Seminar on myltibcillary leprosy
Reading File
Finding Sources
Searching PubMed
"multibacillary leprosy" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive seminar. Here is the full structured presentation:
Seminar on Multibacillary (MB) Leprosy
1. Introduction and Definition
Leprosy (Hansen's disease) is a chronic infectious disease caused by Mycobacterium leprae, an obligate intracellular pathogen. It primarily affects the peripheral nerves and skin, but can also involve the eyes, mucous membranes, muscles, bones, testes, and internal organs.
Multibacillary (MB) leprosy refers to forms of leprosy in which the bacterial load is high because the host's cell-mediated immunity (CMI) against M. leprae is weak or absent. For treatment purposes, MB leprosy is defined as:
- Ridley-Jopling classification: Lepromatous leprosy (LL), borderline lepromatous (BL), and mid-borderline (BB) with BI ≥ 2+
- WHO operational classification: ≥6 skin lesions, OR any positive skin-smear result (irrespective of lesion count)
The cardinal principle is simple: strong CMI = few organisms (paucibacillary); weak CMI = many organisms (multibacillary).
2. Etiology
| Feature | Detail |
|---|---|
| Organism | Mycobacterium leprae (Hansen's bacillus) |
| Type | Obligate intracellular; acid-fast bacillus (AFB) |
| Target cell | Schwann cells of peripheral nerves |
| Doubling time | ~12 days (very slow) |
| Culture | Cannot be grown on artificial media; grown in mouse footpad or nine-banded armadillos |
| Genome | Highly reduced (3.3 Mb); ~50% coding genes |
M. leprae uses PGL-1 (phenolic glycolipid-1) and a laminin-binding protein to invade Schwann cells and bind to the basal lamina of peripheral nerve-axon units, causing demyelination.
3. Epidemiology
Global Burden
- In 1985: 5.2 million cases worldwide; by 2019 the global burden fell to 202,185 new cases detected annually
- The South-East Asia Region (SEAR) accounts for ~71% of the global leprosy burden
- India and Indonesia together contribute 74.4% of global new cases
- ~73.4% of new cases globally are multibacillary (2019 data)
- Nine-banded armadillos (southern USA, South America) are a known animal reservoir
- Cases of new grade-2 disability: 10,813 (5.34% of new cases in 2019)
India
- Peak prevalence: 57.6 per 10,000 (1981); fell to <1 per 10,000 by December 2005 (elimination achieved at national level)
- Disease remains endemic in certain high-burden states
WHO Global Leprosy Strategy 2016-2020: Key Targets
- Zero grade-2 disability in children with new leprosy
- New cases with grade-2 disability <1 per million population
- Zero countries with discriminatory legislation against leprosy patients
Source: Community Medicine (K. Park, 9789382219163)
4. Transmission
- Route: Mainly via nasal droplets from untreated MB patients; traumatic skin inoculation is also possible
- Incubation period: 2-7 years, sometimes up to 4 decades
- Infectivity: Low - most new cases have had prolonged close contact with an infected person
- Once treated, an MB patient becomes non-infectious within 3 weeks of starting rifampicin (or after ~90 days of dapsone monotherapy)
- Attack rate among household contacts of lepromatous cases: 4.4-12% within 5 years
5. Immunopathology
The CMI response to M. leprae is the key determinant of disease type and severity:
| Feature | Tuberculoid (TT/BT) - Paucibacillary | Lepromatous (LL/BL) - Multibacillary |
|---|---|---|
| CMI to M. leprae | Strong | Absent/weak |
| Th1 response | Present (IL-2, IFN-γ) | Absent |
| CD4+ T cells in lesions | Abundant | Sparse (few CD8+ cells dominate) |
| Bacterial load | Very low | Very high |
| Granuloma formation | Well-formed, epithelioid | Absent; foamy macrophages |
| Lepromin test | Strongly positive | Negative |
| Humoral antibody | Low | High (anti-PGL-1) |
| Nerve damage | Focal, asymmetric | Bilateral, symmetric, slow |
In lepromatous leprosy, foamy macrophages (Virchow cells) are loaded with organisms (globi). The absence of Th1 cytokines allows unrestrained bacterial multiplication.
Source: Microbiology (Jawetz, 9781260464283); Dermatology (Habif, 9780323547536)
6. Classification
Ridley-Jopling Classification (Research/Detailed)
| Type | Abbreviation | Bacterial Index | Lesions | CMI |
|---|---|---|---|---|
| Polar tuberculoid | TT | 0 | 1-2, large, defined | +++ |
| Borderline tuberculoid | BT | 0-1+ | <5, defined | ++ |
| Mid-borderline | BB | 2-3+ | Multiple, "punched-out" | + |
| Borderline lepromatous | BL | 3-4+ | Multiple, asymmetric | +/- |
| Polar lepromatous | LL | 5-6+ | Numerous, symmetric, diffuse | 0 |
BB, BL, and LL = MULTIBACILLARY
Borderline disease is unstable and tends to "downgrade" (shift toward LL) over time without treatment.
WHO Operational Classification (Field Use)
- Paucibacillary (PB): <6 skin lesions, smear negative
- Multibacillary (MB): ≥6 skin lesions, OR any smear-positive result
7. Clinical Features of Multibacillary Leprosy
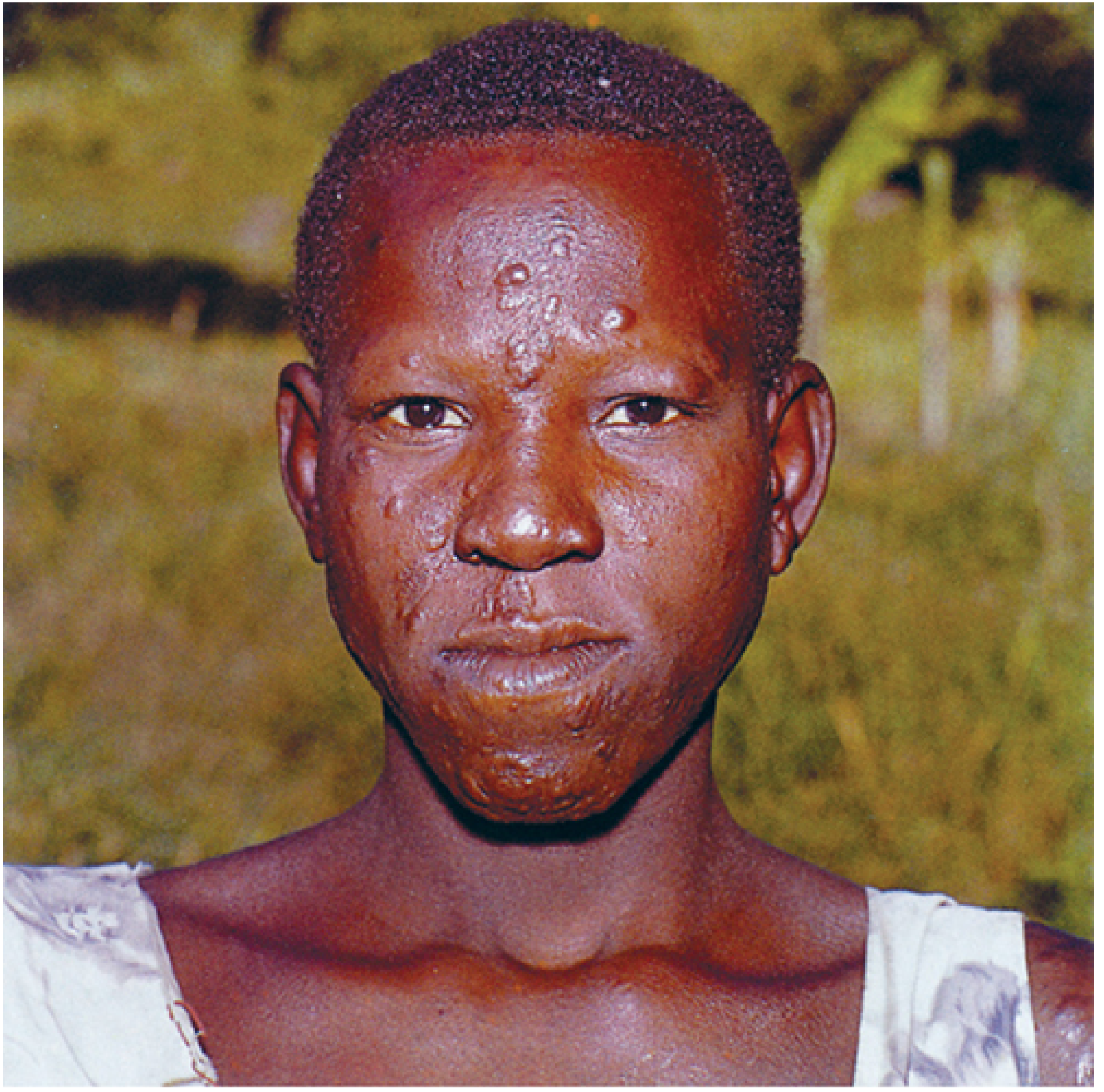
7a. Lepromatous Leprosy (LL) - The Prototype of MB Disease
Skin:
- Multiple, small, poorly defined, hypopigmented or erythematous macules - numerous and symmetrically distributed
- Minimal or no loss of sensation over early macular lesions
- Progressive diffuse infiltration of skin - especially forehead, lips, and ears giving a "leonine facies" (lion-like appearance)
- Madarosis: Loss of lateral third of eyebrows, then eyelashes, then body hair (scalp hair spared)
- Lepromas: Nodules on ear lobes, brow, nose, chin, elbows, knees
- Skin has a waxy, shiny "varnished" appearance
- No change in sweating initially
Nerves:
- Nerve involvement is bilateral and symmetric ("stocking-glove" distribution)
- Develops slowly; can be mistaken for diabetic neuropathy
- Peripheral neuropathy leading to deformity and non-healing plantar ulcers
Systemic involvement:
- Nasal: obstruction, epistaxis, collapse of nasal septum ("saddle nose")
- Eyes: lagophthalmos, corneal anesthesia, iritis, blindness
- Testes: atrophy, gynecomastia, infertility
- Reticuloendothelial system involvement
- Loss of nasal bones, sometimes digits
7b. Histoid Leprosy (Variant of MB)
- Uncommon form of MB Hansen disease
- Large, yellow-red, shiny papules and nodules in dermis or subcutaneous tissue
- Lesions on a background of normal skin (distinct from LL where background skin is abnormal)
- Size 1-15 mm; favor buttocks, lower back, face, bony prominences
- Can resemble molluscum contagiosum
- Mostly described in patients with dapsone resistance or relapse after inadequate treatment
- Very high bacillary load; BI often 6+
7c. Diffuse Leprosy of Lucio (DLL)
- Striking variant seen mainly in western Mexico and parts of Latin America
- Diffuse lepromatous infiltration without discrete lepromas
- Complicated by Lucio phenomenon (erythema necroticans): ischemic vasculitic ulcers due to endothelial invasion
8. Nerve Involvement
The peripheral nerves most commonly enlarged/damaged in leprosy:
| Nerve | Common Manifestation |
|---|---|
| Ulnar nerve (at elbow) | Claw hand (ring and little fingers) |
| Median nerve (at wrist) | Claw hand (index and middle fingers) |
| Common peroneal nerve (at knee) | Foot drop |
| Posterior tibial nerve (at ankle) | Plantar anesthesia, claw toes |
| Radial cutaneous nerve | Wrist drop |
| Facial nerve | Lagophthalmos |
| Greater auricular nerve | Visible/palpable enlarged nerve at neck |
| Supraorbital nerve | Anesthesia of forehead |
In MB leprosy, nerve damage is bilateral, symmetric, and insidious. The feet develop midfoot disintegration, forefoot-hindfoot separation, and pressure ulcers.
Source: Internal Medicine (Firestein, 9780702081330)
9. Diagnosis
Clinical
- ≥6 hypopigmented/erythematous skin lesions with loss of sensation or altered sweating
- Thickened, palpable peripheral nerves
- Positive skin smear for AFB
Bacteriological
- Slit-skin smear (ear lobes, nasal septum, affected skin edges): Stained with modified Ziehl-Neelsen (Fite-Faraco stain - weaker decolorizer than standard AFB, since M. leprae is more sensitive)
- Bacterial Index (BI): Logarithmic scale 0-6+ (Ridley's log scale)
- Morphological Index (MI): Percentage of solid-staining (viable) bacilli
Histopathology
- Skin biopsy: In LL - foamy macrophages (Virchow cells) stuffed with bacilli; no formed granulomas; "Grenz zone" (clear zone between epidermis and infiltrate)
- In TT/BT - well-formed epithelioid granulomas with giant cells and lymphocytes; few or no AFB
Serology
- Anti-PGL-1 antibody (ELISA): Elevated in MB leprosy (correlates with bacillary load); useful for monitoring
Lepromin (Mitsuda) Test
- Intradermal injection of killed M. leprae antigen
- Positive (induration >5 mm at 3-4 weeks): TT and BT leprosy
- Negative: LL leprosy
- This test assesses CMI, NOT diagnosis of infection
PCR
- Detects M. leprae DNA; useful in pure neural leprosy and smear-negative cases
10. Leprosy Reactions (Medical Emergencies)
Reactions are acute inflammatory episodes that can occur before, during, or after treatment and represent the leading cause of nerve damage.
Type 1 Reaction (Reversal Reaction)
| Feature | Detail |
|---|---|
| Mechanism | Enhanced CMI response (Th1 upregulation) to M. leprae antigens |
| Occurs in | Borderline leprosy (BT, BB, BL) - most severe in BL |
| Timing | Usually after starting MDT |
| Skin | Existing lesions become swollen, erythematous, tender - can ulcerate |
| Nerves | Acute neuritis = Emergency - sudden loss of nerve function, permanent damage if untreated |
| Systemic symptoms | None (no fever, no chills) |
| Histology | Perivascular/perineural edema, lymphocytes; reduced bacilli |
| Treatment | Prednisolone 40-60 mg/day, taper over 3-6 months; DO NOT stop MDT |
Type 2 Reaction (Erythema Nodosum Leprosum - ENL)
| Feature | Detail |
|---|---|
| Mechanism | Immune complex-mediated vasculitis + elevated TNF-α |
| Occurs in | BL and LL leprosy (~50% of patients) |
| Timing | 90% within first few years of MDT; also in pregnancy |
| Skin | Tender erythematous nodules (distinct new lesions, not pre-existing) |
| Systemic | Fever, malaise, myalgias, arthralgia, iritis, orchitis, lymphadenopathy, proteinuria |
| Nerves | Nerve damage via membrane attack complex generation |
| Treatment | Thalidomide (drug of choice, especially for chronic recurrent ENL); Prednisolone; clofazimine in high dose |
| Note | Thalidomide contraindicated in women of childbearing age (teratogenic) |
Lucio Phenomenon (Type 3 Reaction)
- Occurs only in Diffuse Leprosy of Lucio
- Ischemic vasculitis - hemorrhagic ulcers
- Systemic toxicity; potentially fatal
11. Deformities and Disabilities
WHO Disability Grading:
| Grade | Hands/Feet | Eyes |
|---|---|---|
| 0 | No impairment | No impairment |
| 1 | Anesthesia, no visible deformity | Anesthesia; no visible impairment |
| 2 | Visible deformity (claw hand, foot drop, ulcer) | Severe visual impairment (VA <6/60) |
Specific deformities in MB leprosy:
- Clawing of fingers (ulnar, median nerve)
- Wrist drop (radial nerve)
- Foot drop (common peroneal nerve)
- Plantar ulcers (posterior tibial nerve)
- Lagophthalmos - corneal ulceration - blindness
- Saddle nose (nasal bone/septal destruction)
- Gynecomastia (testicular atrophy)
- Absorption of phalanges (auto-amputation)
12. Treatment - WHO Multidrug Therapy (MDT)
MDT was introduced by WHO in 1981 to prevent drug resistance (particularly to dapsone monotherapy) and achieve cure.
WHO MDT Regimen for Multibacillary Leprosy (Adults)
| Drug | Dose | Frequency |
|---|---|---|
| Rifampicin 600 mg | Supervised | Monthly |
| Clofazimine 300 mg | Supervised | Monthly |
| Clofazimine 50 mg | Self-administered | Daily |
| Dapsone 100 mg | Self-administered | Daily |
Duration: 12 months (previously 24 months; reduced by WHO in 1998)
Pediatric Dosing (MB, age 10-14 years)
- Rifampicin: 450 mg/month (supervised)
- Clofazimine: 150 mg/month (supervised) + 50 mg alternate days
- Dapsone: 50 mg/day
Mechanism of Action of Each Drug
| Drug | Mechanism |
|---|---|
| Rifampicin | Inhibits DNA-dependent RNA polymerase; bactericidal; most potent anti-leprosy drug |
| Dapsone | Inhibits dihydropteroate synthase (like sulfonamides); bacteriostatic |
| Clofazimine | Binds DNA; generates ROS in macrophages; bactericidal + anti-inflammatory |
Key Points on MDT
- MDT renders patients non-infectious within 3 weeks (rifampicin effect)
- Blister packs provided free of charge by WHO globally
- Relapse rate after MB-MDT: very low (<1% over 9 years)
- No documented clinically significant drug resistance to rifampicin with MDT regimens
Alternative/Second-Line Drugs (for drug intolerance/resistance)
- Ofloxacin/Moxifloxacin (fluoroquinolones)
- Minocycline (tetracycline)
- ROM regimen (Rifampicin + Ofloxacin + Minocycline): single dose for single-lesion PB leprosy
Reactions During MDT
- Continue MDT - never stop for reactions
- Add prednisolone for Type 1 / ENL
- Thalidomide for chronic ENL (adults, non-childbearing)
- Increase clofazimine for chronic ENL (anti-inflammatory effect)
13. Prevention and Control
| Measure | Details |
|---|---|
| MDT | Cornerstone of control; renders patient non-infectious rapidly |
| BCG vaccination | Provides 50-80% protection against leprosy (especially tuberculoid forms); recommended in endemic areas |
| Contact examination | All household contacts of MB cases should be examined annually for 5 years |
| Chemoprophylaxis | Single-dose rifampicin (SDR) for contacts reduces new cases by ~57% (Post-Exposure Prophylaxis for Leprosy - PEP) |
| Health education | Reduces stigma; promotes early case detection |
| Disability prevention | Self-care of anesthetic hands/feet; footwear; physiotherapy |
14. Prognosis
- MB leprosy is curable with complete MDT
- Nerve damage present at diagnosis may partially recover but permanent disability can remain
- Deformities that have developed do not reverse with MDT - surgical rehabilitation may be needed
- Relapse after completing MDT is rare but possible (especially histoid leprosy)
- Leprosy is NOT a death sentence - stigma is the greatest barrier to care-seeking
15. Summary
| Feature | Multibacillary Leprosy |
|---|---|
| Types (R-J) | BB, BL, LL |
| WHO field criterion | ≥6 lesions or smear positive |
| Key immunology | Absent CMI, Th2 dominance, foamy macrophages |
| Bacterial index | 2+ to 6+ |
| Lesions | Multiple, symmetric, poorly defined |
| Nerves | Bilateral, symmetric, slow damage |
| Lepromin | Negative |
| Reactions | Type 1 (reversal) in BL; Type 2 (ENL) in BL/LL |
| Treatment | Rifampicin + Clofazimine + Dapsone × 12 months |
| Global proportion | ~73% of all new leprosy cases |
Sources:
- Dermatology - Habif's Clinical Dermatology (9780323547536)
- Microbiology - Jawetz, Melnick & Adelberg (9781260464283)
- Community Medicine - K. Park (9789382219163)
- Internal Medicine - Firestein et al. (9780702081330)
Pharmacology seminar ??
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive, multi-source pharmacology data. Here is the full seminar:
Pharmacology Seminar: Anti-Leprosy Drugs
1. Introduction
Leprosy is caused by Mycobacterium leprae, an obligate intracellular pathogen. Because M. leprae cannot be cultured on artificial media and has an extremely slow doubling time (~12 days), pharmacological management of leprosy required the development of specific long-course regimens. Dapsone monotherapy, introduced in the 1940s, led to widespread drug resistance by the 1970s, prompting WHO to introduce Multidrug Therapy (MDT) in 1981.
MDT combines three drugs: Rifampicin + Dapsone + Clofazimine. This combination:
- Prevents emergence of resistance
- Kills organisms at multiple targets
- Renders the patient non-infectious within 3 weeks
"Only bactericidal drugs are used in multidrug regimens" - K. Park's Community Medicine
2. Classification of Anti-Leprosy Drugs
First-Line (WHO MDT Drugs)
| Drug | Bactericidal/Static | Class |
|---|---|---|
| Rifampicin | Bactericidal (most potent) | Rifamycin |
| Clofazimine | Bactericidal + anti-inflammatory | Riminophenazine dye |
| Dapsone | Weakly bactericidal / bacteriostatic | Sulfone |
Second-Line (for drug intolerance or resistance)
| Drug | Class |
|---|---|
| Ofloxacin / Levofloxacin / Moxifloxacin | Fluoroquinolones |
| Minocycline | Tetracycline |
| Clarithromycin | Macrolide |
Drugs for Reactions (not directly anti-mycobacterial)
| Drug | Use |
|---|---|
| Prednisolone | Type 1 (reversal) reaction; also ENL |
| Thalidomide | Type 2 reaction (ENL) - drug of choice |
| Clofazimine (high dose) | Chronic recurrent ENL |
3. Drug 1: Dapsone (DDS - Diaminodiphenyl Sulfone)
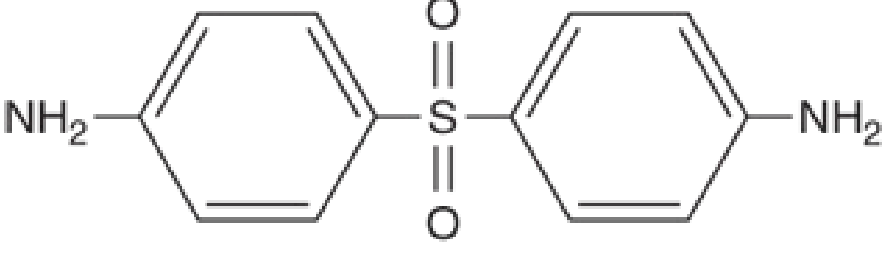
Chemistry
- Diaminodiphenylsulfone (DDS)
- Structurally related to sulfonamides
- Available in 25 mg and 100 mg tablets
Mechanism of Action
- Competitive inhibitor of dihydropteroate synthase (DHPS) in the folate synthesis pathway - the same enzyme inhibited by sulfonamides
- Prevents synthesis of dihydrofolic acid, blocking bacterial DNA synthesis
- Bacteriostatic against M. leprae at normal doses; weakly bactericidal at higher doses
- Active metabolite dapsone hydroxylamine (DDS-NOH) contributes to anti-inflammatory effects (inhibits neutrophil chemotaxis, oxidative burst) - this is the basis of its use in non-infectious dermatoses
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Well absorbed from GI tract; peak levels in 2-6 hours |
| Distribution | Widely distributed; high concentrations in skin (heavily infected skin has several times more drug) |
| Protein binding | ~70-90% |
| Metabolism | Hepatic: N-acetylation (polymorphic - slow/fast acetylators, but clinically irrelevant for dosing) + N-hydroxylation by CYP2C19, 3A4, 2C9 → dapsone hydroxylamine (toxic metabolite) |
| Half-life | ~28-30 hours (enterohepatic recirculation prolongs this) |
| Excretion | Bile (enterohepatic circulation); urine - mostly acetylated form |
| Note | Excreted in breast milk - risk of hemolysis in nursing infants |
Dosage
- Leprosy (adults): 100 mg/day orally (self-administered daily in MDT)
- Pediatric: ~1-2 mg/kg/day (50 mg/day for ages 10-14)
- Dose adjustment needed in renal failure
- Starting dose: 50-100 mg/day to minimize hemolysis
Adverse Effects
1. Hematological (Most Important)
| Effect | Mechanism | Notes |
|---|---|---|
| Hemolytic anemia | Dapsone hydroxylamine causes oxidant stress on RBCs, denaturing hemoglobin (Heinz body formation) | Most common side effect - ~20% of patients; dose-related; much worse in G6PD deficiency |
| Methemoglobinemia | Dapsone hydroxylamine oxidizes Hb-Fe²⁺ to Hb-Fe³⁺ (methemoglobin) | Usually subclinical; severe in NADH-methemoglobin reductase deficiency |
| Agranulocytosis | Idiosyncratic | Rare but life-threatening |
| Aplastic anemia | Idiosyncratic | Rare |
Key point: G6PD screening should be done before starting dapsone. Dapsone hydroxylamine is the toxic metabolite responsible for hemolysis, methemoglobinemia, and hepatotoxicity. It is reduced back to dapsone by methemoglobin reductase and cytochrome b₅ reductase in erythrocytes.
2. Dapsone Hypersensitivity Syndrome (DDS Syndrome)
- Rare but potentially fatal idiosyncratic reaction
- Features: fever + exfoliative dermatitis/rash + hepatitis + lymphadenopathy + hemolysis (maculopapular rash + enlarged lymph glands)
- Onset: usually 6-8 weeks after starting dapsone
- Must be distinguished from leprosy reactions
3. Hepatic
- Toxic hepatitis, cholestatic jaundice, transaminitis
4. Neurological
- Peripheral neuropathy (rare)
- Psychosis (rare)
5. Dermatological
- Rash, pruritus, photosensitivity
6. Life-threatening adverse effects (summary)
- Dapsone hypersensitivity syndrome
- Hemolysis (can be severe in G6PD deficiency)
- Methemoglobinemia
- Agranulocytosis
- Aplastic anemia
- Hemophagocytic syndrome
- TEN / Stevens-Johnson syndrome
Drug Interactions
- Rifampicin (CYP450 inducer) reduces dapsone levels by ~50% - but still effective
- Probenecid reduces renal excretion of dapsone - increases plasma levels
- Trimethoprim increases dapsone levels (competition for metabolism)
- Activated charcoal is useful in overdose (interrupts enterohepatic recirculation)
Contraindications
- Severe G6PD deficiency (relative - use with caution)
- Severe anemia (Hb <60% is a caution per Indian guidelines)
- Dapsone hypersensitivity
Non-Leprosy Uses of Dapsone
Dapsone has broad utility as an anti-inflammatory drug in dermatology via DDS-NOH-mediated inhibition of neutrophil function:
As anti-infective:
- PCP (Pneumocystis jirovecii pneumonia) - treatment + prophylaxis in HIV
- Malaria (combination with pyrimethamine)
- Leishmaniasis, nocardiosis
As anti-inflammatory (dermatology):
- Dermatitis herpetiformis (highly responsive, hallmark indication)
- Linear IgA dermatosis
- Erythema elevatum diutinum
- Bullous SLE, bullous pemphigoid
- Pyoderma gangrenosum, Sweet syndrome
- Subcorneal pustular dermatosis
Topical Dapsone (5% and 7.5% gel):
- FDA-approved for acne vulgaris
- No systemic hemolysis even in G6PD-deficient patients
- Safe for topical use without G6PD pre-testing
Sources: Fitzpatrick's Dermatology; Katzung Pharmacology; Lippincott Pharmacology; Community Medicine (K. Park)
4. Drug 2: Rifampicin (Rifampin)
Chemistry
- Semisynthetic derivative of rifamycin B (produced by Amycolatopsis rifamycinica)
- Macrocyclic antibiotic; large complex structure
Mechanism of Action
- Inhibits DNA-dependent RNA polymerase (DDRP) - specifically the β-subunit (encoded by rpoB gene)
- Blocks initiation of RNA synthesis, NOT elongation
- Bactericidal - most potent drug against M. leprae
- A single dose of 1500 mg or 3-4 daily doses of 600 mg kills 99% of viable organisms
- Effective even when given at monthly intervals - a major clinical advantage
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Well absorbed orally; reduced by food |
| Distribution | Widely distributed; penetrates cells, CSF, abscesses |
| Metabolism | Hepatic; auto-induction of CYP450 enzymes (self-accelerating metabolism) |
| Half-life | ~3.5 hours (but effective in monthly dosing due to concentration-dependent killing) |
| Excretion | Primarily bile/feces; some renal |
| Characteristic | Turns body fluids orange-red (urine, tears, sweat, saliva, sputum) - harmless but important to warn patients |
Dosage in MDT
- Adults: 600 mg once monthly, supervised (to ensure ingestion)
- Children (10-14 yrs): 450 mg once monthly
- Monthly dosing exploits rifampicin's bactericidal concentration-dependent killing of M. leprae
Adverse Effects
- Hepatotoxicity - most serious; monitor LFTs
- Flu-like syndrome (fever, chills, myalgias) - especially with intermittent dosing
- Rash, urticaria
- Thrombocytopenia, hemolytic anemia (intermittent high-dose)
- Nephritis (rare)
- Cholestasis
- GI upset (nausea, vomiting, abdominal pain) - anorexia
- Shock and collapse reported in rare cases (monitor for 1 hour post-dose)
Drug Interactions (Critical - Major Enzyme Inducer)
Rifampicin is a potent inducer of CYP450 enzymes (CYP3A4, CYP2C9, CYP2C19, P-glycoprotein):
- Reduces levels of: oral contraceptives (risk of unintended pregnancy), warfarin, corticosteroids, antiretrovirals, antifungals, calcium channel blockers, anticonvulsants
- Clinical implication: patients on rifampicin-containing MDT may need alternative contraception
Resistance
- Resistance develops rapidly if used as monotherapy
- rpoB gene mutations → rifampicin-resistant strains
- MDT prevents resistance by combining with dapsone and clofazimine
5. Drug 3: Clofazimine
Chemistry
- Fat-soluble riminophenazine dye - appears as red-orange/brick-red crystals
- Originally synthesized in 1954 as a potential anti-TB drug; licensed for leprosy in 1969
- Also has current roles in MDR-TB (WHO Group A drug) and NTM infections
Mechanism of Action (Multifactorial)
- Membrane disruption - directly damages mycobacterial cell membrane
- Inhibition of mycobacterial phospholipase A2
- Inhibition of microbial K⁺ transport
- Generation of hydrogen peroxide and cytotoxic ROS (redox cycling)
- Interference with bacterial electron transport chain
- Efflux pump inhibition
- Anti-inflammatory effects: inhibits macrophages, T cells, neutrophils, and complement
The dual bactericidal + anti-inflammatory action is unique and makes it valuable for preventing/suppressing ENL reactions.
"ENL may not develop in patients treated with clofazimine" - Lippincott Pharmacology
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Oral; bioavailability 45-60% (increased 2-fold by high-fat meals; decreased by antacids) |
| Distribution | Extremely lipophilic; huge volume of distribution (~10,000 L); accumulates in reticuloendothelial tissues, skin, intestinal mucosa, mesenteric lymph nodes, body fat; does NOT enter CNS |
| Metabolism | Hepatic: hydrolytic dehalogenation, deamination, glucuronidation, hydroxylation |
| Half-life | ~35 days with sustained dosing (due to tissue accumulation and slow release) - this permits intermittent monthly dosing |
| Excretion | Primarily feces; drug crystals visible inside phagocytic cells at autopsy |
| Crystals | Crystalline deposits found in intestinal mucosa, liver, spleen, lymph nodes at autopsy |
Dosage in MDT
- Adults: 300 mg once monthly (supervised) + 50 mg daily (self-administered)
- Children (10-14 yrs): 150 mg monthly + 50 mg on alternate days
- For ENL: clofazimine 100-200 mg/day (anti-inflammatory dose)
Adverse Effects
| Effect | Details |
|---|---|
| Skin discoloration | Most prominent; pink → reddish-brown → brownish-black (dose-dependent); also affects conjunctivae, urine, sputum, sweat. Fades in 6-12 months after stopping; traces may persist up to 4 years |
| Ichthyosis | Dry, scaly skin particularly on shins and forearms |
| GI effects | 40-50% of patients; cramps, diarrhea, nausea, weight loss; due to crystal deposition in small bowel wall; rarely requires surgery |
| QT prolongation | ECG monitoring warranted, especially when combined with other QT-prolonging drugs |
| Psychosocial distress | Skin discoloration socially disabling in many patients; major cause of non-adherence (inadvertently "outs" patients as leprosy patients) |
Important warning: Abdominal pain in a patient on clofazimine should raise suspicion of intestinal crystal deposition (enteritis/obstruction). Crystal deposition has been found in multiple organs at autopsy.
Drug Interactions
- Anti-inflammatory effects of clofazimine may be inhibited by dapsone (potential pharmacodynamic antagonism)
- Antacids reduce clofazimine absorption by ~30%
Resistance
- Associated with mutations in Rv0678 (repressor of mmpS5-mmpL5 efflux pump) - cross-resistance with bedaquiline
- Mutations in pepQ and Rv1979c also involved
6. WHO MDT Regimen Summary
Multibacillary Leprosy (Adults) - 12 months
| Drug | Monthly (Supervised) | Daily (Self-administered) |
|---|---|---|
| Rifampicin | 600 mg | - |
| Clofazimine | 300 mg | 50 mg |
| Dapsone | - | 100 mg |
Paucibacillary Leprosy (Adults) - 6 months
| Drug | Monthly (Supervised) | Daily (Self-administered) |
|---|---|---|
| Rifampicin | 600 mg | - |
| Dapsone | - | 100 mg |
(Clofazimine is NOT used in PB leprosy due to psychosocial concerns about skin discoloration for a relatively mild/limited disease)
Key Operational Features of MDT
- Blister pack system - each pack contains all drugs for one month, provided free of charge by WHO
- Supervised monthly administration ensures at least one dose is witnessed
- Non-infectious within 3 weeks of starting (rifampicin effect)
- Cure rate: ~99%
- Relapse rate: <1% (except in patients with BI ≥4 at start, where relapse can reach 4-7 per 100 person-years)
7. Second-Line Anti-Leprosy Drugs
Used when patients are intolerant to first-line drugs or when drug resistance (especially rifampicin resistance) is confirmed.
Fluoroquinolones
| Drug | Dose | Notes |
|---|---|---|
| Ofloxacin | 400 mg/day | Most studied; inhibits DNA gyrase + topoisomerase IV |
| Levofloxacin | Standard dose | Active isomer of ofloxacin |
| Moxifloxacin | Standard dose | More potent; shorter course possible (ROM regimen) |
ROM regimen (single-dose for single-lesion PB leprosy): Rifampicin 600 mg + Ofloxacin 400 mg + Minocycline 100 mg (single dose)
Minocycline
- Tetracycline antibiotic
- Inhibits 30S ribosomal subunit (protein synthesis inhibitor)
- Bactericidal against M. leprae
- Clearance of bacilli from skin was faster than dapsone or clofazimine, similar to ofloxacin
- Dose: 100 mg/day
- May shorten duration of MB-MDT if added to regimen
Clarithromycin
- Macrolide; inhibits 50S ribosomal subunit
- Active against M. leprae
- Used in combination for rifampicin-resistant leprosy
For Rifampicin-Resistant Leprosy (WHO Guidelines)
Phase 1 (6 months): At least 2 second-line drugs (clarithromycin, minocycline, or a quinolone) + clofazimine daily
Phase 2 (18 months): Clofazimine + one second-line drug daily
For rifampicin AND ofloxacin dual resistance: Clarithromycin + minocycline + clofazimine for 6 months, then clarithromycin or minocycline + clofazimine for 18 months
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025)
8. Drugs for Leprosy Reactions
Thalidomide (for ENL - Type 2 Reaction)
| Feature | Detail |
|---|---|
| History | Withdrawn in 1961 for severe teratogenicity (phocomelia); later found effective in ENL; FDA re-approved for ENL in 1998 |
| Classification | Orphan drug (FDA) |
| Mechanism | Inhibits TNF-α production; immunomodulatory effects on T cells and cytokines (IL-12, IFN-γ); anti-angiogenic |
| Indication | Moderate-to-severe ENL (acute and maintenance); first-line drug for ENL |
| Dose | 100-300 mg/day |
| Toxicities | Teratogenic (absolute contraindication in pregnancy - phocomelia, limb defects); peripheral neuropathy; sedation; constipation; DVT; thromboembolic events |
| Prescribing | Must be used under strict REMS program (STEPS program in USA); mandatory contraception for women of childbearing potential |
Corticosteroids (for Type 1 Reversal Reaction and ENL)
- Prednisolone 40-60 mg/day, tapered over 3-6 months
- Mandatory for reversal reactions with neuritis (nerve function emergency)
- Also used in ENL when thalidomide is contraindicated (e.g., women of childbearing age)
- MDT must NEVER be stopped when treating reactions
Clofazimine (High Dose for Chronic ENL)
- 100-200 mg/day
- Anti-inflammatory effect takes 4-6 weeks to manifest
- Used as a steroid-sparing agent in chronic recurrent ENL
9. Rationale for Combination Therapy (MDT)
| Principle | Explanation |
|---|---|
| Prevention of resistance | Each drug targets a different bacterial pathway; the probability of spontaneous resistance to all three simultaneously is negligible |
| Complementary killing | Rifampicin kills proliferating organisms; dapsone blocks folate; clofazimine attacks dormant/intracellular bacilli |
| Shortened duration | Triple therapy allows cure in 12 months vs. years with dapsone monotherapy |
| Preventing ENL | Clofazimine's anti-inflammatory component suppresses the immune complex reactions |
| Compliance | Blister packs, monthly supervision, and free provision enhance adherence |
10. Drug Comparison Table
| Feature | Rifampicin | Dapsone | Clofazimine |
|---|---|---|---|
| Class | Rifamycin | Sulfone | Riminophenazine dye |
| Bactericidal? | Yes (most potent) | Weakly bactericidal / bacteriostatic | Yes |
| Target | RNA polymerase (rpoB) | Dihydropteroate synthase (DHPS) | Membrane + electron transport + K⁺ transport + ROS |
| Anti-inflammatory? | No | No (but DDS-NOH inhibits neutrophils) | Yes (major feature) |
| Half-life | ~3.5 h (short, but effective monthly) | ~28-30 h | ~35 days |
| Skin pigmentation | Turns fluids orange | None | Red-brown discoloration |
| Dosing in MDT | 600 mg monthly (supervised) | 100 mg daily | 300 mg monthly + 50 mg daily |
| Key toxicity | Hepatotoxicity; CYP450 induction | Hemolysis; methemoglobinemia | Skin discoloration; GI toxicity; QT prolongation |
| G6PD concern | No | Yes (major) | No |
| CNS penetration | Yes | Yes | No |
| Use in ENL | No direct role | Dapsone itself can trigger ENL | Suppresses ENL (key benefit) |
11. Special Populations
| Population | Considerations |
|---|---|
| Pregnancy | MDT is safe; dapsone - no proven teratogenicity (Category C); thalidomide absolutely contraindicated; clofazimine - crosses placenta, neonatal discoloration possible |
| G6PD deficiency | Screen before dapsone; severe hemolysis risk; substitute dapsone with clofazimine if necessary |
| Renal failure | Reduce dapsone dose; rifampicin and clofazimine are primarily hepatically/biliary excreted - relatively safer |
| Children | Weight-based dosing; same 3-drug MDT for MB disease |
| HIV co-infection | MDT can be given; rifampicin interactions with antiretrovirals must be managed carefully |
12. Monitoring During MDT
| Drug | Monitoring Parameter |
|---|---|
| Dapsone | CBC (hemolysis), LFTs, G6PD screen pre-treatment |
| Rifampicin | LFTs, CBC, urine color warning |
| Clofazimine | Skin color counseling, GI symptoms, ECG (QT) |
| All drugs | Skin smear (BI) every 6 months, disability grading |
13. Summary: Key Points for Exams
- Most potent anti-leprosy drug: Rifampicin (bactericidal; kills 99% organisms with 3-4 doses)
- Drug of choice for ENL: Thalidomide (FDA approved 1998 for ENL)
- Most common adverse effect of dapsone: Hemolytic anemia (dose-related; worst in G6PD deficiency)
- Toxic metabolite of dapsone: Dapsone hydroxylamine (DDS-NOH) - causes hemolysis + methemoglobinemia
- Why clofazimine is given in MB leprosy but NOT PB: To prevent ENL reactions (its anti-inflammatory property)
- Half-life of clofazimine: ~35 days (extremely long due to tissue accumulation)
- ROM regimen: Single-dose Rifampicin + Ofloxacin + Minocycline for single-lesion PB leprosy
- Rifampicin CYP interaction: Potent inducer - reduces OCP efficacy, warfarin, etc.
- Dapsone syndrome: Fever + rash + lymphadenopathy + hepatitis; idiosyncratic; onset 6-8 weeks
- Clofazimine + QT prolongation: Monitor ECG, especially with other QT-prolonging drugs
- MDT duration: MB = 12 months; PB = 6 months
- Type 1 reaction treatment: Prednisolone (nerve function emergency - do NOT stop MDT)
Sources:
- Katzung's Basic & Clinical Pharmacology, 16th Ed. (9781260463309)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics (9781264258079)
- Lippincott Illustrated Reviews: Pharmacology (9781975170561)
- Fitzpatrick's Dermatology, 9th Ed. (9780071837781)
- Harrison's Principles of Internal Medicine, 22nd Ed. (9781265977061)
- K. Park's Community Medicine (9789382219163)
Seminar on multi bCillary pharmacology
Based on your previous two seminars, it looks like you want a combined seminar covering the pharmacology specific to multibacillary (MB) leprosy - essentially the MDT drugs (Rifampicin, Dapsone, Clofazimine) in the context of MB disease, reactions, second-line agents, and special situations.
I already have all the content from the textbooks loaded in our conversation. Here is the full integrated seminar:
Seminar: Pharmacology of Multibacillary Leprosy
1. Introduction
Multibacillary (MB) leprosy represents the high-bacterial-load end of the leprosy spectrum (BB, BL, LL types). Its pharmacological management is more complex than paucibacillary disease because:
- The bacterial burden is enormous (Bacterial Index up to 6+)
- Treatment duration is longer (12 months vs. 6 months)
- The risk of leprosy reactions - particularly ENL (Type 2) - is high
- Clofazimine is added specifically to combat reactions and the higher bacillary load
- Relapse, though rare, is more likely in patients with very high initial BI (≥4)
The fundamental pharmacological strategy is WHO Multidrug Therapy (MDT), introduced in 1981 after widespread dapsone resistance emerged from decades of monotherapy.
2. Why Multidrug Therapy?
| Problem with Monotherapy | MDT Solution |
|---|---|
| Dapsone resistance by 1970s | Three drugs with different targets - resistance to all three simultaneously is negligible |
| Long treatment duration (years) | Combination kills organisms faster; 12 months is sufficient |
| ENL reactions | Clofazimine's anti-inflammatory action suppresses ENL |
| High relapse rate | Triple bactericidal pressure sterilizes tissue faster |
"The fall in prevalence rate is largely explained by improvement in management of cases, very low rates of relapse, high cure rates, absence of drug resistance and shorter duration of treatment with MDT." - K. Park's Community Medicine
3. The Three Pillars of MB-MDT
At a glance
| Drug | Dose in MB-MDT | Frequency | Mode |
|---|---|---|---|
| Rifampicin | 600 mg | Once monthly | Supervised |
| Clofazimine | 300 mg | Once monthly | Supervised |
| Clofazimine | 50 mg | Daily | Self-administered |
| Dapsone | 100 mg | Daily | Self-administered |
Duration: 12 months
Pediatric dosing (10-14 years): Rifampicin 450 mg monthly + Clofazimine 150 mg monthly + 50 mg on alternate days + Dapsone 50 mg daily.
4. Drug 1 - Rifampicin: The Backbone
Why it is the most important drug
Rifampicin is the only highly bactericidal drug against M. leprae. It kills 99% of viable organisms with just 3-4 consecutive daily doses of 600 mg. This is why:
- It renders patients non-infectious within 3 weeks
- It is given monthly under supervision (because even one monthly dose has enormous killing power)
- It is the single most effective anti-leprosy drug ever discovered
Mechanism
Rifampicin binds the β-subunit of DNA-dependent RNA polymerase (DDRP), encoded by the rpoB gene, blocking initiation of RNA transcription. This halts protein synthesis and kills the organism.
Pharmacokinetics relevant to MB leprosy
| Parameter | Clinical Relevance |
|---|---|
| Well absorbed orally | Standard oral route is effective |
| Half-life ~3.5 hours | Short, but concentration-dependent killing means monthly dosing is bactericidal |
| Potent CYP450 inducer | Reduces efficacy of oral contraceptives, warfarin, corticosteroids used for reactions |
| Turns body fluids orange | Warn patient - urine, tears, sweat turn orange; harmless |
| Penetrates cells and tissues | Reaches intracellular M. leprae in Schwann cells and macrophages |
Key adverse effects in MB leprosy context
| Effect | Clinical Note |
|---|---|
| Hepatotoxicity | Monitor LFTs; especially relevant since patients may also be on corticosteroids for reactions |
| Flu-like syndrome | With intermittent (monthly) dosing - fever, myalgias, rigors |
| GI upset | Anorexia, nausea, vomiting; monitor patient for 1 hour after supervised dose |
| Thrombocytopenia | Rare; with intermittent dosing |
| CYP450 induction | Reduces plasma levels of dapsone (~50%); reduces corticosteroid levels when used for reactions - may need higher steroid doses |
| Orange discoloration | Body fluids - not harmful but counsel patients |
Resistance
- rpoB mutations confer resistance
- Rifampicin resistance in leprosy is rare but reported from several countries
- MDT prevents resistance through combination therapy
- If rifampicin-resistant: switch to second-line regimen (see Section 9)
5. Drug 2 - Dapsone: The Backbone Partner
Role in MB-MDT
Dapsone is given daily as the self-administered component of MDT. Though only weakly bactericidal, its daily continuous action complements rifampicin's monthly bactericidal pulses and prevents regrowth between doses.
Mechanism
Dapsone competitively inhibits dihydropteroate synthase (DHPS) - the same target as sulfonamides - blocking conversion of para-aminobenzoic acid (PABA) to dihydropteroic acid in the folate synthesis pathway. This prevents bacterial DNA synthesis.
Active metabolite (DDS-NOH / dapsone hydroxylamine):
- Produced by CYP2C19, 3A4, 2C9 in liver
- Toxic - causes hemolysis and methemoglobinemia
- Also has anti-inflammatory activity (inhibits neutrophil chemotaxis) - relevant in leprosy reactions
Pharmacokinetics relevant to MB leprosy
| Parameter | Clinical Relevance |
|---|---|
| Well absorbed orally | Reliable daily self-administration |
| Half-life ~28-30 hours | Enterohepatic recirculation prolongs action; once-daily dosing is effective |
| High skin concentration | Skin infected with M. leprae contains several times more drug than normal skin |
| Hepatic N-acetylation | Polymorphic (slow/fast acetylators) - but clinically irrelevant; do not need to check |
| Excreted in breast milk | Risk of hemolysis in nursing infants |
| Renal excretion | Dose reduction needed in renal failure |
Adverse effects specific to MB leprosy
| Effect | Mechanism | Clinical Relevance |
|---|---|---|
| Hemolytic anemia | DDS-NOH → oxidant stress on RBCs → Heinz body formation | ~20% of patients; dose-related; much worse in G6PD deficiency - test before starting |
| Methemoglobinemia | DDS-NOH oxidizes Fe²⁺ → Fe³⁺ (methemoglobin) | Usually subclinical; severe in NADH-methemoglobin reductase deficiency |
| ENL triggering | Dapsone therapy itself can precipitate ENL reactions in lepromatous patients | Can be difficult to distinguish from disease progression - important clinical trap |
| Dapsone syndrome | Idiosyncratic; fever + rash + hepatitis + lymphadenopathy | Onset 6-8 weeks; rare but potentially fatal |
| Agranulocytosis | Idiosyncratic | Rare; stop drug immediately |
| Peripheral neuropathy | Direct toxicity | Rare |
Critical Point: G6PD screening before starting dapsone - G6PD-deficient patients develop severe hemolysis. If G6PD deficient, dapsone can be replaced by clofazimine (additional dose) in the MDT regimen.
Critical Point: Hemoglobin should be ≥60% (not severely anemic) before starting dapsone (Indian national guidelines). Prescribe iron supplements routinely.
Dapsone and ENL (Type 2 Reaction)
In MB leprosy patients on dapsone-containing MDT, ENL can develop as an immune complex-mediated reaction. This is not a drug allergy - it is the immunological response to dying M. leprae antigens. Continue MDT; manage the reaction separately with thalidomide or corticosteroids.
6. Drug 3 - Clofazimine: The Multi-Role Drug
Clofazimine is uniquely valuable in MB leprosy because it serves two distinct pharmacological roles simultaneously: anti-mycobacterial AND anti-inflammatory.
Mechanism of action (multifactorial)
- Membrane disruption - directly damages mycobacterial cell membrane integrity
- Inhibition of mycobacterial phospholipase A2
- Inhibition of K⁺ transport across bacterial membrane
- Generation of ROS (H₂O₂ and superoxide) via redox cycling - directly toxic to bacteria
- Disruption of electron transport chain
- Efflux pump inhibition
- Anti-inflammatory: inhibits macrophages, T lymphocytes, neutrophils, and complement activation
"ENL may not develop in patients treated with clofazimine" - Lippincott Pharmacology
Why clofazimine is essential in MB (but not PB) leprosy
| Reason | Explanation |
|---|---|
| Higher bacterial load | More drug needed for sterilization |
| ENL prevention | MB patients (BL/LL) have ~50% risk of ENL; clofazimine's anti-inflammatory action prevents/suppresses it |
| Anti-inflammatory synergy | Reduces need for corticosteroids and thalidomide |
| Psychosocial (skin discoloration) | In PB leprosy (limited disease), adding clofazimine just for its anti-inflammatory benefit is not justified given the social stigma of discoloration |
Pharmacokinetics relevant to MB leprosy
| Parameter | Clinical Relevance |
|---|---|
| Oral bioavailability 45-60% | Increased 2-fold by high-fat meals - advise patients to take with food; antacids reduce absorption by 30% |
| Volume of distribution ~10,000 L | Massive tissue accumulation - drug reaches deep tissue M. leprae reservoirs |
| Half-life ~35 days | Extremely long; permits monthly supervised dosing + daily low-dose self-administration; residual drug persists months after stopping |
| Does NOT enter CNS | No CNS effects; not useful for neural leprosy in the brain |
| Crystal deposits in tissues | Intestinal mucosa, liver, spleen, lymph nodes - can cause obstructive GI complications |
| Metabolized in liver | 4-step process: dehalogenation, deamination, glucuronidation, hydroxylation |
Adverse effects specific to MB leprosy
| Effect | Details |
|---|---|
| Skin discoloration | Most prominent and most distressing; dose-dependent; pink → reddish-brown → brownish-black; affects skin + conjunctivae + urine + sputum + sweat; fades in 6-12 months after stopping; traces may persist up to 4 years. This discoloration "outs" patients as leprosy patients, causing major psychosocial harm and treatment non-adherence. Must counsel extensively before starting. |
| Ichthyosis | Dry, scaling skin on shins and forearms |
| GI toxicity (40-50%) | Cramps, diarrhea, nausea, weight loss - due to crystal deposition in intestinal wall; rarely requires surgery |
| QT prolongation | ECG monitoring warranted, especially with other QT-prolonging agents |
| Accumulation in lesions | Clofazimine accumulates in active leprosy skin lesions, making them temporarily more prominent - warn patients |
Drug interaction specific to MB leprosy
- Dapsone inhibits the anti-inflammatory effects of clofazimine (pharmacodynamic antagonism) - Goodman & Gilman
- Antacids reduce clofazimine absorption
7. The Pharmacological Basis of ENL Suppression by Clofazimine
ENL (Erythema Nodosum Leprosum / Type 2 reaction) is an immune complex-mediated vasculitis occurring in 50% of BL/LL patients. The reaction involves:
- TNF-α overproduction
- Elevated IL-1, IL-6
- Complement activation with membrane attack complex (MAC) generation in nerves
- Increased CD4:CD8 ratio in skin and blood
Clofazimine addresses this through:
- Inhibition of macrophage and T-cell activation
- Complement inhibition
- Reduction of pro-inflammatory cytokines
However, the anti-inflammatory effect takes 4-6 weeks to develop - so acute ENL still requires immediate treatment with thalidomide or corticosteroids.
8. Treatment of Reactions in MB Leprosy
Golden Rule: NEVER stop MDT during a reaction
Stopping MDT allows bacterial regrowth. Reactions are immunological events - not drug toxicity. Continue MDT and treat the reaction separately.
Type 1 Reaction (Reversal Reaction) - Occurs in BL
| Feature | Management |
|---|---|
| Mechanism | Upregulation of CMI (Th1 response) to M. leprae antigens |
| Emergency signal | Acute neuritis - sudden nerve function loss |
| Treatment | Prednisolone 40-60 mg/day, taper over 3-6 months |
| Rationale | Corticosteroids suppress the acute CMI inflammation within infected nerves |
| DO NOT use | Thalidomide (not effective for Type 1) |
Type 2 Reaction (ENL) - Occurs in BL/LL
| Scenario | Drug of Choice | Notes |
|---|---|---|
| Acute moderate-to-severe ENL | Thalidomide 100-300 mg/day | FDA-approved 1998 for ENL; inhibits TNF-α; most effective |
| Women of childbearing age | Prednisolone | Thalidomide absolutely contraindicated in pregnancy - phocomelia |
| Chronic recurrent ENL | Clofazimine 100-200 mg/day | Steroid-sparing; takes 4-6 weeks to work |
| Mild ENL | NSAIDs / Aspirin | Symptomatic relief only |
Thalidomide in ENL - Pharmacology
| Feature | Detail |
|---|---|
| Mechanism | Inhibits TNF-α synthesis; immunomodulation of IL-12, IFN-γ; anti-angiogenic |
| History | Withdrawn 1961 (phocomelia/limb defects in fetuses); re-approved FDA 1998 for ENL |
| Classification | Orphan drug (FDA) |
| Indication | Moderate-to-severe acute ENL; maintenance to prevent recurrence |
| Key toxicity | Absolute teratogen (phocomelia); peripheral neuropathy; sedation; DVT; thromboembolic events |
| Prescribing restriction | REMS/STEPS program in USA; mandatory contraception for women of childbearing potential |
9. Second-Line Drugs for Resistant/Intolerant MB Leprosy
Used when: (a) patients cannot tolerate first-line drugs, or (b) rifampicin resistance is confirmed.
Individual Drug Substitutions (Intolerance)
| Intolerant to | Substitute with |
|---|---|
| Rifampicin | Ofloxacin 400 mg/day OR Minocycline 100 mg/day |
| Dapsone | Clofazimine 50 mg/day (additional dose) |
| Clofazimine | Minocycline 100 mg/day OR Ofloxacin 400 mg/day |
Rifampicin-Resistant Leprosy (WHO Protocol)
Phase 1 (6 months): Clofazimine + at least 2 of: clarithromycin, minocycline, ofloxacin/levofloxacin/moxifloxacin - all daily
Phase 2 (18 months): Clofazimine + one second-line drug daily
Rifampicin + Ofloxacin dual resistance: Clarithromycin + minocycline + clofazimine × 6 months → clarithromycin or minocycline + clofazimine × 18 months
Second-Line Drugs - Key Pharmacology
| Drug | Class | Mechanism | Activity against M. leprae |
|---|---|---|---|
| Ofloxacin | Fluoroquinolone | Inhibits DNA gyrase + topoisomerase IV | Bactericidal; clearance similar to rifampicin |
| Minocycline | Tetracycline | Inhibits 30S ribosomal subunit | Bactericidal; clears bacilli faster than dapsone or clofazimine |
| Clarithromycin | Macrolide | Inhibits 50S ribosomal subunit | Bactericidal |
| Moxifloxacin | Fluoroquinolone | DNA gyrase + topo IV | Most potent fluoroquinolone; ROM regimen use |
ROM regimen (single-lesion PB leprosy - not MB): Single dose of Rifampicin + Ofloxacin + Minocycline
10. Relapse in MB Leprosy - Pharmacological Approach
- Cure rate with MDT: ~99%
- Relapse defined as: increase in BI of ≥2+ over previous value at any single site, with clinical deterioration
- Relapse rate: <1% overall; up to 4-7 per 100 person-years in patients with initial BI ≥4
- Most relapses occur within 5 years of completing MDT
Treatment of relapse:
- Re-treat with the same MB-MDT regimen (no dose escalation needed)
- Resistance to all three MDT drugs simultaneously is extremely rare
- Patients with MB disease require monitoring for at least 5 years after completing MDT
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025)
11. Drug Interactions Matrix for MB-MDT
| Drug Pair | Interaction | Clinical Action |
|---|---|---|
| Rifampicin + Dapsone | Rifampicin reduces dapsone levels ~50% (CYP induction) | MDT doses are pre-adjusted for this |
| Rifampicin + Corticosteroids (for reactions) | Rifampicin reduces prednisolone levels | Use higher steroid doses (1.5-2x) |
| Rifampicin + Oral contraceptives | Rifampicin reduces OCP efficacy | Use alternative/barrier contraception |
| Clofazimine + Dapsone | Dapsone inhibits clofazimine's anti-inflammatory action | Unavoidable in MDT; clinically managed |
| Clofazimine + QT-prolonging drugs | Additive QT prolongation | Monitor ECG; avoid other QT drugs |
| Clofazimine + Antacids | Antacids reduce clofazimine absorption by ~30% | Separate dosing times |
12. Special Situations in MB Leprosy Pharmacology
| Situation | Pharmacological Consideration |
|---|---|
| G6PD deficiency | Screen before dapsone; if deficient, substitute dapsone with extra clofazimine; risk of life-threatening hemolysis |
| Pregnancy | MDT is safe; thalidomide absolutely contraindicated; clofazimine crosses placenta (neonatal skin discoloration); rifampicin + corticosteroids for reactions |
| HIV co-infection | MDT can be given; major rifampicin-antiretroviral interactions (especially PIs and NNRTIs); consider rifabutin substitution |
| Renal failure | Reduce dapsone dose; rifampicin and clofazimine are primarily biliary/hepatic - safer |
| Hepatic failure | Use all three drugs with caution; rifampicin most hepatotoxic; monitor LFTs |
| Children | Weight-adjusted dosing (see Section 3); same three-drug MDT |
| Histoid leprosy | MB regimen; often associated with prior dapsone resistance - confirm susceptibility |
13. Monitoring During MB-MDT
| Parameter | Frequency | Why |
|---|---|---|
| CBC (Hb, reticulocytes) | Monthly initially | Dapsone-induced hemolysis |
| LFTs | Monthly first 3 months, then 3-monthly | Rifampicin hepatotoxicity |
| G6PD level | Once before starting | Predicts dapsone hemolysis risk |
| Skin smear (BI, MI) | 6-monthly | Assess bacteriological response |
| Disability grade assessment | At diagnosis, 6, 12 months | Monitor nerve function; detect reactions early |
| ECG | If high-risk or co-medications | Clofazimine QT prolongation |
| Skin counseling | Each visit | Clofazimine discoloration adherence |
14. Exam High-Yield Summary
| Question | Answer |
|---|---|
| Most potent anti-leprosy drug | Rifampicin |
| Only bactericidal drug in MB-MDT | Rifampicin (most potent); clofazimine also bactericidal |
| Drug that prevents ENL | Clofazimine |
| Drug of choice for ENL | Thalidomide |
| Why thalidomide cannot be used in pregnant women | Phocomelia (absolute teratogen) |
| Toxic metabolite of dapsone | Dapsone hydroxylamine (DDS-NOH) |
| Dapsone mechanism | Inhibits dihydropteroate synthase (DHPS) |
| Why rifampicin is given monthly (not daily) in MDT | Monthly supervised dose has enough bactericidal power; ensures compliance; even monthly dosing kills 99% viable organisms |
| Half-life of clofazimine | ~35 days |
| Why clofazimine is not given in PB leprosy | Psychosocial harm of skin discoloration; ENL risk is low in PB disease |
| What makes clofazimine unique | Dual action: bactericidal + anti-inflammatory |
| Duration of MB-MDT | 12 months |
| What to do during a leprosy reaction | Continue MDT; treat reaction separately |
| Dapsone hypersensitivity syndrome features | Fever + rash + hepatitis + lymphadenopathy (onset 6-8 weeks) |
| Clofazimine in pregnancy | Crosses placenta; neonatal skin discoloration; continue if necessary |
| Rifampicin color change | Turns body fluids orange-red (urine, tears, sweat) |
Sources:
- Katzung's Basic & Clinical Pharmacology, 16th Ed. (9781260463309)
- Goodman & Gilman's Pharmacological Basis of Therapeutics (9781264258079)
- Lippincott Illustrated Reviews: Pharmacology (9781975170561)
- Fitzpatrick's Dermatology (9780071837781)
- Harrison's Principles of Internal Medicine, 22nd Ed. (9781265977061)
- K. Park's Textbook of Community Medicine (9789382219163)
This is a shared conversation. Sign in to Orris to start your own chat.