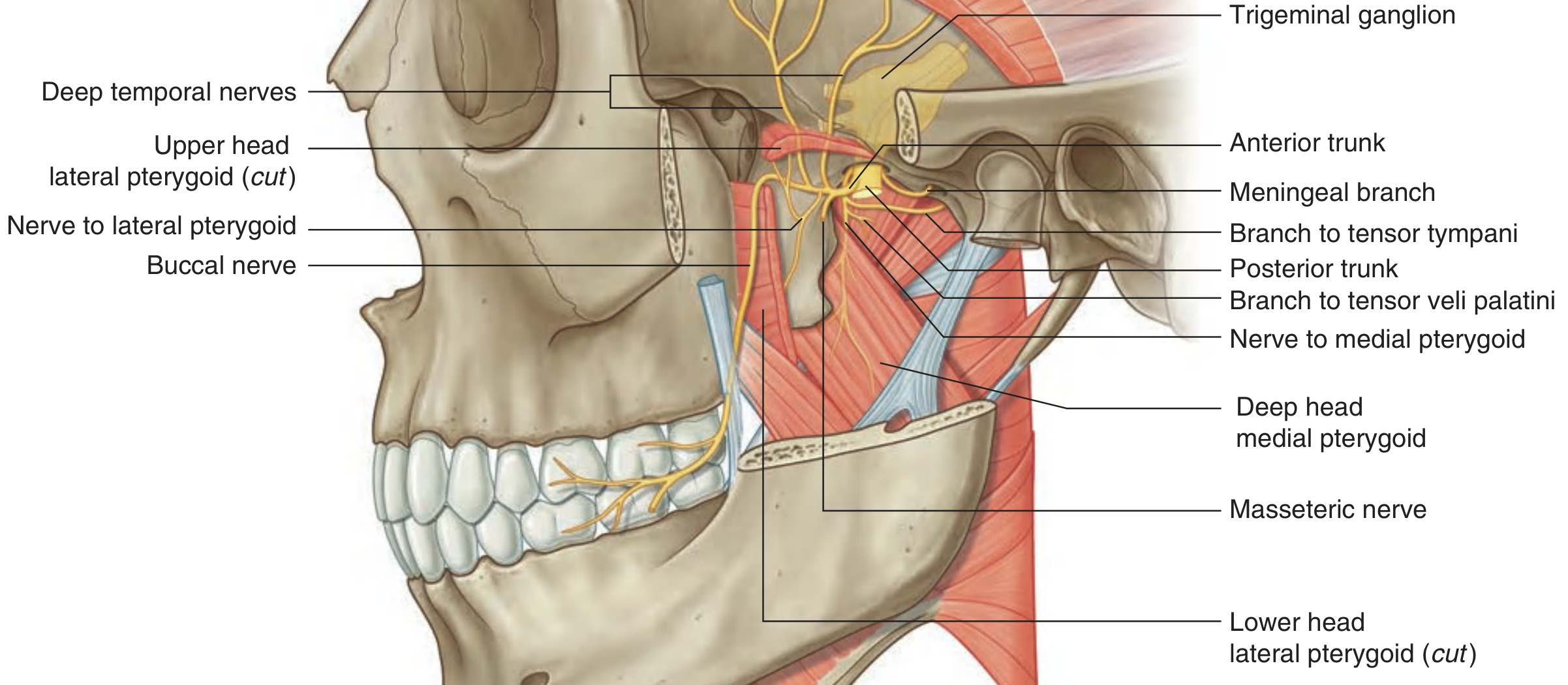
The nerve enters the infratemporal fossa between the tensor veli palatini (medially) and the upper head of the lateral pterygoid (laterally). All branches of V3 originate in the infratemporal fossa.
Branches
The main trunk first gives off:
- Meningeal branch (nervus spinosus) - re-enters skull through foramen spinosum; sensory to dura of middle cranial fossa and mastoid air cells.
- Nerve to medial pterygoid - motor to medial pterygoid, with twigs to tensor tympani and tensor veli palatini.
Then divides into anterior and posterior trunks:
Anterior Trunk (mostly motor, one sensory)
| Branch | Type | Distribution |
|---|---|---|
| Buccal nerve | Sensory | Skin and mucosa of cheek; buccal gingivae of lower molars |
| Masseteric nerve | Motor | Masseter muscle |
| Deep temporal nerves (x2) | Motor | Temporalis muscle (deep surface) |
| Nerve to lateral pterygoid | Motor | Lateral pterygoid muscle |
Posterior Trunk (mostly sensory, one motor branch)
| Branch | Type | Distribution |
|---|---|---|
| Auriculotemporal nerve | Sensory + parasympathetic relay | Skin of temple, external ear, EAC, tympanic membrane, TMJ; carries postganglionic parasympathetics from otic ganglion to parotid gland |
| Lingual nerve | Sensory (+ chorda tympani joins it) | General sensation - anterior 2/3 of tongue, floor of mouth, lingual gingivae; taste via chorda tympani; submandibular ganglion is suspended from it |
| Inferior alveolar nerve | Sensory + one motor branch | All lower teeth and gingivae; gives nerve to mylohyoid (motor to mylohyoid + anterior belly of digastric); divides terminally into mental nerve (chin and lower lip) and incisive nerve |
Sensory Distribution (Summary)
- Skin over lower face, lower lip, chin, temple, part of auricle
- Anterior two-thirds of tongue (general sensation)
- Mucosa of cheek, floor of mouth
- All mandibular teeth and associated gingivae
- TMJ, external acoustic meatus, tympanic membrane
- Dura of middle cranial fossa
Motor Distribution (Summary)
The mandibular nerve supplies 8 muscles:
- Temporalis
- Masseter
- Medial pterygoid
- Lateral pterygoid
- Tensor tympani
- Tensor veli palatini
- Mylohyoid
- Anterior belly of digastric
Applied Anatomy / Clinical Significance
- Inferior alveolar nerve block - injected near the mandibular foramen (between sphenomandibular ligament and ramus) to anaesthetize all lower teeth on that side; widely used in dentistry.
- Mental nerve block - at the mental foramen, anaesthetizes lower lip and chin.
- Lingual nerve injury - during lower third molar extraction; causes loss of general sensation and taste from anterior 2/3 of tongue.
- Auriculotemporal nerve - carries secretomotor fibres to the parotid; damage can cause Frey's syndrome (gustatory sweating after parotid surgery).
Source: Gray's Anatomy for Students, 4th Ed. - Chapter 8 (Infratemporal Fossa)
Scalp layers , nerve supply and blood supply and clinical anatomy 10 mark question
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
All content and images are gathered. Here is the complete 10-mark exam answer:
SCALP - 10 Mark Answer (BDS 1st Year, RGUHS)
Definition and Extent
The scalp is the soft tissue covering of the calvaria (vault of the skull). It extends:
- Anteriorly - from the superciliary arches
- Posteriorly - to the external occipital protuberance and superior nuchal lines
- Laterally - down to the zygomatic arches on each side
Layers of the Scalp (S-C-A-L-P)
The layers of the scalp are conveniently remembered by the word SCALP itself:
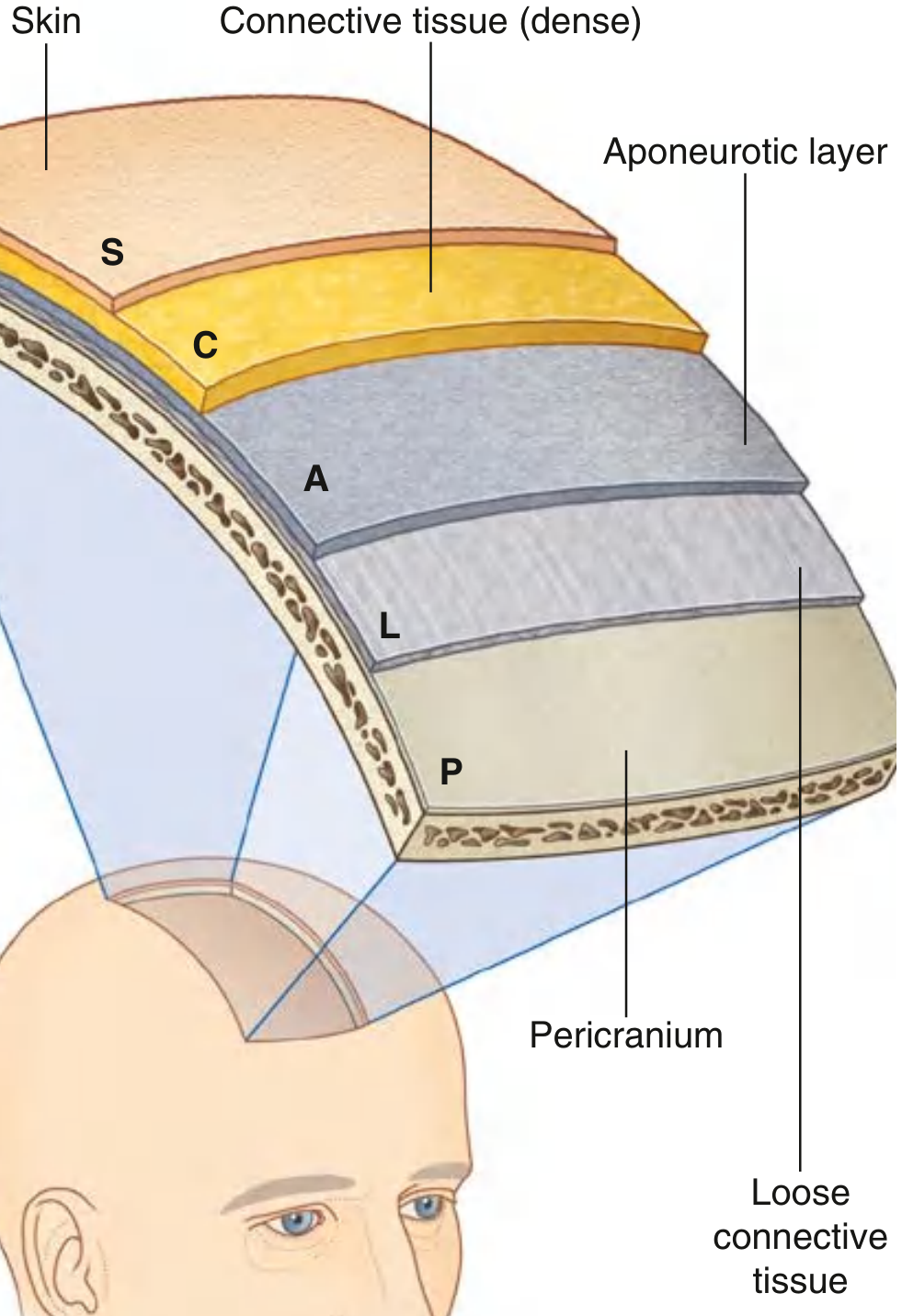
1. S - Skin
- Outer most layer; thickest skin in the body
- Contains hair follicles, sebaceous glands, and sweat glands
- Hair follicles extend deep into the connective tissue layer below
2. C - (Dense) Connective Tissue
- Immediately deep to the skin; tightly anchors skin to the aponeurotic layer
- Contains all the blood vessels and nerves of the scalp
- The dense fibrous septa surrounding vessels prevent their retraction when cut - this is why scalp wounds bleed profusely
- Arteries, veins, and nerves of the scalp all run in this layer
3. A - Aponeurotic Layer (Epicranial Aponeurosis / Galea Aponeurotica)
- A sheet of dense fibrous tissue connecting the frontal belly (frontalis) anteriorly to the occipital belly (occipitalis) posteriorly
- Together the muscles and aponeurosis form the occipitofrontalis (epicranius) muscle
- The first three layers (S-C-A) are bound tightly together and move as a single unit - this is called the "scalp proper" and is the tissue torn away during "scalping" injuries
4. L - Loose Connective Tissue (Subaponeurotic / Danger Layer)
- A loose, areolar layer separating the aponeurosis from the pericranium
- Allows the scalp proper to slide freely over the skull
- Also called the "dangerous area of the scalp" because:
- Infections spreading through this plane can reach the intracranial venous sinuses via emissary veins
- Blood from trauma collects here and can spread widely (subgaleal hematoma)
- Pus or blood here is limited anteriorly at orbital margins, posteriorly at nuchal lines, and laterally by temporal fascia attachment
5. P - Pericranium
- The deepest layer; the periosteum of the outer surface of the calvaria
- Firmly attached at the cranial sutures but loosely attached over the bones
- Blood collecting between the pericranium and bone is called a cephalhematoma (limited to one bone because it cannot cross sutures)
Nerve Supply of the Scalp
Sensory innervation comes from two sources depending on location relative to the ears and vertex:

Anterior to the Ears and Vertex (Branches of Trigeminal Nerve, CN V)
| Nerve | Origin | Area Supplied |
|---|---|---|
| Supratrochlear nerve | Ophthalmic (V1) via frontal nerve | Forehead near midline, front of scalp |
| Supra-orbital nerve | Ophthalmic (V1) via frontal nerve | Forehead and front of scalp to vertex |
| Zygomaticotemporal nerve | Maxillary (V2) | Small anterior temporal region |
| Auriculotemporal nerve | Mandibular (V3) | Temporal region and scalp anterior to ear, up to vertex |
Posterior to the Ears and Vertex (Cervical Nerves, C2-C3)
| Nerve | Origin | Area Supplied |
|---|---|---|
| Greater occipital nerve | Posterior ramus of C2 | Large area of posterior scalp up to vertex (most important) |
| Lesser occipital nerve | Anterior ramus of C2 (cervical plexus) | Area posterior and superior to ear |
| Great auricular nerve | Anterior rami of C2 and C3 (cervical plexus) | Small area just posterior to ear |
| Third occipital nerve | Posterior ramus of C3 | Lower part of posterior scalp |
Motor supply: The occipitofrontalis muscle is innervated by the facial nerve (CN VII) - frontal belly by temporal branches; occipital belly by the posterior auricular branch.
Blood Supply of the Scalp
The scalp has an extremely rich blood supply from two sources:
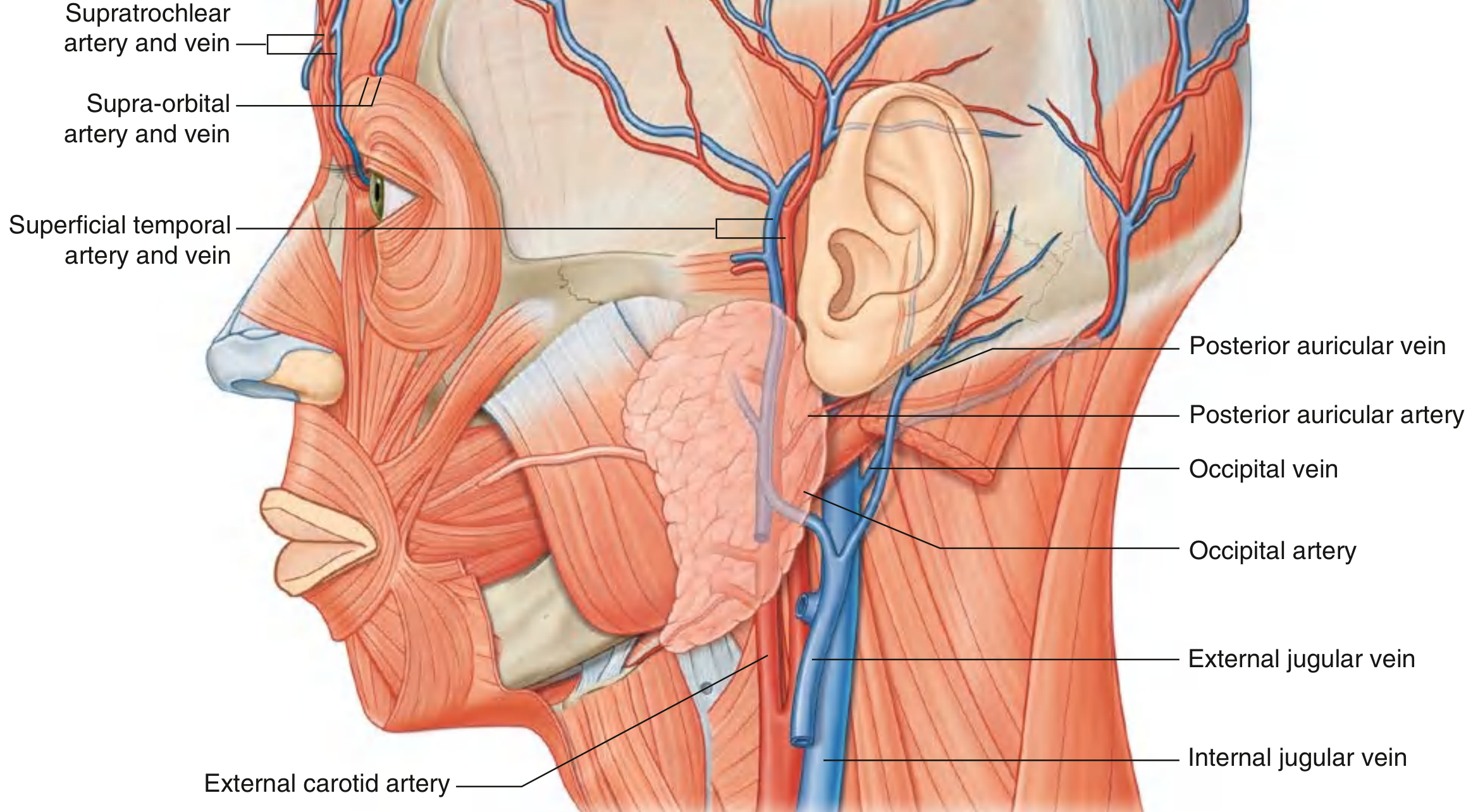
Arteries
From the Internal Carotid Artery (via Ophthalmic Artery):
- Supratrochlear artery - anterior scalp near midline
- Supra-orbital artery - anterior and superior scalp
From the External Carotid Artery:
- Superficial temporal artery (terminal branch of ECA) - divides into anterior and posterior branches; supplies the entire lateral scalp (largest contributor)
- Posterior auricular artery - small area posterior to the ear
- Occipital artery - large area of posterior scalp
Mnemonic for arteries: SASSO - Supratrochlear, Auricular (posterior), Superficial temporal, Supra-orbital, Occipital
Veins
Veins parallel the arteries in distribution:
- Supratrochlear and supra-orbital veins → angular vein → facial vein → internal jugular vein
- Superficial temporal vein → retromandibular vein → internal/external jugular veins
- Posterior auricular vein → external jugular vein
- Occipital vein → suboccipital venous plexus → vertebral vein
Important: Veins of the scalp communicate with diploic veins of the skull and with dural venous sinuses via emissary veins - this is clinically significant.
Lymphatic Drainage
- Occipital scalp → occipital lymph nodes → upper deep cervical nodes
- Posterior-lateral scalp (posterior to vertex) → mastoid (retro-auricular) nodes → upper deep cervical nodes
- Anterior to vertex → preauricular/parotid nodes → upper deep cervical nodes
- Forehead → submandibular nodes (via facial artery pathway)
Clinical Anatomy
1. Profuse Bleeding in Scalp Lacerations
Scalp wounds bleed extensively because:
- The scalp has an extremely rich blood supply
- Blood vessels lie in the dense connective tissue (layer C) - the fibrous septa hold cut vessels open and prevent retraction, so they cannot constrict spontaneously
- In the erect posture, venous pressure is very low, so bleeding is predominantly arterial
Management: Firm pressure; suturing; all layers of the scalp must be sutured for hemostasis.
2. "Dangerous Area" / Subgaleal Plane (Layer L)
- The loose areolar layer (L) is called the "dangerous area" because infections here can spread:
- Anteriorly to the orbit (limited by orbital margins)
- Intracranially via emissary veins to the dural venous sinuses, causing meningitis or cavernous sinus thrombosis
- Subgaleal hematomas spread widely over the whole calvaria (not limited to one bone like cephalhematoma)
3. Cephalhematoma vs. Subgaleal Hematoma
| Feature | Cephalhematoma (Layer P) | Subgaleal Hematoma (Layer L) |
|---|---|---|
| Layer involved | Between pericranium and bone | Below galea, above pericranium |
| Crossing sutures? | No - limited to one bone | Yes - spreads widely |
| Clinical setting | Birth trauma (neonate) | Trauma, vacuum delivery |
4. Scalping Injuries
- Since layers S, C, and A are tightly bound, they are torn away together as a unit - the "scalp proper"
- The avulsed flap retains its blood supply if the pedicle is intact (important for reimplantation)
5. Occipital Neuralgia
- Irritation or entrapment of the greater occipital nerve (C2) causes shooting pain over the posterior scalp
- Tender point over the greater occipital nerve at the superior nuchal line
6. Temporal Arteritis (Giant Cell Arteritis)
- Inflammatory disease of the superficial temporal artery (branch of ECA supplying the lateral scalp)
- Presents with tender, thickened, non-pulsatile temporal artery, headache, and risk of blindness (ophthalmic artery involvement)
- Treated with corticosteroids
7. Scalp Ringworm (Tinea Capitis) and Infections
- Infection can spread widely in the loose areolar layer
- Emissary veins connect scalp veins to dural sinuses - scalp infections can therefore lead to intracranial sepsis
Source: Gray's Anatomy for Students, 4th Ed. - Chapter 8, Head and Neck
This is a shared conversation. Sign in to Orris to start your own chat.