Which anti diabetic drug is preferred in type 2 diabetes with ckd?
Reading File
Finding Sources
Finding Sources
Searching PubMed
"type 2 diabetes" AND "chronic kidney disease" AND "antidiabetic"
Reading File
Finding Sources
Reading Article
PMID: 40798873
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to give a detailed, well-cited answer.
Antidiabetic Drugs in Type 2 Diabetes with CKD
The preferred approach is based on the KDIGO 2022 Clinical Practice Guidelines for Diabetes Management in CKD, and evidence has been further reinforced by multiple large outcome trials and recent meta-analyses.
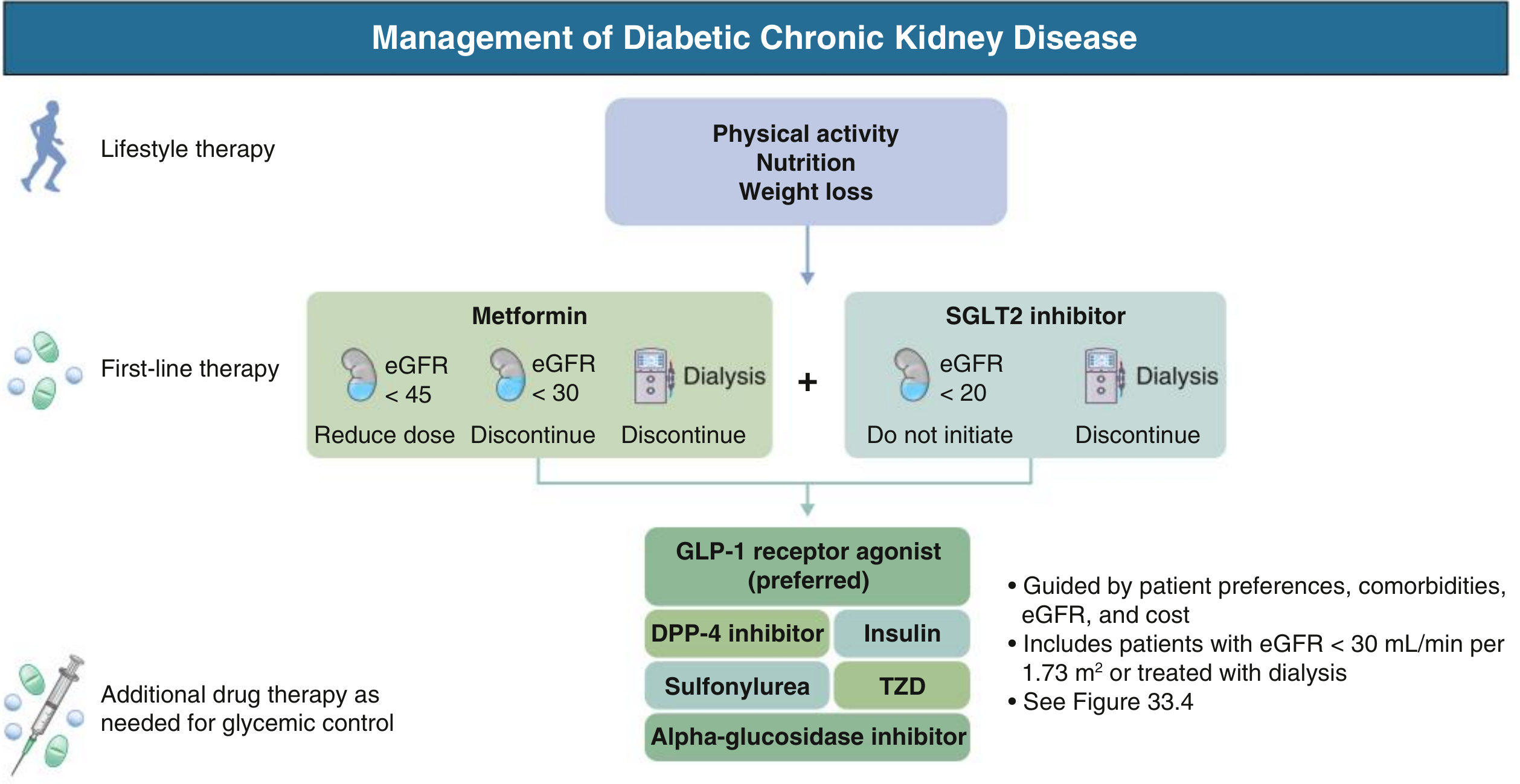
First-Line Therapy: Metformin + SGLT2 Inhibitor (Dual Backbone)
Most patients with T2D and CKD should be on both metformin AND an SGLT2 inhibitor as first-line therapy, with additional agents added as needed.
1. Metformin
- Preferred initial drug for T2D due to low cost, high efficacy, low hypoglycemia risk, weight- and lipid-lowering effects, and CV/mortality benefit.
- Renally eliminated - dose adjustment is needed:
| eGFR (mL/min/1.73 m²) | Action |
|---|---|
| ≥ 45 | Continue at full dose |
| 30-44 | Reduce dose to 500 mg twice daily |
| < 30 | Discontinue |
| Dialysis | Discontinue |
- Comprehensive Clinical Nephrology, 7th Ed., p. 458
2. SGLT2 Inhibitors (Preferred for CKD protection)
This is the most important drug class in T2D + CKD. SGLT2 inhibitors provide CV and renal protection far beyond their glycemic effect.
Key trial evidence:
- CREDENCE (canagliflozin): 30% reduction in composite ESKD/doubling of creatinine/CV death, halted early for efficacy
- DAPA-CKD (dapagliflozin): 39% relative risk reduction in sustained eGFR decline, ESKD, or CV/renal death - also effective in patients without diabetes
- EMPA-REG OUTCOME (empagliflozin): 39% reduction in worsening kidney disease; 55% reduction in kidney replacement therapy
- Meta-analysis: SGLT2 inhibitors reduce CKD progression by 37%, AKI risk by 23%, CV death/HF hospitalization by 23%
eGFR thresholds:
| eGFR | Action |
|---|---|
| ≥ 20 | Initiate and continue |
| < 20 | Do not initiate |
| On dialysis | Discontinue |
A 2025 network meta-analysis of 26 RCTs (143,296 patients) confirmed SGLT2 inhibitors ranked highest for composite renal outcomes (P-score 0.94), eGFR decline/RRT (P-score 0.99), MACE (0.93), and HF (1.00) among all antidiabetic drug classes. (PMID: 40798873)
3. GLP-1 Receptor Agonists (Preferred if SGLT2 not tolerated)
- Used when metformin + SGLT2 inhibitor is insufficient, not tolerated, or contraindicated
- Provide CV benefit: LEADER trial (liraglutide) showed 22% CV death reduction, 23% reduction in kidney endpoints
- Particularly effective for reducing macroalbuminuria (P-score 0.86) and stroke (P-score 0.83)
- Dose adjustment: Most are safe across CKD stages (renal dose adjustment not required for most agents); semaglutide is preferred
- Comprehensive Clinical Nephrology, 7th Ed., p. 459
4. Additional Agents (as needed for glycemic control)
| Drug Class | Notes in CKD |
|---|---|
| DPP-4 inhibitors | Safe but dose adjustment needed (except linagliptin - no renal adjustment); limited cardiorenal benefits vs SGLT2/GLP-1 |
| Sulfonylureas | Risk of hypoglycemia in CKD; if used, prefer glipizide (shorter-acting) |
| Insulin | Safe at all CKD stages; may need dose reduction as eGFR falls |
| TZDs (pioglitazone) | Avoid in fluid-retentive states; no dose adjustment needed |
| Alpha-glucosidase inhibitors | Avoid if eGFR < 30 |
5. Finerenone (Non-steroidal MRA) - Emerging Addition
- A selective nonsteroidal mineralocorticoid receptor antagonist
- FIDELIO-DKD trial: Reduced risk of kidney failure, CV death, MI, stroke, and HF hospitalization in T2D with CKD
- Recommended for patients with T2D + moderately-severely increased albuminuria + impaired eGFR, especially on top of ACEi/ARB therapy
- Comprehensive Clinical Nephrology, 7th Ed., p. 242
Summary: Drug Preference by CKD Stage
| CKD Stage | eGFR | Preferred Drugs |
|---|---|---|
| G1-G2 | > 60 | Metformin + SGLT2i |
| G3a | 45-59 | Metformin (full dose) + SGLT2i |
| G3b | 30-44 | Metformin (reduced dose) + SGLT2i + GLP-1 RA |
| G4 | 15-29 | Discontinue metformin; SGLT2i if eGFR ≥20; GLP-1 RA |
| G5/Dialysis | < 15 | GLP-1 RA, DPP-4i, insulin; stop SGLT2i and metformin |
Key principle: SGLT2 inhibitors are the cornerstone of CKD protection in T2D - their benefit is independent of glycemic control and persists even at lower eGFR levels. Metformin remains the glycemic backbone when tolerated. GLP-1 receptor agonists step in when either is contraindicated or additional CV/renal protection is needed.
Sources:
- Comprehensive Clinical Nephrology, 7th Edition (KDIGO 2022 guideline-based)
- Bramlage P et al., Network meta-analysis, 26 RCTs, 143K patients, Diabetes Obes Metab, 2025 (PMID: 40798873)
- CREDENCE, DAPA-CKD, EMPA-REG OUTCOME, FIDELIO-DKD trials
Lose motion medicine?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a complete, textbook-backed overview:
Medicines for Loose Motion (Diarrhea)
Treatment is organized by priority - rehydration first, then symptomatic drugs, then cause-specific medicines.
Step 1: Rehydration (Most Important!)
Oral Rehydration Solution (ORS) is the WHO-recommended first-line treatment for ALL types of diarrhea.
- ORS composition: water + glucose + sodium + potassium + chloride
- Prevents and treats dehydration
- Avoid high-sugar drinks (juice, soda) - they worsen fluid loss
- IV fluids (Normal saline, Ringer's lactate) needed if severe dehydration or vomiting prevents oral intake
"Adequate hydration is the most important treatment in managing diarrheal diseases." - The Washington Manual of Medical Therapeutics
Step 2: Symptomatic (Antidiarrheal) Drugs
These reduce stool frequency and urgency but do not treat the cause.
| Drug | Mechanism | Notes |
|---|---|---|
| Loperamide (Imodium) | Slows gut motility (opioid receptor agonist) | Most commonly used; no CNS effects; first choice for traveler's diarrhea |
| Diphenoxylate + Atropine (Lomotil) | Anticholinergic + opioid | Effective; atropine added to discourage misuse |
| Bismuth subsalicylate (Pepto-Bismol) | Antibacterial + anti-inflammatory | Useful in traveler's diarrhea; reduces stool frequency |
| Racecadotril (Acetorphan) | Enkephalinase inhibitor - reduces secretion | Preferred in children; does not cause rebound constipation |
| Kaolin-Pectin | Binds toxins, increases stool bulk | Mild effect; safe in children |
Caution: Avoid loperamide/diphenoxylate in bloody diarrhea, suspected C. difficile, or when fever is present - can worsen disease.
Step 3: Antibiotics (Only for Specific Causes)
Empiric antibiotics are only used in moderate-severe diarrhea with systemic symptoms (high fever, bloody stool, toxic appearance). Routine use is discouraged.
| Cause | Drug of Choice |
|---|---|
| Traveler's diarrhea (E. coli, Shigella) | Azithromycin (1st line), Ciprofloxacin, Rifaximin |
| C. difficile (pseudomembranous colitis) | Oral Vancomycin or Fidaxomicin |
| Amebiasis (Entamoeba histolytica) | Metronidazole, then Paromomycin/Iodoquinol |
| Giardiasis | Metronidazole or Tinidazole |
| Cholera | Doxycycline or Azithromycin + ORS |
| Typhoid-related diarrhea | Ceftriaxone or Azithromycin |
Important: Antibiotics in E. coli O157:H7 (Shiga toxin-producing) infections - especially in children and elderly - can increase risk of hemolytic-uremic syndrome (HUS). Avoid unless confirmed.
Step 4: Other Specific Agents
| Drug | Use |
|---|---|
| Probiotics (Lactobacillus, Saccharomyces boulardii) | Reduces duration; especially in antibiotic-associated diarrhea and children |
| Zinc supplementation | WHO-recommended in children under 5 with acute diarrhea (10-20 mg/day x 10-14 days) |
| Cholestyramine (bile acid binder) | Bile acid-induced diarrhea (post-cholecystectomy) |
| Octreotide | Hormone-mediated secretory diarrhea (VIPoma, carcinoid); refractory cases |
When to Seek Immediate Medical Attention
- Blood or mucus in stool
- High fever (>38.5°C)
- Signs of dehydration: no urine, sunken eyes, dry mouth, dizziness
- Diarrhea lasting > 48-72 hours
- Infant or elderly patient
- Recent hospital stay or antibiotic use (suspect C. difficile)
Quick Reference Summary
Loose Motion → ORS First
├── Mild/no fever → Loperamide + ORS
├── Traveler's diarrhea → Azithromycin + ORS
├── Bloody stool/fever → See doctor; investigate before treating
├── Children → Zinc + ORS + Racecadotril
└── C. difficile → Oral Vancomycin / Fidaxomicin
Sources: The Washington Manual of Medical Therapeutics; Sleisenger & Fordtran's Gastrointestinal and Liver Disease, 11th Ed.
Vomiting medicine
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a complete, textbook-backed breakdown of all vomiting medicines:
Medicines for Vomiting (Antiemetics)
Antiemetics work at different receptor sites in the brain and gut. The right drug depends on the cause of vomiting.
Drug Classes at a Glance
| Class | Mechanism | Key Drugs | Best For |
|---|---|---|---|
| 5-HT₃ Antagonists | Block serotonin receptors | Ondansetron, Granisetron | Chemotherapy, radiation, post-op, opioid-induced |
| D₂ Antagonists (Prokinetics) | Block dopamine receptors + enhance gut motility | Metoclopramide, Domperidone | Gastroparesis, gastric causes, general-purpose |
| Phenothiazines | Antidopaminergic | Prochlorperazine, Promethazine | General nausea, toxin/metabolic causes |
| Antihistamines | Block H₁ vestibular receptors | Dimenhydrinate (Dramamine), Meclizine, Promethazine | Motion sickness, inner ear, pregnancy |
| Anticholinergics | Block muscarinic receptors | Scopolamine (patch) | Motion sickness, post-op |
| NK₁ Receptor Antagonists | Block substance P | Aprepitant, Fosaprepitant, Rolapitant | Chemotherapy-induced vomiting (highly emetogenic) |
| Atypical Antipsychotics | Multiple receptors | Olanzapine, Haloperidol, Droperidol | Refractory vomiting, chemotherapy |
| Cannabinoids | CB₁ receptors | Dronabinol, Nabilone | Chemotherapy-induced, refractory |
| Corticosteroids | Anti-inflammatory | Dexamethasone | Chemotherapy combinations |
| Others | Various | Mirtazapine, Gabapentin, Amitriptyline | Chronic nausea, cyclic vomiting syndrome |
Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Table 48-2
1. Ondansetron (Zofran) - Most Widely Used
- Class: 5-HT₃ receptor antagonist
- Dose: 4-8 mg oral/IV/ODT (orally dissolving tablet)
- Best for: Post-operative nausea, chemotherapy, radiation, general vomiting
- Route: Oral, IV, IM, sublingual ODT (very convenient)
- Side effects: Headache, constipation, QT prolongation (high doses)
- Generally first-line in the emergency setting - inexpensive and well tolerated
- Rosen's Emergency Medicine, p. 294
2. Metoclopramide (Reglan/Perinorm) - Prokinetic
- Class: D₂ antagonist + 5-HT₄ agonist (prokinetic)
- Dose: 10-20 mg oral/IV/IM
- Best for: Gastroparesis, gastric motility issues, general vomiting
- Speeds up gastric emptying - excellent when vomiting is from a slow stomach
- Side effects: Extrapyramidal symptoms (tardive dyskinesia with prolonged use), restlessness
- Rosen's Emergency Medicine, p. 294
3. Domperidone (Motilium) - Peripheral Prokinetic
- Class: Peripheral D₂ antagonist
- Does not cross blood-brain barrier - fewer CNS/extrapyramidal side effects vs. metoclopramide
- Best for: Gastroparesis, nausea with bloating, GERD-related nausea
- Used widely in India, UK (not FDA-approved in USA)
4. Promethazine (Phenergan)
- Class: Phenothiazine + H₁ antihistamine
- Dose: 12.5-25 mg oral/IM/rectal
- Best for: Motion sickness, pregnancy nausea, general vomiting
- Caution: Very sedating; avoid IV use (risk of severe tissue injury); avoid in children < 2 years
5. Prochlorperazine (Stemetil/Compazine)
- Class: Phenothiazine / D₂ antagonist
- Dose: 5-10 mg oral/IM/IV; 25 mg rectal
- Best for: Severe nausea, migraine-associated vomiting, chemotherapy
- Side effects: Extrapyramidal reactions, drowsiness
6. Aprepitant (Emend) - NK₁ Antagonist
- Best for: Prevention of chemotherapy-induced nausea/vomiting (CINV), especially highly emetogenic regimens
- Used in combination with ondansetron + dexamethasone ("triple therapy" for CINV)
- Oral (day 1: 125 mg; day 2-3: 80 mg)
7. Dimenhydrinate / Meclizine - For Motion Sickness
- Class: Antihistamine (H₁ blocker)
- Best for: Motion sickness, vertigo, inner ear-related vomiting
- Scopolamine patch (behind ear): Best for motion sickness prevention - lasts 72 hours
Based on Cause - Which Drug to Choose
| Cause of Vomiting | Preferred Drug |
|---|---|
| Post-operative (PONV) | Ondansetron ± Dexamethasone |
| Chemotherapy (CINV) | Ondansetron + Aprepitant + Dexamethasone |
| Motion sickness | Dimenhydrinate, Meclizine, or Scopolamine patch |
| Gastroparesis | Metoclopramide, Domperidone |
| Pregnancy (morning sickness) | Doxylamine + B6 (1st line), Ondansetron, Metoclopramide |
| Hyperemesis gravidarum | Ondansetron IV, Promethazine, IV fluids |
| Gastroenteritis / general | Ondansetron 4 mg ODT, Metoclopramide |
| Migraine-related | Prochlorperazine, Metoclopramide |
| Vertigo/inner ear | Meclizine, Dimenhydrinate, Betahistine |
| Opioid-induced | Ondansetron, Haloperidol, Metoclopramide |
| Refractory/intractable | Olanzapine, Haloperidol, Lorazepam |
Important Complications of Prolonged Vomiting
| Complication | Cause |
|---|---|
| Dehydration / Hypovolemia | Loss of water and sodium |
| Metabolic alkalosis | Loss of H⁺ ions |
| Hypokalemia | Loss of potassium |
| Mallory-Weiss tear | Forceful retching tearing esophageal mucosa |
| Boerhaave syndrome | Esophageal perforation - surgical emergency (50% mortality if not treated within 24h) |
| Aspiration pneumonia | Especially in altered consciousness |
Rosen's Emergency Medicine, Table 25.6
When to Seek Medical Attention
- Vomiting blood (hematemesis)
- Unable to keep any fluids down for > 24 hours
- Signs of dehydration (dizziness, no urine, dry mouth)
- Associated severe headache, stiff neck, or visual changes (rule out brain causes)
- Vomiting after head injury
- In pregnancy with severe/persistent vomiting
Sources: Harrison's Principles of Internal Medicine 22nd Ed. (2025); Rosen's Emergency Medicine; Sleisenger & Fordtran's GI & Liver Disease
For Hadeace
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a complete, textbook-backed guide to headache medicines:
Medicines for Headache
Treatment depends on the type of headache. The three most common types are tension-type, migraine, and cluster headache.
For Simple / Tension-Type Headache (Most Common)
These are the everyday "stress headaches" - dull, band-like pressure around the head.
| Drug | Dose | Notes |
|---|---|---|
| Paracetamol (Acetaminophen) | 500-1000 mg every 4-6h (max 4g/day) | Safest first-line; no gastric irritation |
| Ibuprofen (NSAID) | 400 mg every 4-6h | Very effective; take with food |
| Aspirin | 300-600 mg | Also effective; avoid in children and peptic ulcer |
| Naproxen | 220-550 mg twice daily | Longer-acting NSAID |
| Paracetamol + Aspirin + Caffeine (e.g., Excedrin) | 2 tablets every 6h | Caffeine boosts analgesic effect |
| Diclofenac | 50 mg | Fast-acting NSAID |
Important: Do NOT take painkillers more than 10-15 days per month - this causes medication overuse headache (rebound headache), making things worse.
For Migraine Headache
Migraine is a severe, one-sided, pulsating headache lasting 4-72 hours, often with nausea, vomiting, and sensitivity to light and sound.
Step 1 - Mild to Moderate Migraine (Non-specific)
- Ibuprofen 400 mg or Naproxen 500 mg - take at first sign
- Paracetamol - less effective alone for migraine; works better with caffeine
- Aspirin 600-900 mg + metoclopramide (for nausea)
Step 2 - Moderate to Severe Migraine: Triptans (Migraine-Specific, First-Line)
Triptans are selective 5-HT₁B/1D receptor agonists - they constrict dilated cranial blood vessels and block pain pathways. They abort migraine in ~70% of patients.
| Triptan | Dose | Notes |
|---|---|---|
| Sumatriptan (Imitrex, Suminat) | 50-100 mg oral; 6 mg SC | Prototype; multiple routes (oral, nasal, SC) |
| Rizatriptan (Maxalt) | 5-10 mg oral | Among the most efficacious and fastest |
| Eletriptan (Relpax) | 40-80 mg oral | Highly efficacious |
| Zolmitriptan (Zomig) | 2.5 mg oral or nasal | Also available as nasal spray |
| Naratriptan (Naramig) | 2.5 mg oral | Slower onset, better tolerated, fewer side effects |
| Frovatriptan | 2.5 mg oral | Longest half-life - useful for menstrual migraine |
| Almotriptan | 12.5 mg oral | Well tolerated |
Tip: Rizatriptan and eletriptan are the most efficacious triptans. Clinical efficacy is related more to speed of absorption than potency. Take triptans as early as possible after headache onset (not during aura).
Contraindications for triptans: History of coronary artery disease, stroke, peripheral vascular disease, uncontrolled hypertension, pregnancy.
Triptan + Naproxen Combination
- Adding naproxen 500 mg to sumatriptan boosts initial effect AND reduces headache recurrence.
Step 3 - Ergotamine (Older, Second-Line)
- Ergotamine + caffeine (Cafergot): 1-2 tablets at onset (max 6/day, 10/week)
- Dihydroergotamine (DHE): IV/IM/SC for severe/refractory migraine in hospital
- More nausea than triptans; can cause rebound headache
Step 4 - Antiemetics (for nausea with migraine)
- Metoclopramide 10 mg or Prochlorperazine 10 mg - also have mild analgesic effect for migraine
- Ondansetron - if nausea/vomiting is prominent
Newer Drugs (CGRP-based)
| Drug | Class | Use |
|---|---|---|
| Rimegepant (Nurtec) | CGRP receptor antagonist (gepant) | Acute + preventive migraine |
| Ubrogepant (Ubrelvy) | CGRP receptor antagonist | Acute migraine |
| Lasmiditan (Reyvow) | 5-HT₁F agonist (ditan) | Acute migraine; safe in cardiovascular disease |
| Erenumab, Fremanezumab | Anti-CGRP monoclonal antibodies | Migraine prevention (monthly injection) |
Lippincott Pharmacology, 2024; Harrison's Principles, 22nd Ed. 2025
Migraine Prevention (Prophylaxis)
Used when migraines are frequent (≥4/month) or disabling.
| Drug | Class |
|---|---|
| Propranolol, Metoprolol | Beta-blockers (first-line) |
| Amitriptyline, Nortriptyline | Tricyclic antidepressants |
| Topiramate, Valproate | Anticonvulsants |
| Verapamil | Calcium channel blocker |
| Candesartan | ARB |
| OnabotulinumtoxinA (Botox) | For chronic migraine (≥15 days/month) |
| Anti-CGRP antibodies | Most effective newer option |
For Cluster Headache
Cluster headache is the most severe headache - described as a "hot poker through the eye," occurring in daily clusters.
| Drug | Use |
|---|---|
| 100% Oxygen (7-12 L/min x 15 min) | First-line acute treatment |
| Sumatriptan SC 6 mg | Most effective acute drug |
| Zolmitriptan nasal spray | Acute |
| Verapamil | Prevention (first-line) |
| Short-course Prednisolone | Bridge therapy during cluster period |
| Lithium | Prevention of chronic cluster |
Quick Reference Summary
Headache Type → Drug of Choice
─────────────────────────────────────
Tension headache → Paracetamol / Ibuprofen
Mild migraine → NSAIDs (Ibuprofen/Naproxen)
Moderate/severe → Triptans (Sumatriptan/Rizatriptan)
migraine
Migraine + nausea → Triptan + Metoclopramide
Cluster headache → Oxygen + Sumatriptan SC
Prevention → Propranolol / Topiramate / Anti-CGRP
When to See a Doctor Urgently ("Red Flag" Headaches)
- Thunderclap headache - worst headache of your life (rule out brain bleed)
- Headache with fever + neck stiffness (rule out meningitis)
- Headache after head injury
- New headache in someone over 50
- Headache with vision changes, weakness, or confusion
- Progressive worsening over days/weeks
Sources: Harrison's Principles of Internal Medicine, 22nd Ed. (2025); Lippincott Illustrated Reviews: Pharmacology; Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.