Hey
Hey! How can I help you today?
You are going to help in medicine
Perfect! I'm well-equipped for medical questions. I have access to a library of authoritative medical textbooks, peer-reviewed literature via PubMed, and current web sources.
I can help with:
- Diagnoses & clinical presentations - symptoms, signs, differentials
- Pharmacology - drug mechanisms, dosing, interactions, side effects
- Physiology & pathophysiology - how systems work and what goes wrong
- Anatomy - structures, relations, clinical relevance
- Procedures & investigations - labs, imaging, clinical tests
- Treatment guidelines - evidence-based management
- Exam prep - USMLE, MBBS, clinical scenarios, MCQs
Go ahead and ask your question!
Explain hiv
Reading File
Finding Sources
Searching the Web
HIV pathogenesis classification treatment overview 2025
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Let me compile it.
HIV - Human Immunodeficiency Virus
1. Overview
HIV (Human Immunodeficiency Virus) is a nontransforming human retrovirus belonging to the lentivirus family. It causes progressive destruction of cell-mediated immunity, ultimately leading to AIDS (Acquired Immunodeficiency Syndrome). There are two forms:
-
HIV-1: Most common worldwide; responsible for the global pandemic
-
HIV-2: Causes a similar but slower disease, predominantly in West Africa and India
-
Robbins & Kumar Basic Pathology, p. 199
2. Structure of HIV
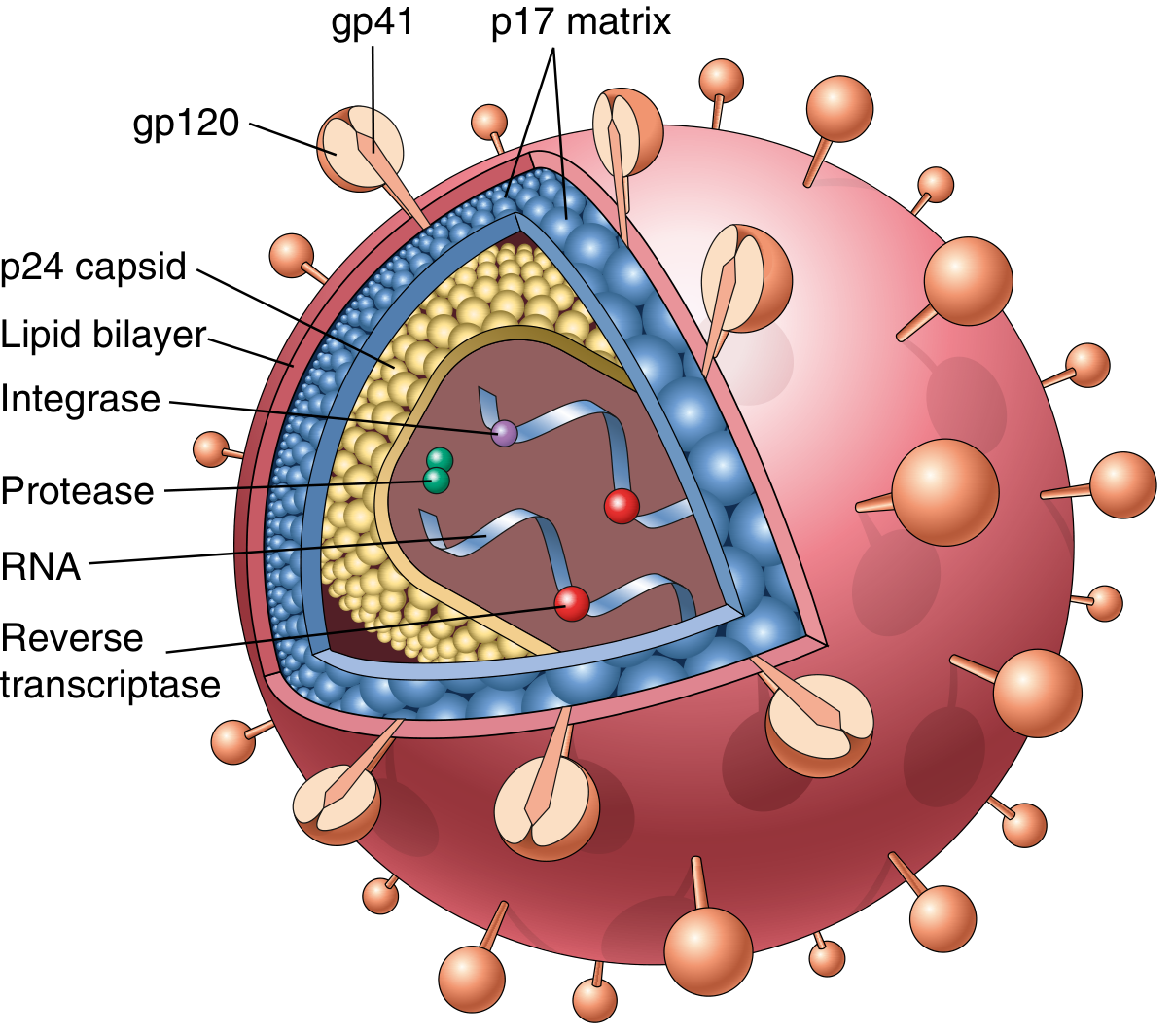
The HIV virion is spherical with a cone-shaped electron-dense core, surrounded by a host cell-derived lipid envelope.
| Component | Role |
|---|---|
| gp120 | Binds CD4 receptor on target cells |
| gp41 | Mediates membrane fusion |
| p17 | Matrix protein beneath the envelope |
| p24 | Major capsid protein; target of diagnostic assays |
| Reverse transcriptase | Converts viral RNA to proviral DNA |
| Integrase | Integrates proviral DNA into host genome |
| Protease | Cleaves precursor proteins for viral assembly |
The genome contains three core genes:
gag (nucleocapsid), pol (enzymes), and env (gp160 → gp120 + gp41), plus regulatory genes: tat, rev, vif, nef, vpr, vpu.- Robbins & Kumar Basic Pathology, p. 199
3. Transmission
| Route | Notes |
|---|---|
| Sexual contact | Most common globally; unprotected anal intercourse carries highest risk |
| Parenteral (IV drug use) | Sharing contaminated needles |
| Blood/blood products | Largely eliminated by modern screening |
| Mother-to-child | During delivery, breastfeeding; ART in pregnancy dramatically reduces this |
HIV is not transmitted by casual contact, saliva, tears, or insects.
4. Life Cycle and Pathogenesis
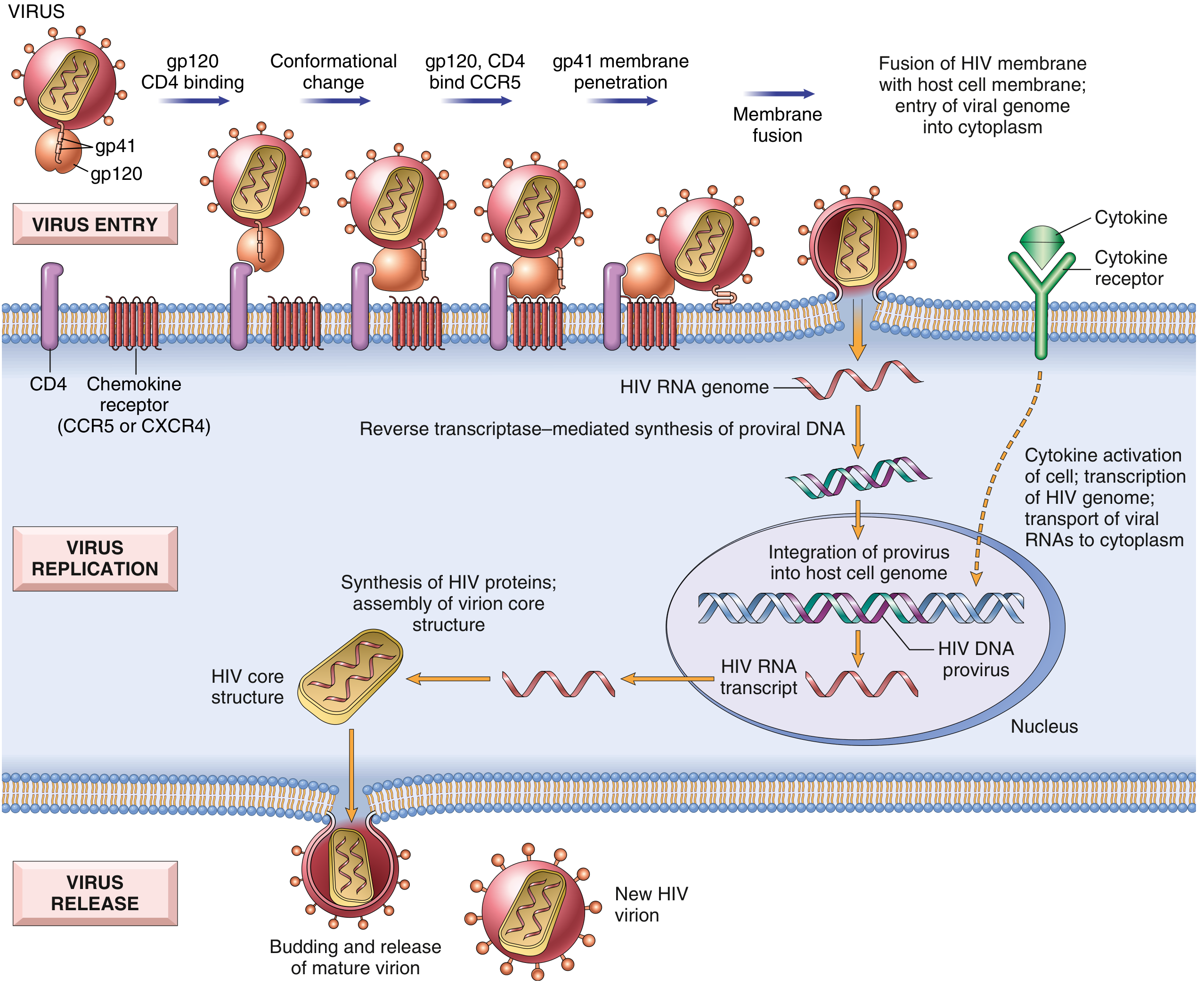
Step-by-step:
- Attachment: gp120 binds to CD4 receptor on T helper cells, macrophages, dendritic cells
- Co-receptor binding: gp120 then binds to chemokine co-receptors (CCR5 or CXCR4), causing conformational change
- Fusion: gp41 inserts fusion peptide into host cell membrane → viral genome enters cytoplasm
- Reverse transcription: Viral RNA → double-stranded proviral DNA (via reverse transcriptase)
- Integration: Proviral DNA integrates into host genome (via integrase) - can remain latent for years
- Transcription & translation: Upon activation, proviral DNA is transcribed → viral proteins synthesized
- Assembly & budding: New virions bud from host cell surface
- Maturation: Protease cleaves precursor proteins → mature, infectious virion
Co-receptor tropism:
-
R5 strains (CCR5): Infect macrophages and T cells; predominate in early infection
-
X4 strains (CXCR4): T-tropic; appear in late disease, associated with rapid CD4 decline
-
~1% of Europeans with homozygous CCR5-Δ32 mutation are resistant to HIV infection
-
Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine 22E (2025)
5. CD4+ T Cell Depletion
The hallmark of HIV is progressive loss of CD4+ T cells through:
Direct mechanisms:
- Loss of membrane integrity during viral budding
- Syncytia formation (infected + uninfected cells fuse)
- Accumulation of unintegrated viral DNA
Indirect mechanisms:
- Apoptosis, pyroptosis (caspase-1 mediated)
- Autoimmunity
- Activation-induced cell death
- Elimination of HIV-infected cells by immune responses
Normal CD4 count: ~500-1500 cells/μL. Disease progresses as CD4 falls.
- Harrison's Principles of Internal Medicine 22E (2025)
6. Clinical Stages (CDC Classification)
Stage A - Primary/Acute HIV (2-6 weeks post-infection)
- Flu-like illness: fever, lymphadenopathy, pharyngitis, rash, myalgias
- High viral load, CD4 may temporarily drop
- Self-limiting in most; some never notice it
- Also called "acute retroviral syndrome"
Stage B - Chronic Asymptomatic/Symptomatic Phase
- Can last 8-10 years without ART
- Virus replicates slowly; CD4 gradually declines
- Symptomatic stage B: oral candidiasis, hairy leukoplakia, recurrent herpes zoster, pelvic inflammatory disease, peripheral neuropathy
Stage C - AIDS
Defined by:
- CD4+ count < 200 cells/μL, OR
- Presence of an AIDS-defining illness (opportunistic infection or malignancy)
AIDS-defining illnesses include:
| Category | Examples |
|---|---|
| Fungi | PCP (Pneumocystis jirovecii pneumonia), esophageal candidiasis, cryptococcosis, histoplasmosis |
| Viruses | CMV retinitis, HSV (chronic ulcers >1 month), PML (JC virus) |
| Bacteria | Mycobacterium avium complex, disseminated TB |
| Parasites | Toxoplasmosis of brain, cryptosporidiosis |
| Malignancies | Kaposi's sarcoma, Burkitt's lymphoma, primary CNS lymphoma |
| Other | HIV encephalopathy, HIV wasting syndrome, invasive cervical cancer |
- Harrison's Principles of Internal Medicine 22E (2025), Table 208-1
7. Diagnosis
| Test | Use |
|---|---|
| 4th-generation HIV Ag/Ab combo test | Initial screening; detects p24 antigen + antibodies |
| HIV RNA (viral load) | Confirms acute infection; monitors treatment response |
| CD4+ count | Assesses immune status; guides OI prophylaxis |
| Western blot / confirmatory assay | Confirms positive screening test |
| HIV resistance genotype | Before starting ART; guides drug selection |
Target on ART: Viral load < 50 copies/mL (undetectable)
8. Treatment - Antiretroviral Therapy (ART)
ART is recommended for all people living with HIV, initiated as soon as possible after diagnosis.
Drug Classes and Targets:
| Class | Mechanism | Examples |
|---|---|---|
| NRTIs (Nucleoside RT inhibitors) | Block reverse transcription | Tenofovir (TDF/TAF), emtricitabine (FTC), lamivudine (3TC), abacavir (ABC) |
| NNRTIs (Non-nucleoside RT inhibitors) | Block RT allosterically | Efavirenz, rilpivirine, doravirine |
| INSTIs (Integrase inhibitors) | Block viral DNA integration | Dolutegravir (DTG), bictegravir (BIC), raltegravir |
| PIs (Protease inhibitors) | Block viral maturation | Darunavir, atazanavir |
| Entry/fusion inhibitors | Block gp120-CD4 binding or CCR5 | Maraviroc (CCR5 antagonist), enfuvirtide |
Preferred first-line regimens (2025):
-
Bictegravir/TAF/FTC (single pill, once daily) - preferred for most patients
-
Dolutegravir + TAF/FTC
-
Dolutegravir/lamivudine (2-drug regimen, if HIV RNA <500,000 and CD4 >200, no HBV)
-
2025 DHHS ART guidelines; Harrison's Principles of Internal Medicine 22E (2025)
9. Prevention
| Strategy | Details |
|---|---|
| PrEP (Pre-exposure prophylaxis) | Tenofovir-based regimen for high-risk individuals; >99% effective when taken correctly |
| nPEP (Nonoccupational post-exposure) | TDF/FTC + dolutegravir for 28 days; must start within 72 hours of exposure |
| Condoms | Effective barrier against sexual transmission |
| PMTCT | ART in pregnancy; cesarean before labor/membrane rupture reduces vertical transmission |
| Needle exchange programs | Reduces parenteral transmission |
| Viral suppression | Undetectable = Untransmittable (U=U) - confirmed by landmark studies |
10. Key Numbers to Remember
| Parameter | Value |
|---|---|
| Normal CD4 count | 500-1500 cells/μL |
| AIDS threshold | CD4 < 200 cells/μL |
| Start PCP prophylaxis | CD4 < 200 cells/μL |
| Start MAC prophylaxis | CD4 < 50 cells/μL |
| ART target viral load | < 50 copies/mL |
| nPEP window | Within 72 hours |
| Acute HIV window period | 2-6 weeks post-exposure |
Sources: Robbins & Kumar Basic Pathology (9th ed.), Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill), Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.