Pulmonary Function Tests - MD ANAESTHESIA PG EXAM - 30 marks major answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive, rich content from multiple authoritative anaesthesia and pulmonary textbooks. Let me compose the complete 30-mark major answer.
Pulmonary Function Tests (PFTs)
MD Anaesthesia PG Examination - 30 Marks
1. INTRODUCTION
Pulmonary function tests (PFTs) are a group of non-invasive investigations that objectively assess the mechanical properties of the lungs, airways, and respiratory muscles. In anaesthesia practice, PFTs serve three key purposes:
- Preoperative risk stratification - identifying patients at risk of postoperative pulmonary complications (PPCs)
- Staging of chronic lung disease - particularly COPD and interstitial lung diseases
- Guiding surgical decisions - especially in lung resection candidates
A thorough history and physical examination remain the cornerstone of preoperative pulmonary assessment. PFTs complement this evaluation in patients with known lung disease, risk factors, or planned thoracic surgery.
- Miller's Anesthesia, 10e, p. 1302
- Barash's Clinical Anesthesia, 9e, p. 3144
2. CLASSIFICATION OF PFTs
| Category | Tests |
|---|---|
| Spirometry | FVC, FEV1, FEV1/FVC, FEF25-75%, PEFR, MVV |
| Lung Volumes | TLC, FRC, RV, VC, IC, ERV (via body plethysmography, N2 washout, He dilution) |
| Diffusing Capacity | DLCO (single breath CO transfer) |
| Airway Resistance | Raw, specific airway conductance (SGaw) |
| Respiratory Muscle Strength | PImax (MIP), PEmax (MEP) |
| Exercise Testing | Cardiopulmonary exercise test (CPET), 6-minute walk test |
3. LUNG VOLUMES AND CAPACITIES
Understanding lung volumes is fundamental to interpreting PFTs.
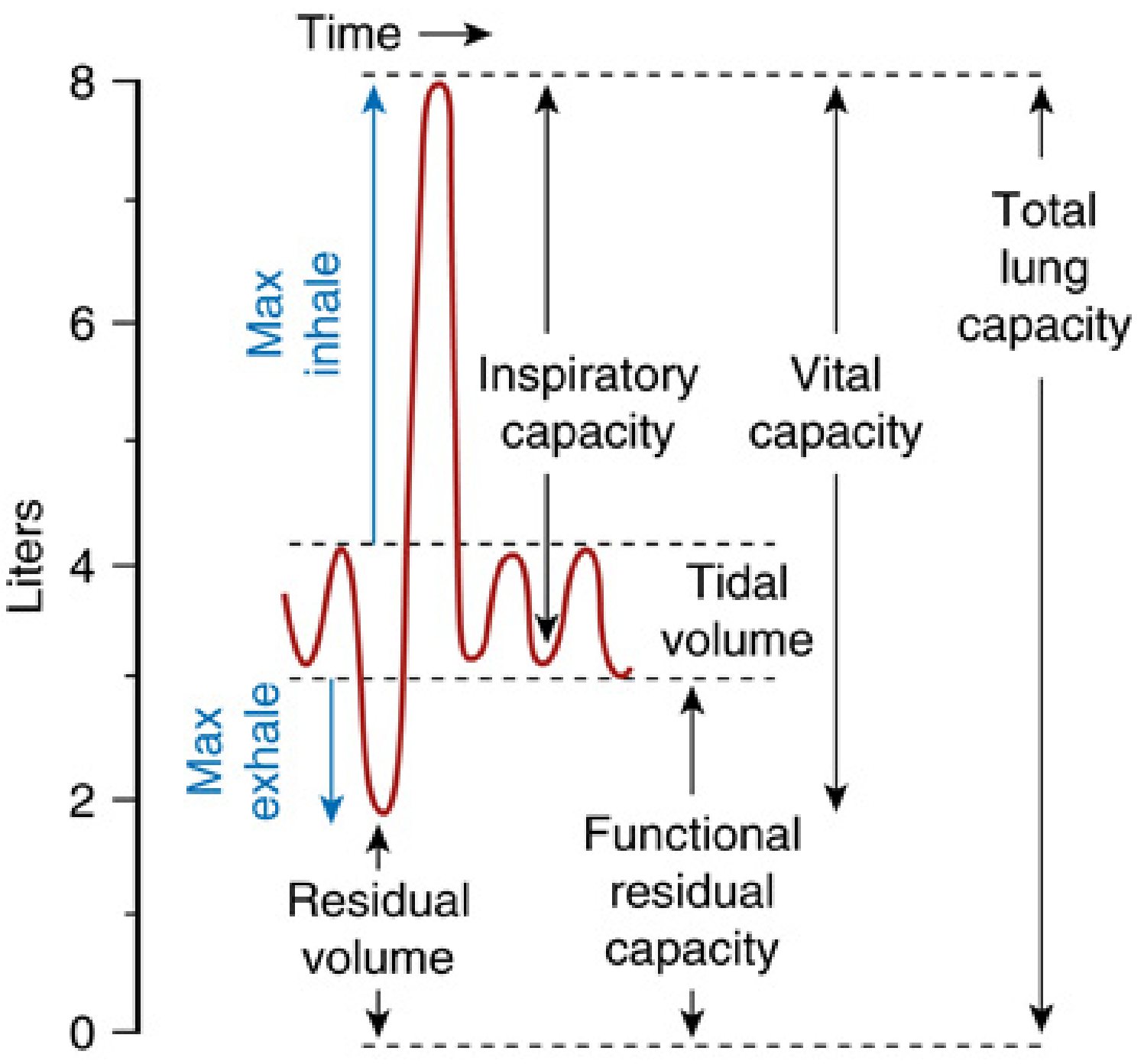
Fig. 1 - Lung volumes and capacities (Miller's Anesthesia, 10e)
Static Lung Volumes (Normal Adult Values)
| Volume/Capacity | Definition | Normal Value |
|---|---|---|
| Tidal Volume (VT) | Air inhaled/exhaled per breath | ~500 mL |
| Inspiratory Reserve Volume (IRV) | Max air inhaled above VT | ~3000 mL |
| Expiratory Reserve Volume (ERV) | Max air exhaled below FRC | ~1000 mL |
| Residual Volume (RV) | Air remaining after maximal exhalation | ~1200 mL |
| Total Lung Capacity (TLC) | Total lung volume at maximal inspiration | ~6000 mL |
| Vital Capacity (VC) | IRV + VT + ERV | ~4500 mL |
| Functional Residual Capacity (FRC) | ERV + RV; end-expiratory volume | ~2200 mL |
| Inspiratory Capacity (IC) | VT + IRV | ~3500 mL |
Key point: RV, FRC, and TLC cannot be measured by spirometry alone - they require nitrogen washout, helium dilution, or body plethysmography.
- Murray & Nadel's Textbook of Respiratory Medicine
- Miller's Anesthesia, 10e, p. 1303
4. SPIROMETRY
4.1 Principle
Spirometry measures the volume of air inhaled or exhaled using a pneumotachometer that measures flow and integrates it to obtain volume. The test consists of:
- Inhalation to TLC
- A forceful, maximal exhalation to RV
- Optionally, maximal inhalation back to TLC (to generate flow-volume loop)
The initial 25-30% of the maximal expiratory maneuver is effort-dependent; the remainder is largely effort-independent. This requires good patient cooperation and a trained technician.
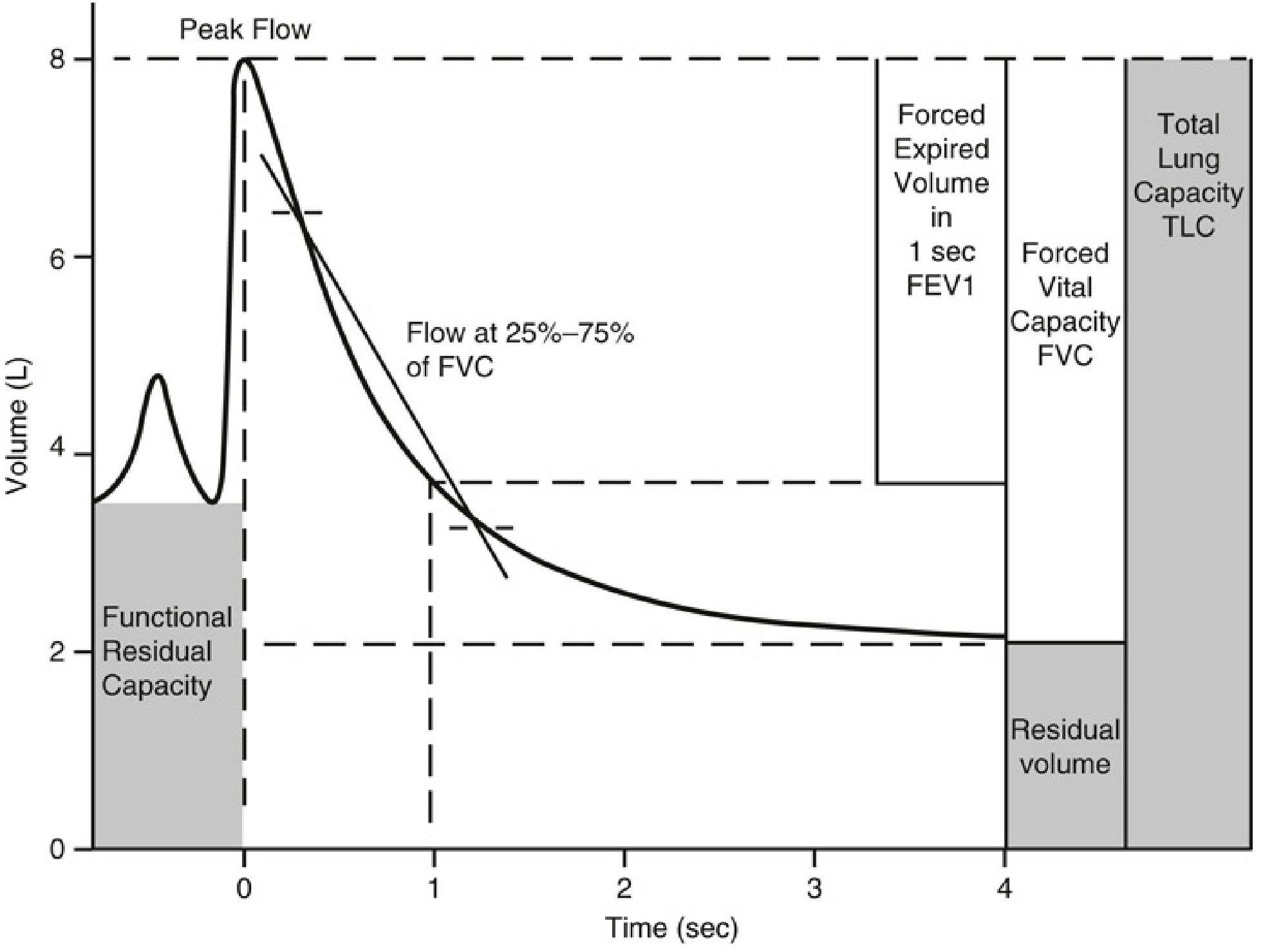
Fig. 2 - Spirometry trace: FEV1, FVC, peak flow, and FEF25-75% (Miller's Anesthesia, 10e)
4.2 Key Spirometric Parameters
| Parameter | Definition | Normal Value |
|---|---|---|
| FVC (Forced Vital Capacity) | Total air forcibly exhaled from TLC to RV | >80% predicted |
| FEV1 | Volume exhaled in the first second | >80% predicted |
| FEV1/FVC ratio | Tiffeneau index | >0.70 (>70%) |
| FEF25-75% | Mean flow during middle half of FVC; small airway index | >60-70% predicted |
| PEFR (Peak Expiratory Flow Rate) | Maximal flow in first 10 ms of exhalation | Effort-dependent |
| MVV (Maximum Voluntary Ventilation) | Maximum volume breathed in 12 seconds x 5 | >80% predicted |
4.3 Interpretation of FEV1/FVC
-
FEV1/FVC < 0.70 = Obstructive defect
-
FEV1/FVC ≥ 0.70 with reduced FVC = Restrictive defect
-
Both FEV1 and FVC reduced with FEV1/FVC ≥ 0.70 = Restriction
-
Miller's Anesthesia, 10e, p. 1302
-
Barash's Clinical Anesthesia, 9e, p. 3144-3145
5. MEASUREMENT OF LUNG VOLUMES
Three techniques are used to measure volumes that include RV (and hence FRC and TLC):
5.1 Body Plethysmography (Gold Standard)
- Patient sits in an airtight, constant-volume chamber (body box)
- Makes inspiratory efforts against a closed shutter with a pressure transducer
- Applies Boyle's Law: P1V1 = P2V2
- As diaphragm contracts, thoracic volume increases and box pressure rises proportionately
- Measures FRC (or RV), from which TLC is derived
- Advantage: Measures all gas in the thorax, including trapped gas - most accurate in severe obstruction
5.2 Nitrogen Washout (Open-Circuit Method)
- Patient inhales 100% oxygen; all exhaled gas collected
- N2 concentration measured in exhaled gas by microprocessors
- When exhaled N2 < 1.5% for 3 breaths, test ends
- N2 washed out = 80% of initial lung gas → FRC calculated
- Modern ventilators use a modification of this technique for FRC estimation at the bedside
5.3 Helium Dilution (Closed-Circuit Method)
-
Patient rebreathes a known volume and concentration of He in a closed circuit
-
He equilibrates until concentration stabilizes
-
C1V1 = C2(V1 + FRC) → FRC calculated
-
Limitation: Underestimates FRC in severe obstruction (poorly ventilated regions don't equilibrate)
-
Miller's Anesthesia, 10e, p. 1303
-
Murray & Nadel's Respiratory Medicine
6. FLOW-VOLUME LOOPS
The flow-volume loop plots flow (y-axis) against lung volume (x-axis) during a maximal expiration followed by a maximal inspiration. It displays the same spirometric information more conveniently and allows identification of airway obstruction patterns.
6.1 Normal Flow-Volume Loop
- Expiratory limb: rapid rise to peak flow (effort-dependent), followed by a linear decline (effort-independent)
- Inspiratory limb: symmetric, semicircular shape
- Flow at 75%, 50%, 25% of VC (V75, V50, V25) can be measured
- FEF25-75% reflects small airway resistance (effort-independent portion)
6.2 Patterns in Disease
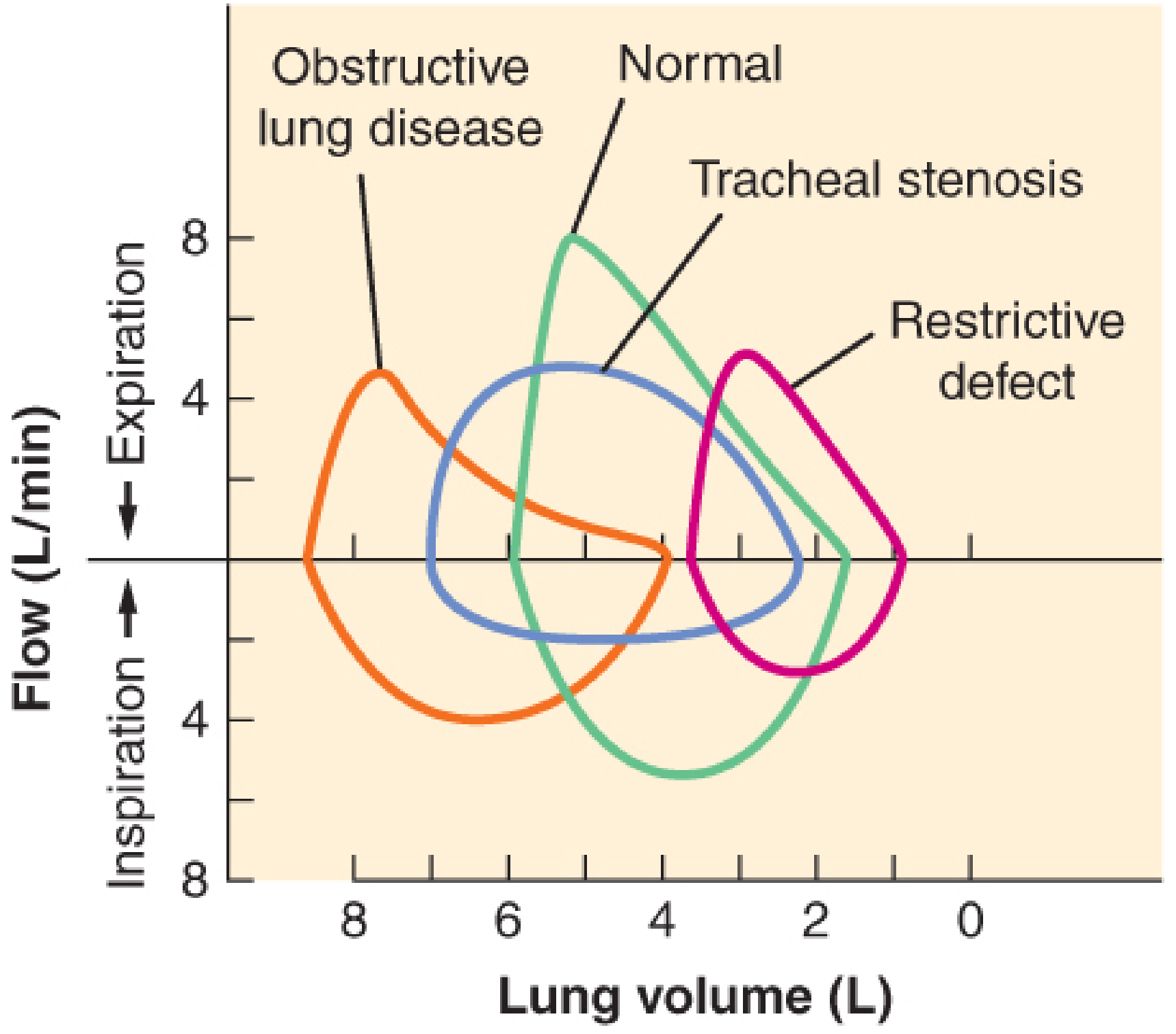
Fig. 3 - Flow-volume loops: Normal, Obstructive lung disease, Tracheal stenosis, Restrictive defect (Barash's Clinical Anesthesia, 9e)
| Pattern | FEV1/FVC | TLC | Shape of Loop |
|---|---|---|---|
| Obstructive (COPD, asthma) | ↓ (<0.70) | ↑ | Concave (scooped) expiratory limb, shifted left |
| Restrictive (fibrosis, scoliosis) | Normal | ↓↓ | Normal shape but reduced size (shifted right) |
| Fixed obstruction (tracheal stenosis) | ↓ | Normal | Flattening of BOTH inspiratory and expiratory limbs |
6.3 Variable Airway Obstruction
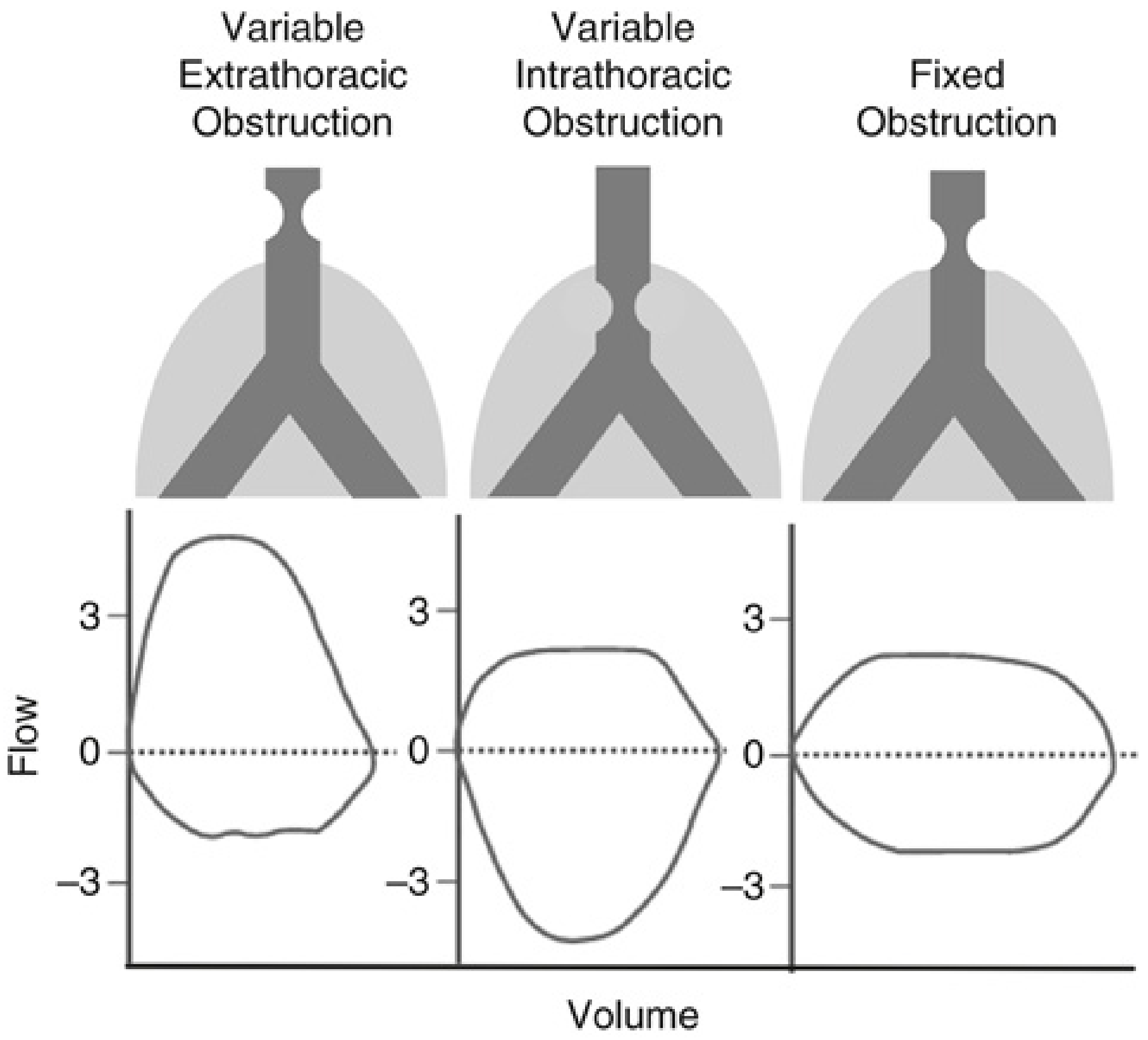
Fig. 4 - Variable extrathoracic, variable intrathoracic, and fixed obstruction patterns (Miller's Anesthesia, 10e)
| Type | Flattening | Mechanism | Example |
|---|---|---|---|
| Variable extrathoracic obstruction | Inspiratory limb flattened | During inspiration, atmospheric pressure > lesion lumen pressure → collapse | Vocal cord palsy, subglottic stenosis |
| Variable intrathoracic obstruction | Expiratory limb flattened | During forced expiration, pleural pressure > lesion lumen pressure → collapse | Tracheomalacia, intrathoracic tracheal tumor |
| Fixed obstruction | Both limbs flattened equally | Obstruction is rigid; not affected by pressure changes | Tracheal ring, bilateral vocal cord fixation |
- Miller's Anesthesia, 10e, p. 1302
- Barash's Clinical Anesthesia, 9e, p. 3145-3146
7. PATTERNS OF PFT ABNORMALITY
7.1 Obstructive Pattern
| Parameter | Change |
|---|---|
| FEV1 | ↓↓ |
| FVC | Normal or mildly ↓ |
| FEV1/FVC | ↓ (<0.70) |
| TLC | ↑ (air trapping) |
| RV, FRC | ↑ |
| FEF25-75% | ↓ (early small airway disease) |
Causes: COPD (chronic bronchitis, emphysema), asthma, bronchiectasis, cystic fibrosis, small airway disease
The hallmark is a reduction in FEV1/FVC%. In emphysema, loss of elastic recoil leads to dynamic airway compression. In chronic bronchitis, airway narrowing is due to fibrosis and secretions. RV, FRC, and TLC are typically all elevated (air trapping).
7.2 Restrictive Pattern
| Parameter | Change |
|---|---|
| FEV1 | ↓ |
| FVC | ↓↓ |
| FEV1/FVC | Normal (≥0.70) |
| TLC | ↓↓ |
| RV | ↓ or normal |
| FEF25-75% | Normal |
Causes:
- Pulmonary: Interstitial lung disease, pulmonary fibrosis, sarcoidosis, pneumonia
- Extrapulmonary: Obesity, scoliosis, pleural effusion, neuromuscular disease (myasthenia gravis, GBS), diaphragm palsy
7.3 Mixed Pattern
- Both FEV1/FVC < 0.70 AND TLC reduced
- Seen in: advanced COPD with co-existing fibrosis, bronchiectasis with fibrosis
GOLD Classification of COPD (Spirometry-Based)
| Stage | Criteria (Post-bronchodilator) |
|---|---|
| I - Mild | FEV1 ≥ 80% predicted |
| II - Moderate | 50% ≤ FEV1 < 80% |
| III - Severe | 30% ≤ FEV1 < 50% |
| IV - Very Severe | FEV1 < 30% |
All stages require FEV1/FVC < 0.70.
- Fishman's Pulmonary Diseases and Disorders
- Barash's Clinical Anesthesia, 9e, p. 3145-3146
8. DIFFUSING CAPACITY FOR CARBON MONOXIDE (DLCO)
Principle
DLCO evaluates the functional capillary surface area available for gas exchange. CO is used because its high affinity for hemoglobin keeps alveolar capillary pCO near zero - so transfer is limited only by membrane thickness, not perfusion.
Fick's Law: DLCO is determined by:
- Surface area of alveolar-capillary membrane
- Pressure gradient (alveolar pCO - capillary pCO)
- Membrane thickness
- Molecular weight and solubility of gas
Method (Single Breath Technique)
- Patient inhales a gas mixture containing 0.3% CO + 10% He + 21% O2 (balance N2)
- Holds breath for 10 seconds
- Exhales; sample analyzed for CO and He
- He dilution gives alveolar volume; CO uptake gives DLCO
Clinical Significance
| DLCO | Interpretation |
|---|---|
| >80% predicted | Normal |
| 60-80% | Mild reduction |
| 40-60% | Moderate reduction |
| <40% | Severe reduction |
Causes of reduced DLCO:
- Emphysema (loss of alveolar surface area) - often with normal spirometry in early disease
- Interstitial lung disease (increased membrane thickness)
- Pulmonary hypertension, pulmonary emboli (reduced pulmonary capillary blood volume)
- Anemia (less hemoglobin to bind CO)
- Lobectomy/pneumonectomy
Causes of elevated DLCO:
- Polycythemia, left-to-right shunts, mild left heart failure (increased pulmonary blood volume)
Anaesthetic relevance: DLCO < 60% predicted = increased risk of PPCs; indication for further preoperative evaluation including CPET. - Miller's Anesthesia, 10e, p. 1303-1304
9. RESPIRATORY MUSCLE STRENGTH TESTS
| Test | Description | Significance |
|---|---|---|
| PImax / MIP (Maximum Inspiratory Pressure) | Maximal inspiratory effort against occluded airway at RV | Reflects diaphragm and accessory inspiratory muscle strength; PImax < -25 cmH2O suggests need for ventilatory support |
| PEmax / MEP (Maximum Expiratory Pressure) | Maximal expiratory effort against occluded airway at TLC | Reflects expiratory/abdominal muscle strength; PEmax < +40 cmH2O → impaired cough |
Both PImax and PEmax are reduced in neuromuscular disease, poor effort, and fatigue. Increased lung volumes reduce PImax (flatter diaphragm); decreased lung volumes reduce PEmax. - Fishman's Pulmonary Diseases
10. CARDIOPULMONARY EXERCISE TESTING (CPET)
CPET is a dynamic, integrated test evaluating functional capacity and the contribution of the respiratory, cardiovascular, and musculoskeletal systems.
Key Measured Parameters
| Parameter | Threshold | Clinical Meaning |
|---|---|---|
| VO2max (max oxygen consumption) | <15 mL/kg/min = high risk | Broad indicator of cardiorespiratory reserve |
| Anaerobic Threshold (AT) | <10 mL/kg/min = high risk | Sustainable exercise capacity; point where anaerobic metabolism begins |
| VE/VCO2 slope | >35 = high risk | Efficiency of ventilation; reflects V/Q mismatch and dead space |
Monitoring during CPET: ECG, SpO2, respiratory rate, exhaled gas analysis (VO2, VCO2), airflow, and volume on a cycle ergometer or treadmill with incremental workload.
Anaesthetic significance: CPET is the most comprehensive preoperative cardiorespiratory assessment, particularly for lung resection, major abdominal, and cardiac surgery candidates.
- Miller's Anesthesia, 10e, p. 1307
11. PREOPERATIVE PFT ASSESSMENT FOR LUNG RESECTION
This is a core anaesthetic application of PFTs. Three goals:
- Identify patients at risk of increased postoperative morbidity/mortality
- Identify patients needing short- or long-term postoperative ventilatory support
- Evaluate reversibility of airway obstruction with bronchodilators
Predicted Postoperative FEV1 (ppoFEV1)
ppoFEV1 = Preoperative FEV1 × % lung tissue remaining after resection
| ppoFEV1 | Risk |
|---|---|
| >40% | Reduced risk |
| 30-40% | Moderate risk |
| <30% | High risk - likely needs postoperative ventilation |
Spirometric Thresholds for Lung Resection Risk
| Parameter | High Risk Threshold |
|---|---|
| FEV1 | <60% predicted → increased PPCs; <800 mL historically = absolute contraindication (now less used with VATS) |
| FVC | Abnormal VC in 30-40% of postoperative deaths |
| MVV | <50% predicted |
| RV/TLC ratio | >50% |
| FEV1/FVC | Low ratio = obstructive disease present |
Note: With thoracoscopic surgery (VATS) and improved pain management, patients with lower lung volumes can now be safely operated on. It is preferable to express FEV1 as % predicted rather than absolute value (accounts for age, sex, height). - Barash's Clinical Anesthesia, 9e, p. 3144-3145
12. EFFECTS OF ANAESTHESIA AND SURGERY ON PFT PARAMETERS
Understanding how anaesthesia and surgery alter lung function is equally important:
| Parameter | Change After Surgery |
|---|---|
| TLC | Decreases after abdominal (not limb) surgery |
| VC (Vital Capacity) | Decreases by 25-50% within 1-2 days; returns to normal in 1-2 weeks |
| RV (Residual Volume) | Increases by ~13% |
| ERV | Decreases by 25% after lower abdominal, 60% after upper abdominal/thoracic surgery |
| VT (Tidal Volume) | Decreases by 20% within 24 hours |
| FRC | Decreases ~33% with reduced compliance; small airway closure occurs |
Mechanism of FRC reduction under anaesthesia:
-
Loss of muscle tone alters balance between chest wall recoil (outward) and lung elastic recoil (inward)
-
Moving supine: FRC reduces ~1 L
-
Induction of anaesthesia: further reduces FRC by ~400-500 mL
-
Results in: increased elastic behavior (reduced compliance), increased airway resistance, atelectasis, V/Q mismatch, and impaired oxygenation
-
50% of anaesthesia-related deaths involve hypoxemia
-
Barash's Clinical Anesthesia, 9e, p. 3144
-
Miller's Anesthesia, 10e, p. 1307-1308
13. BRONCHODILATOR REVERSIBILITY TESTING
PFTs are routinely performed before and after bronchodilator administration (typically salbutamol 400 mcg by MDI or nebulization, wait 15 minutes; or ipratropium, wait 30 minutes).
-
Positive response: ≥15% improvement (or ≥200 mL absolute improvement) in FEV1 or FVC
-
Indicates reversible airway obstruction (typical of asthma)
-
Bronchodilator therapy should be initiated/optimized before elective surgery
-
Anaesthetic significance: Prognosis in COPD correlates better with post-bronchodilator spirometry than baseline values
-
Barash's Clinical Anesthesia, 9e, p. 3147
14. SUMMARY TABLE: PFT PATTERNS AT A GLANCE
| Parameter | Normal | Obstructive | Restrictive | Mixed |
|---|---|---|---|---|
| FEV1 | >80% | ↓↓ | ↓ | ↓↓ |
| FVC | >80% | Normal or ↓ | ↓↓ | ↓↓ |
| FEV1/FVC | >0.70 | ↓ (<0.70) | Normal | ↓ |
| TLC | Normal | ↑ | ↓↓ | Variable |
| RV | Normal | ↑↑ | ↓ | ↑ |
| FRC | Normal | ↑ | ↓ | Variable |
| DLCO | Normal | ↓ (emphysema) | ↓ (fibrosis) | ↓ |
| FEF25-75% | Normal | ↓↓ | Normal | ↓ |
| Flow-volume loop | Normal | Scooped, shifted left | Small but normal shape | Mixed |
15. INDICATIONS FOR PFTs IN ANAESTHESIA PRACTICE
- Preoperative - known COPD, asthma, interstitial lung disease, unexplained dyspnoea, thoracic surgery, morbid obesity, neuromuscular disease
- Lung resection - mandatory to calculate ppoFEV1 and guide surgical decision
- Monitoring disease progression - COPD, ILD, sarcoidosis
- ICU - weaning readiness (RSBI = RR/VT < 105 = ready to wean), NIF/PImax assessment
- Assessment of bronchodilator response - asthma vs COPD
- Occupational lung disease - silicosis, asbestosis
CONCLUSION
PFTs provide the anaesthesiologist with objective, quantifiable data about lung mechanics, gas exchange efficiency, and respiratory reserve. Spirometry (FEV1, FVC, FEV1/FVC) forms the foundation of PFT interpretation. Lung volume measurement (particularly body plethysmography) adds information about air trapping and restriction. DLCO identifies impaired gas exchange. Flow-volume loops characterize the site and nature of airway obstruction. CPET offers the most comprehensive preoperative cardiorespiratory risk assessment. Together, these tests guide patient selection for surgery, predict postoperative complications, direct perioperative optimization, and inform ventilatory management in the ICU.
Key References (Sources):
- Miller's Anesthesia, 10e - Chapters 12 and 19
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Chapter 38
- Murray & Nadel's Textbook of Respiratory Medicine - Chapter 31
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set - Chapter 31
This is a shared conversation. Sign in to Orris to start your own chat.