Hematuria
Reading File
Finding Sources
Finding Sources
Searching PubMed
hematuria evaluation management
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have thorough content from multiple authoritative sources. Let me compile the comprehensive answer.
Hematuria
Definition
Hematuria is the presence of blood (red blood cells) in the urine. It is classified as:
- Gross (macroscopic) hematuria - visible to the naked eye; urine appears red or brown
- Microscopic hematuria - detected only on urinalysis; defined as ≥3 RBCs per high-power field (HPF) on properly collected midstream urine microscopy
Asymptomatic microscopic hematuria (AMH) may be detected by dipstick in up to 16% of screening populations, but dipstick alone is insufficient - urine microscopy must confirm true RBCs. - Henry's Clinical Diagnosis and Management by Laboratory Methods, p.551
Pseudohematuria
Before workup, exclude pseudohematuria - red/brown urine without RBCs on microscopy. Causes include:
- Foods: beets, rhubarb, blackberries
- Drugs: rifampicin, phenazopyridine, nitrofurantoin, chloroquine
- Metabolites: myoglobinuria (rhabdomyolysis), hemoglobinuria (hemolysis)
- Porphyria
The absence of RBCs on microscopy with a positive dipstick heme strongly suggests hemoglobinuria or myoglobinuria. - Campbell-Walsh-Wein Urology
Classification by Origin
1. Glomerular Hematuria
| Feature | Finding |
|---|---|
| Urine color | Brown / "tea-colored" / "cola-colored" |
| RBC morphology | Dysmorphic / acanthocytes ("crenated" / Mickey Mouse cells) |
| RBC casts | Present - pathognomonic of glomerulonephritis |
| Proteinuria | Significant - often >500 mg/day |
| Clots | Absent |
Causes:
- IgA nephropathy (Berger disease) - most common; hematuria follows URTI by 24-48 hrs
- Post-streptococcal glomerulonephritis (↑ ASO, ↓ C3)
- Lupus nephritis (↑ ANA, ↓ C3/C4)
- Goodpasture syndrome (hemoptysis + microcytic anemia)
- Alport syndrome / familial nephritis (family history + sensorineural deafness)
- Thin basement membrane disease
- Membranoproliferative GN, membranous nephropathy
2. Nonglomerular Hematuria
| Feature | Finding |
|---|---|
| Urine color | Bright red / pink |
| RBC morphology | Normal (circular, isomorphic) |
| RBC casts | Absent |
| Proteinuria | Minimal (if heavy, suggests parenchymal, not urologic) |
| Clots | May be present |
a) Medical/Nonsurgical causes (renal parenchymal):
- Tubulointerstitial disease (interstitial nephritis, analgesic nephropathy)
- Papillary necrosis (diabetes, sickle cell disease/trait, analgesic abuse)
- Polycystic kidney disease
- Renal vascular disease: renal artery embolism/thrombosis, AV fistula, renal vein thrombosis, Nutcracker syndrome
- Medullary sponge kidney
- Sickle cell disease - typically unilateral, left-sided (4x more common left)
b) Surgical/Urologic causes:
- Bladder cancer - most common cause of gross hematuria in patients >50 years
- Renal cell carcinoma
- Urothelial carcinoma (ureter, renal pelvis)
- Urolithiasis (nephrolithiasis, ureteral calculi)
- Benign prostatic hyperplasia (BPH)
- Urinary tract infection (most common cause of gross hematuria in children)
- Bladder/urethral trauma
- Urethral stricture
Localization by Stream Pattern
| Pattern | Location |
|---|---|
| Initial stream hematuria | Prostatic urethra or anterior urethra |
| Total (throughout stream) | Bladder, upper tract (kidney, ureter) |
| Terminal hematuria | Bladder neck, trigone, posterior urethra |
Clot shape also helps: vermiform (worm-shaped) clots = upper tract (ureter molds the clot); cuboid clots = bladder origin.
Evaluation Flowchart (Glomerular)
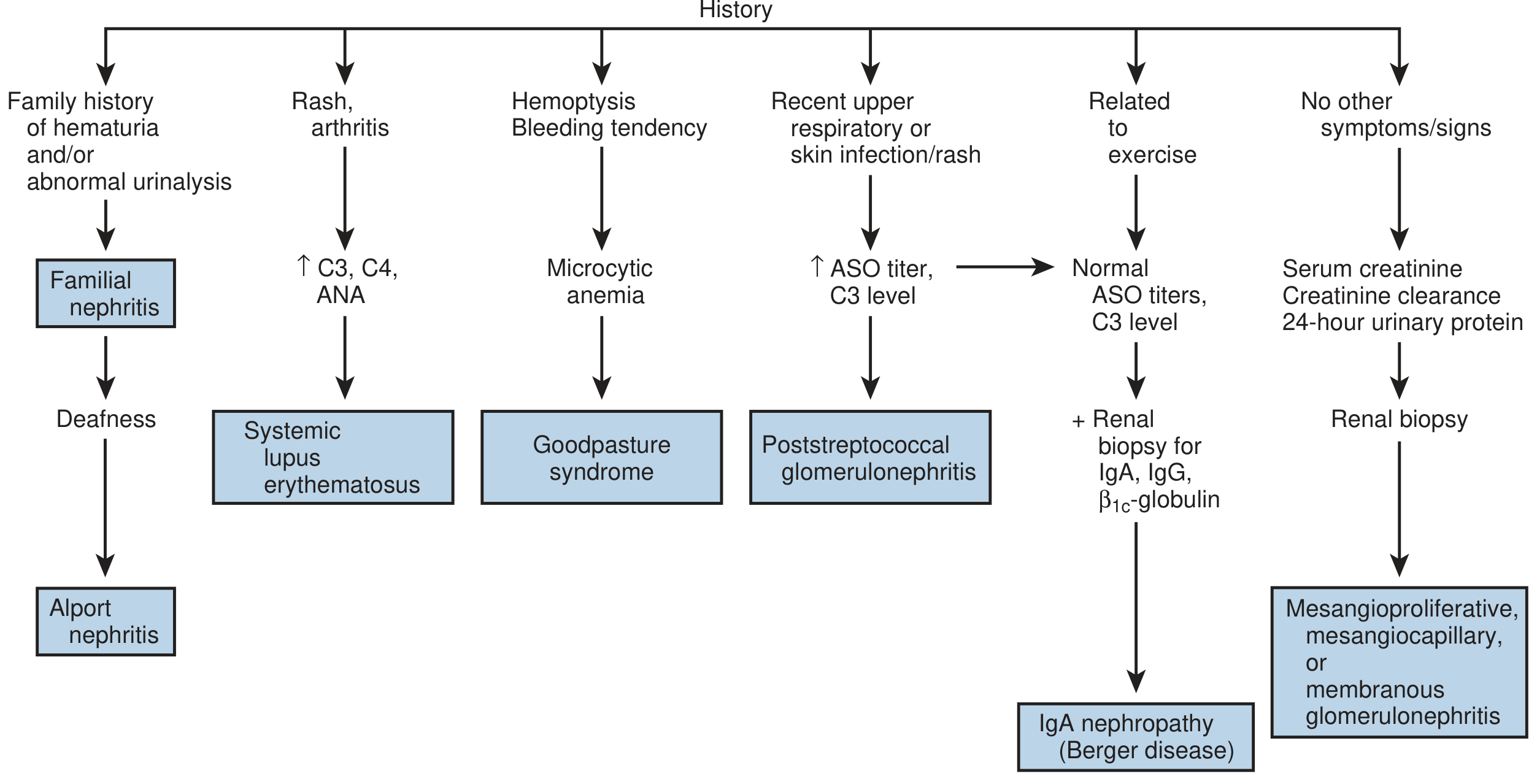
Fig. 2.1 - Evaluation of glomerular hematuria (dysmorphic erythrocytes, RBC casts, proteinuria). - Campbell-Walsh-Wein Urology
Evaluation Approach
Step 1 - Urinalysis and Microscopy
- Confirm RBCs (not pseudohematuria)
- Check RBC morphology: dysmorphic = glomerular; isomorphic = non-glomerular
- Look for RBC casts (= GN), WBCs/bacteria (= UTI), crystals (= stones)
- Quantify proteinuria
Step 2 - History and Risk Stratification
High-risk features for malignancy:
- Age >35 (especially >50)
- Smoking history
- Occupational exposure to industrial chemicals/dyes (benzidine, aniline)
- Pelvic irradiation
- Chronic cyclophosphamide exposure
- Analgesic abuse
- Chronic indwelling foreign bodies
Benign/low-risk features:
- Young woman with dysuria, frequency → UTI
- Recent vigorous exercise → exercise-induced hematuria (rule out IgA nephropathy)
- Recent URTI + hematuria → IgA nephropathy vs. post-streptococcal GN
- Family history of renal disease, deafness → Alport syndrome
- Sickle cell trait/disease + left-sided flank pain
Step 3 - Laboratory Workup
For suspected glomerular disease:
- Serum creatinine, BUN, electrolytes
- CBC, serum albumin
- C3, C4 (low in SLE, MPGN, post-strep GN)
- ANA (SLE)
- ASO / anti-DNase B titer (post-streptococcal)
- ANCA (vasculitis)
- Anti-GBM antibody (Goodpasture)
- 24-hour urine protein or urine protein:creatinine ratio
For suspected urologic/malignant cause:
- Urine cytology
- CT urogram (gold standard for upper tract evaluation)
- Cystoscopy (mandatory to exclude bladder cancer - especially in adults >35 with gross hematuria)
Step 4 - Imaging
- CT urogram (CTU): first-line for evaluating the upper urinary tract
- Renal ultrasound: useful in children, pregnant women, renal failure
- MR urography: contrast allergy, CKD, avoiding radiation
- Retrograde pyelogram: for upper tract urothelial lesions
Step 5 - Cystoscopy
Indicated in all adults with gross hematuria and adults ≥35 with asymptomatic microscopic hematuria (per AUA guidelines). Bladder cancer is the most common cause of gross hematuria in adults >50. - Campbell-Walsh-Wein Urology, p.40
Special Situations
Anticoagulation
Anticoagulation at therapeutic levels does NOT independently cause hematuria (prevalence 3.2% vs. 4.8% in controls). Urologic disease was found in 81% of anticoagulated patients with >1 episode of microscopic hematuria. Do not attribute hematuria to anticoagulant therapy - full workup is required. - Campbell-Walsh-Wein Urology
Children
Causes include UTI (most common for gross), hypercalciuria, glomerulonephritis, IgA nephropathy, urolithiasis, Wilms tumor (rare). In isolated microscopic hematuria without proteinuria, test parents for hematuria and check urinary calcium:creatinine ratio. Cystoscopy is rarely indicated in children. - Campbell-Walsh-Wein Urology, p.3003
Sickle Cell Disease
Typically unilateral, left-sided (4x more common left due to longer left renal vein course and higher venous pressure). Treatment: bed rest, high urine output, urine alkalinization. For massive/persistent bleeding: epsilon-aminocaproic acid (EACA) or tranexamic acid (use with caution given thrombotic risk). Rarely, nephrectomy. - NKF Primer on Kidney Diseases, p.412
Renal Transplant Recipients
Add BK virus to the differential. Confirm by urine cytology (viral cytopathic changes) and urine BK virus PCR titers. - Campbell-Walsh-Wein Urology
AUA Asymptomatic Microhematuria (AMH) Guidelines
AMH = ≥3 RBC/HPF on properly collected urine in the absence of an obvious benign cause (after excluding UTI, menstruation, vigorous exercise, recent urologic procedure, trauma).
After confirming true AMH:
- Renal function tests + urine protein
- Upper tract imaging (CT urogram preferred)
- Cystoscopy (in adults ≥35, or any risk factors)
- Urology/nephrology referral as appropriate
- Follow-up urinalysis if no cause found
Key Differentiating Points
| Feature | Glomerular | Non-Glomerular |
|---|---|---|
| Color | Brown/cola | Bright red |
| RBC morphology | Dysmorphic | Isomorphic |
| RBC casts | Present | Absent |
| Proteinuria | Marked | Minimal |
| Clots | Absent | May be present |
| Pain | Usually absent | Colicky (stones), suprapubic |
Sources: Campbell-Walsh-Wein Urology (3-Vol Set); Henry's Clinical Diagnosis and Management by Laboratory Methods; NKF Primer on Kidney Diseases, 8e; Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.