Oxygen transport
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content to write a detailed answer. Let me compile everything.
Oxygen Transport
Oxygen transport describes how O2 moves from the lungs to every metabolically active cell in the body. It involves two inseparable systems - the respiratory system (for gas exchange) and the cardiovascular system (for delivery).
1. Overview of Oxygen Delivery
Oxygen delivery (DO2) is defined as the volume of O2 delivered to the systemic vascular bed per minute:
DO2 = Cardiac Output (CO) × Arterial O2 Content (CaO2)
The ability to deliver O2 depends on:
-
The amount of O2 entering the lungs
-
Adequacy of pulmonary gas exchange
-
Blood flow to the tissue (cardiac output + local vascular tone)
-
The capacity of blood to carry O2 (hemoglobin concentration and its affinity for O2)
-
Ganong's Review of Medical Physiology, 26e, p. 641
2. Forms of Oxygen in Blood
O2 is carried in blood in two forms:
A. Dissolved O2 (~2%)
- Free in solution; follows Henry's Law: concentration = PO2 × 0.003 mL O2/100 mL blood/mmHg
- At a normal PaO2 of 100 mmHg → only 0.3 mL O2/100 mL blood
- Dissolved O2 is the ONLY form that exerts a partial pressure and drives diffusion
- Alone it is grossly inadequate: at rest, O2 consumption ~250 mL/min; dissolved O2 can deliver only ~15 mL/min
B. O2 Bound to Hemoglobin (~98%)
-
Reversibly bound to hemoglobin inside red blood cells
-
Provides the large bulk of O2 transport
-
Costanzo Physiology, 7e, p. 223
3. Hemoglobin Structure and O2 Binding
Hemoglobin is a globular protein with 4 subunits, each containing:
- A heme moiety (iron-binding porphyrin ring with Fe²+ in ferrous state)
- A polypeptide chain (α or β)
Adult hemoglobin A = α₂β₂ - two α chains and two β chains.
Each subunit binds one molecule of O2, so one Hb molecule binds 4 O2 molecules total.
The stepwise binding:
Hb₄ + O₂ ⇌ Hb₄O₂
Hb₄O₂ + O₂ ⇌ Hb₄O₄
Hb₄O₄ + O₂ ⇌ Hb₄O₆
Hb₄O₆ + O₂ ⇌ Hb₄O₈
Each reaction occurs in under 0.01 seconds.
Cooperativity (T-R model):
-
Deoxyhemoglobin = tense (T) configuration - low O2 affinity
-
After first O2 binds, bonds loosen into relaxed (R) configuration - exposes more binding sites
-
Net result: ~500-fold increase in O2 affinity with each successive binding
-
This cooperativity produces the characteristic sigmoid (S-shaped) dissociation curve
-
Ganong's Review, p. 641
4. O2-Binding Capacity and O2 Content
| Quantity | Formula | Normal Value |
|---|---|---|
| O2-binding capacity | [Hb] × 1.34 mL O2/g | 20.1 mL/100 mL blood |
| Arterial O2 content (CaO2) | (20.1 × 0.97) + 0.29 | ~19.8 mL/100 mL |
| Venous O2 content (CvO2) | (20.1 × 0.75) + 0.12 | ~15.2 mL/100 mL |
| O2 extraction per dL | CaO2 - CvO2 | ~4.6 mL/dL |
At rest, 250 mL O2/min is transported from blood to tissues (cardiac output ~5 L/min × 4.6 mL O2/dL × 10 dL/L).
- Ganong's Review, p. 641; Costanzo Physiology, p. 224
5. Oxygen-Hemoglobin Dissociation Curve (ODC)
The ODC plots % saturation of Hb against PO2:
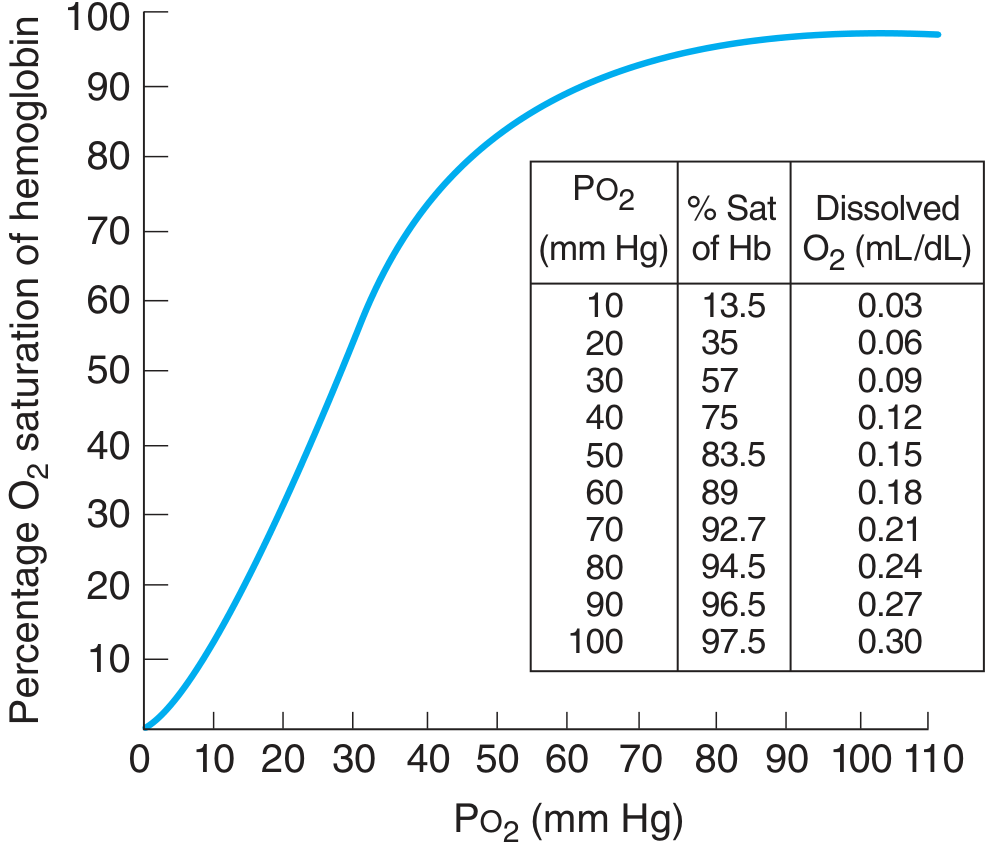
Key points from the curve:
- PO2 = 100 mmHg → SaO2 = 97.5% (arterial blood in lungs)
- PO2 = 40 mmHg → SaO2 = 75% (venous blood at rest)
- PO2 = 26 mmHg → SaO2 = 50% (this is the P50 - the standard reference point)
Clinical significance of the sigmoid shape:
- The flat upper portion (PO2 > 60 mmHg) means Hb stays well-saturated even if alveolar PO2 falls moderately
- The steep middle portion allows large amounts of O2 to be released with small PO2 drops in tissues
6. Factors Shifting the ODC
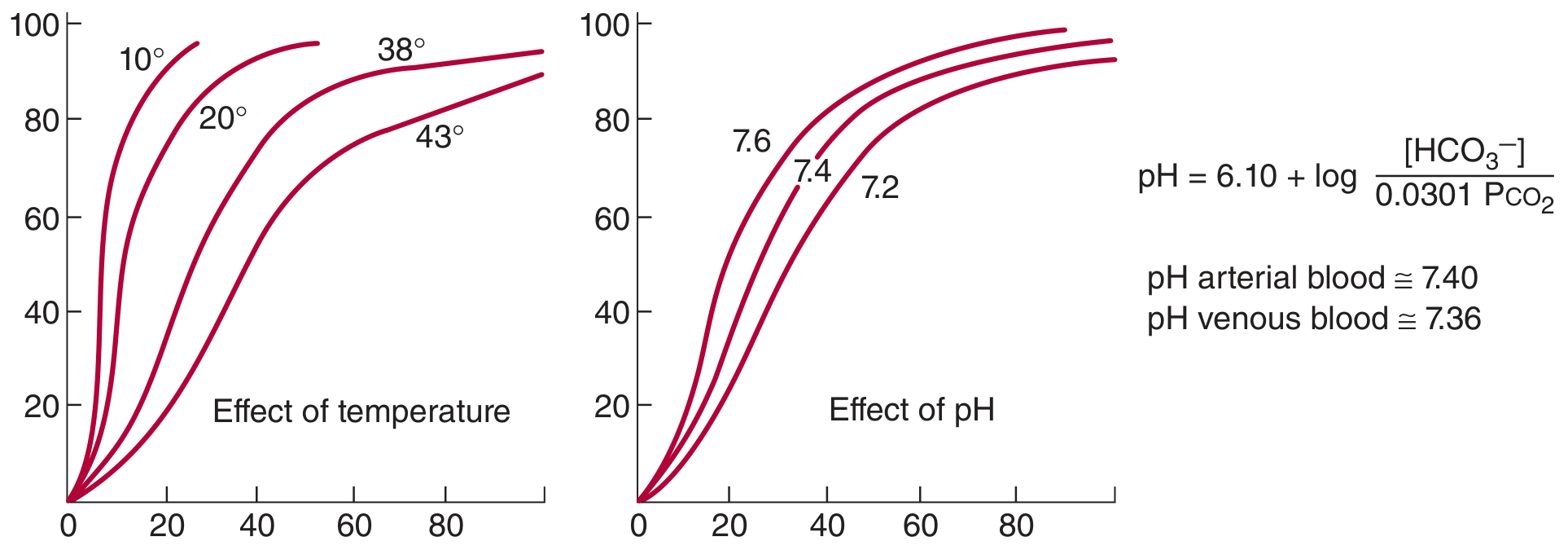
Right shift (↑ P50, ↓ O2 affinity - promotes O2 release to tissues):
| Factor | Change | Mechanism |
|---|---|---|
| pH | Decreases | Bohr effect - H+ binds deoxyhemoglobin preferentially |
| Temperature | Increases | Thermal disruption of Hb-O2 bonds |
| PaCO2 | Increases | CO2 → H+ → Bohr effect |
| 2,3-DPG | Increases | Binds β chains, stabilizes T state |
Left shift (↓ P50, ↑ O2 affinity - promotes O2 loading in lungs):
- Alkalosis (↑ pH), hypothermia, low 2,3-DPG, fetal hemoglobin (HbF)
- Carbon monoxide (CO) - shifts curve left AND reduces O2-carrying capacity
The Bohr Effect in context: In metabolically active tissues, CO2 and lactic acid accumulate → pH falls → curve shifts right → more O2 released exactly where it is needed.
- Ganong's Review, p. 642
7. Role of 2,3-DPG
2,3-Diphosphoglycerate (2,3-DPG) is formed in red cells via glycolysis (Embden-Meyerhof pathway). It binds the β chains of deoxyhemoglobin, stabilizing the T (low affinity) state:
HbO2 + 2,3-DPG ⇌ Hb-2,3-DPG + O2
Increased 2,3-DPG (right shift) occurs with:
- Chronic hypoxia (high altitude, anemia, COPD)
- Exercise (within 60 min)
- Thyroid hormones, growth hormone, androgens
Decreased 2,3-DPG (left shift) occurs with:
-
Acidosis (inhibits glycolysis)
-
Stored bank blood (key clinical consideration in transfusions)
-
Ganong's Review, p. 642
8. Hemoglobin Variants Affecting O2 Transport
| Variant | Defect | Effect on O2 transport |
|---|---|---|
| Methemoglobin | Fe²+ oxidized to Fe³+ (by nitrites, sulfonamides) | Cannot bind O2; also shifts ODC left in remaining Hb |
| Carboxyhemoglobin (HbCO) | CO binds with 210× affinity of O2 | Blocks O2 binding; left shift of ODC |
| Hemoglobin S (HbS) | β-chain mutation (αA₂βS₂); polymerizes when deoxygenated | Lower O2 affinity; sickling causes vascular occlusion |
| Fetal Hemoglobin (HbF) | γ chains replace β chains; lower 2,3-DPG binding | Higher O2 affinity - facilitates O2 transfer from mother to fetus |
9. O2 Delivery at the Tissue Level
In pulmonary capillaries:
- Venous blood arrives with PO2 ~40 mmHg; alveolar PO2 ~104 mmHg
- O2 diffuses down its gradient; Hb becomes ~97.5% saturated
- Due to ~2% shunt (bronchial circulation), systemic arterial PO2 ~95 mmHg
In peripheral capillaries:
-
Arterial PO2 = 95 mmHg; interstitial fluid PO2 ~40 mmHg; intracellular PO2 ~23 mmHg
-
O2 diffuses from capillary → interstitial fluid → cell
-
Tissue factors (↑ CO2, ↓ pH, ↑ temperature) enhance unloading via Bohr effect
-
Guyton and Hall Textbook of Medical Physiology, p. 522
10. Myoglobin - Intracellular O2 Storage
Myoglobin in skeletal muscle resembles hemoglobin but:
- Has only 1 subunit → binds 1 O2 molecule
- No cooperativity → hyperbolic (not sigmoid) dissociation curve
- Higher O2 affinity than Hb → curve is shifted LEFT of Hb curve
- Releases O2 only at very low PO2 (e.g., during intense exercise when blood flow is compressed)
- Acts as an O2 reservoir and facilitates intracellular O2 diffusion in sustained contractions
11. Summary: O2 Transport at a Glance
Lungs (PO2 ~104 mmHg)
→ O2 loads onto Hb (97.5% saturation)
→ Arterial blood carries ~19.8 mL O2/dL
→ Cardiac output delivers O2 to tissues
Tissues (PO2 ~40 mmHg; ↑ CO2, ↑ temp, ↓ pH)
→ Bohr effect + 2,3-DPG shift ODC right
→ O2 unloads (~4.6 mL O2/dL extracted at rest)
→ Venous blood returns (~15.2 mL O2/dL, 75% saturation)
| Parameter | Normal Value |
|---|---|
| Arterial PO2 (PaO2) | 95 mmHg |
| Venous PO2 (PvO2) | 40 mmHg |
| SaO2 | 97% |
| SvO2 | 75% |
| Hb concentration | 15 g/dL (men ~16, women ~14) |
| O2 carrying capacity | 20.1 mL/100 mL blood |
| O2 consumption at rest | ~250 mL/min |
| P50 | ~26-27 mmHg |
Sources: Ganong's Review of Medical Physiology 26e; Costanzo Physiology 7e; Guyton and Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.