Derivatives of mesonephric duct 5 mark Short note
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have all the information needed for a comprehensive 5-mark short note. Let me compose the answer.
Derivatives of the Mesonephric (Wolffian) Duct
Introduction
The mesonephric duct, also called the Wolffian duct, is a paired embryonic structure that appears in the fourth week of development, lateral to the mesonephros. It originally drains mesonephric tubules into the cloaca. The mesonephros functions as an interim kidney for ~4 weeks before degenerating, but the duct itself persists and gives rise to important adult structures depending on the hormonal environment of the fetus.
- The Developing Human: Clinically Oriented Embryology, p. 681-684
Hormonal Regulation
- In males (XY): Testosterone produced by Leydig cells maintains and differentiates the mesonephric duct into male genital structures. Simultaneously, Anti-Mullerian Hormone (AMH) from Sertoli cells causes regression of the paramesonephric (Mullerian) duct.
- In females (XX): Without testosterone, the Wolffian duct degenerates and only rudimentary vestiges remain. The Mullerian duct instead develops into the female reproductive tract.
- Color Atlas of Human Anatomy Vol. 2, p. 544-545; Medical Physiology, p. 884
Derivatives in the MALE
The Wolffian duct is preserved under testosterone and differentiates into the following, craniocaudally:
| Structure | Origin from Mesonephric Duct |
|---|---|
| Appendix of epididymis | Cranial end of the duct (vestigial) |
| Duct of epididymis | Segment adjacent to the testis; becomes highly coiled (~6 m) |
| Ductus (Vas) deferens | Caudal to epididymis; 30-35 cm long; transports sperm from cauda epididymis to ejaculatory duct |
| Ejaculatory duct | Terminal portion of vas deferens, after joining the seminal vesicle duct |
| Seminal vesicle (seminal gland) | Lateral outgrowth from the distal end of the mesonephric duct |
Note: The efferent ductules of the testis are derived from mesonephric tubules (not the duct itself), and connect the rete testis to the epididymis. The prostate arises separately from urethral epithelial buds, not from the mesonephric duct.
- Campbell-Walsh-Wein Urology; The Developing Human Table 12.1; Color Atlas of Human Anatomy
Derivatives in the FEMALE (Vestigial Remnants)
In females, without testosterone, the mesonephric duct regresses but leaves behind rudimentary structures:
| Remnant | Location/Description |
|---|---|
| Gartner's duct (longitudinal duct of epoophoron) | Runs along the anterolateral wall of the vagina and uterus |
| Duct of epoophoron | In the broad ligament, lateral to the ovary |
| Appendix vesiculosa | Small vestigial cyst near the ovary |
Mesonephric tubules in the female give rise to the epoophoron and paroophoron (vestigial structures in the broad ligament).
- The Developing Human, Table 12.1, p. 684
Histological Landmark: Mesonephric Duct at ~42 Days
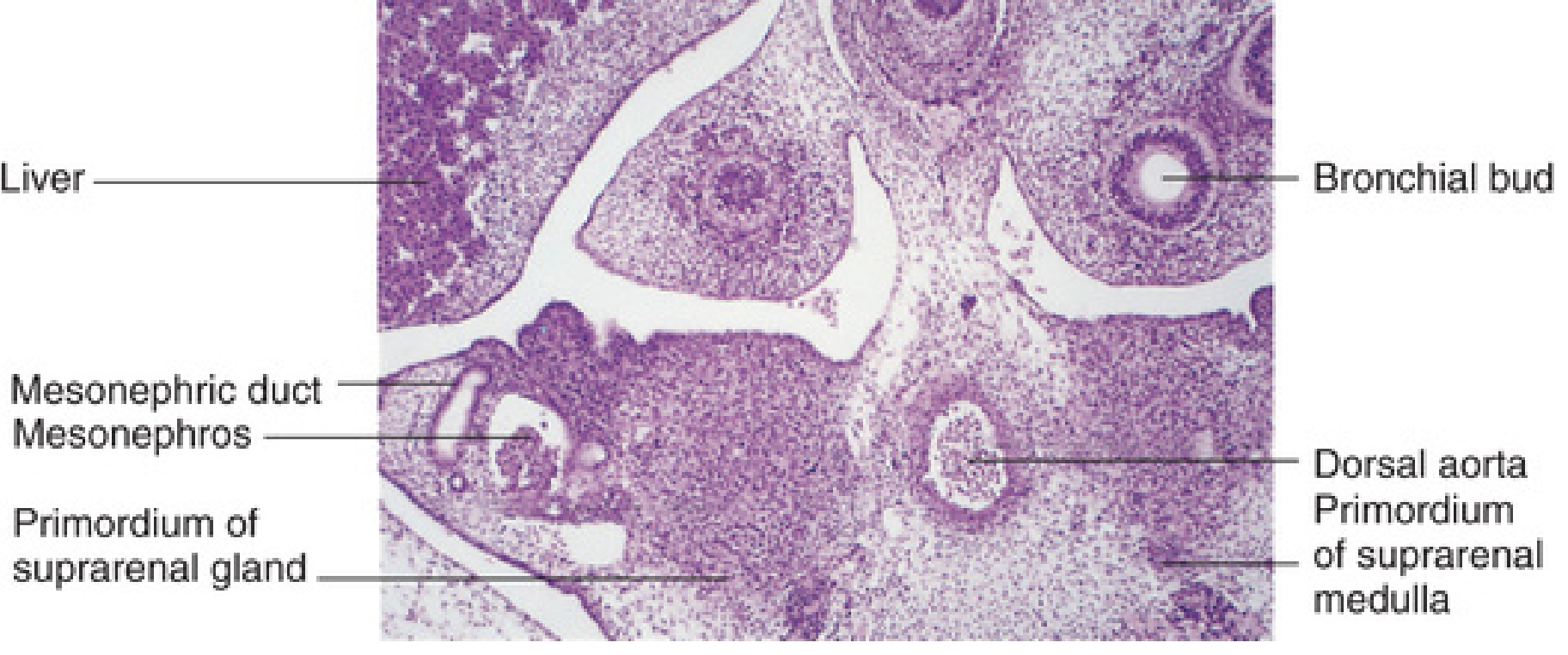
Photomicrograph of transverse section at ~42 days (6 weeks), showing the mesonephric duct and mesonephros - From The Developing Human, Fig. 12.4
Summary Table (Table 12.1 - The Developing Human)
| Embryonic Structure | Male Derivative | Female Derivative |
|---|---|---|
| Mesonephric duct | Appendix of epididymis, Duct of epididymis, Ductus deferens, Ejaculatory duct, Seminal vesicle | Appendix vesiculosa, Duct of epoophoron, Gartner's duct |
| Mesonephric tubules | Efferent ductules of testis, Paradidymis | Epoophoron, Paroophoron |
| Stalk of ureteric bud | Ejaculatory duct + ureter/pelvis/calices | Ureter/pelvis/calices |
Clinical Relevance
- Gartner's duct cysts: Remnants of the mesonephric duct in females can form cysts along the anterolateral vaginal wall. They appear as benign, thin-walled cysts on imaging.
- Congenital bilateral absence of vas deferens (CBAVD): A mesonephric duct-derived structure; associated with CFTR mutations (cystic fibrosis gene) and results in obstructive azoospermia.
- Renal agenesis with seminal vesicle anomaly: Since the ureteric bud arises from the mesonephric duct, unilateral renal agenesis is often accompanied by ipsilateral seminal vesicle aplasia.
- Campbell-Walsh-Wein Urology; Smith & Tanagho's General Urology, 19th Ed.
Short note on stomach bed
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
stomach bed anatomy structures posterior surface lesser sac
Reading File
Finding Sources
I have enough information from the textbooks plus my comprehensive anatomical knowledge. Let me now compose the full short note.
Stomach Bed
Definition
The stomach bed refers to the group of structures that form the floor of the lesser sac (omental bursa) and directly underlie the posterior surface of the stomach, separated from it by the peritoneum of the lesser sac. These are the structures upon which the posterior wall of the stomach "rests."
- Fischer's Mastery of Surgery, 8th ed.
Boundaries
The stomach bed is essentially the posterior wall of the lesser sac (omental bursa). It is bounded:
- Anteriorly - by the peritoneum lining the posterior surface of the stomach
- Posteriorly - by the posterior parietal peritoneum covering the structures of the stomach bed
- Superiorly - by the diaphragm
- Inferiorly - by the transverse mesocolon
Structures Forming the Stomach Bed
From above downward and left to right, the following structures form the stomach bed:
1. Diaphragm
- Forms the uppermost part of the stomach bed
- The posterior surface of the fundus and the upper body of the stomach rest on the left dome of the diaphragm
- The diaphragm separates the stomach from the left pleural cavity and left lung
2. Left Suprarenal (Adrenal) Gland
- Lies on the medial aspect of the upper pole of the left kidney
- Forms part of the stomach bed in the upper and medial region
- Covered by the posterior parietal peritoneum of the lesser sac
3. Upper Part of Left Kidney
- The anterior surface of the upper pole of the left kidney contributes to the stomach bed
- Lies behind the peritoneum of the lesser sac
- Explains why left renal pathology can present with gastric symptoms
4. Pancreas (Body and Tail)
- The most important and central structure of the stomach bed
- The body and tail of the pancreas lie posterior to the lesser sac peritoneum, directly behind the stomach
- The splenic artery runs along the superior border of the pancreas
- Explains why carcinoma of the body of the pancreas can invade the posterior wall of the stomach
- Pancreatic pseudocysts typically bulge forward into the lesser sac, displacing the stomach anteriorly
5. Splenic Artery
- Runs a tortuous course along the superior border of the body of the pancreas
- Forms part of the posterior wall of the lesser sac and thus the stomach bed
6. Spleen
- The spleen lies in contact with the posterolateral aspect of the stomach
- Connected to the stomach by the gastrosplenic ligament (containing short gastric and left gastroepiploic vessels)
- Connected to the posterior abdominal wall by the splenorenal (lienorenal) ligament (containing splenic vessels and the tail of the pancreas)
7. Transverse Mesocolon
- Forms the inferior boundary of the stomach bed
- The posterior surface of the antrum of the stomach is related to the transverse mesocolon
Summary Table
| Structure | Region of Stomach Related |
|---|---|
| Diaphragm (left dome) | Fundus and upper body |
| Left suprarenal gland | Upper body (medial) |
| Upper pole of left kidney | Body (upper) |
| Body and tail of pancreas | Body (central and main) |
| Splenic artery | Along superior pancreatic border |
| Spleen | Fundus and upper body (lateral) |
| Transverse mesocolon | Antrum (lower) |
Peritoneal Covering
The stomach bed structures are not in direct contact with the stomach. They are separated by:
- The posterior parietal peritoneum (covering the stomach bed structures)
- The cavity of the lesser sac (omental bursa)
- The visceral peritoneum on the posterior surface of the stomach
This arrangement means that fluid (blood, pus, pancreatic juice) can collect in the lesser sac between the stomach and its bed.
Clinical Significance
-
Carcinoma of the stomach - posterior wall carcinomas can invade the pancreas, left kidney, or spleen, making resection difficult.
-
Pancreatitis and pancreatic pseudocysts - inflammation or pseudocyst of the pancreatic body/tail displaces the stomach anteriorly. The pseudocyst bulges into the lesser sac and is visible on barium meal as anterior displacement of the stomach.
-
Gastric surgery - mobilization of the posterior wall of the stomach requires careful dissection to avoid injury to the splenic artery, pancreas, and left kidney.
-
Left subphrenic abscess - can form between the diaphragm and the posterior surface of the stomach, within the confines of the lesser sac.
-
Referred pain - posterior gastric ulcers may penetrate into the pancreas (the most common organ of penetration), causing pain radiating to the back.
- Fischer's Mastery of Surgery, 8th ed.; Grainger & Allison's Diagnostic Radiology; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.