MRI spine
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
MRI Spine: Normal Anatomy & Sequences
Source: Grainger & Allison's Diagnostic Radiology, 6th Ed.
Why MRI?
MRI is the method of choice for imaging the spine. It is non-invasive, carries no radiation, and exploits differences in proton concentration and relaxation times to visualize water, fat, bone, and soft tissue simultaneously. It provides unmatched contrast between the CSF, spinal cord, nerve roots, discs, and ligaments in a single examination.
Standard Routine Protocol
The recommended routine sequence set for spine MRI is:
| Sequence | Plane | Purpose |
|---|---|---|
| T1 weighted | Sagittal | Anatomy, bone marrow, fat |
| T2 weighted | Sagittal | Disc hydration, CSF, cord signal |
| STIR (or T2 fat-sat) | Sagittal | Oedema, ligamentous injury, metastases |
| T2 weighted | Axial | Neural foramina, canal, disc herniation |
| T1 weighted | Axial (lumbar) | Foraminal fat around nerve roots |
For the postoperative lumbar spine, add sagittal and axial T1 with gadolinium (Gd) to distinguish scar from recurrent disc herniation.
Individual Sequences Explained
T1 Weighted Imaging
- Parameters: short TR (300-700 ms), short TE (<30 ms), spin-echo (SE)
- Bright (high signal): fat, fatty bone marrow, subacute blood
- Dark (low signal): CSF, water, oedema, most tumours
- Best for: bone marrow, disc anatomy, osseous structures, soft-tissue planes
- Normal bone marrow is bright due to its fat content; a dark vertebral body on T1 should raise concern for infiltrative disease
T2 Weighted Imaging
- Parameters: long TR (2000-3000 ms), long TE (80-120 ms); fast spin-echo (FSE/TSE) is used in practice
- Bright: CSF (the hallmark), normal hydrated discs, free water, oedema
- Dark: cortical bone, ligaments, dehydrated/degenerate discs, fibrocartilage
- The spinal cord and nerve roots appear at intermediate signal, creating maximum contrast against the bright CSF - this "myelographic effect" is the reason T2 is so valuable
- Note: on FSE sequences fat remains relatively bright, which can mask vertebral metastases
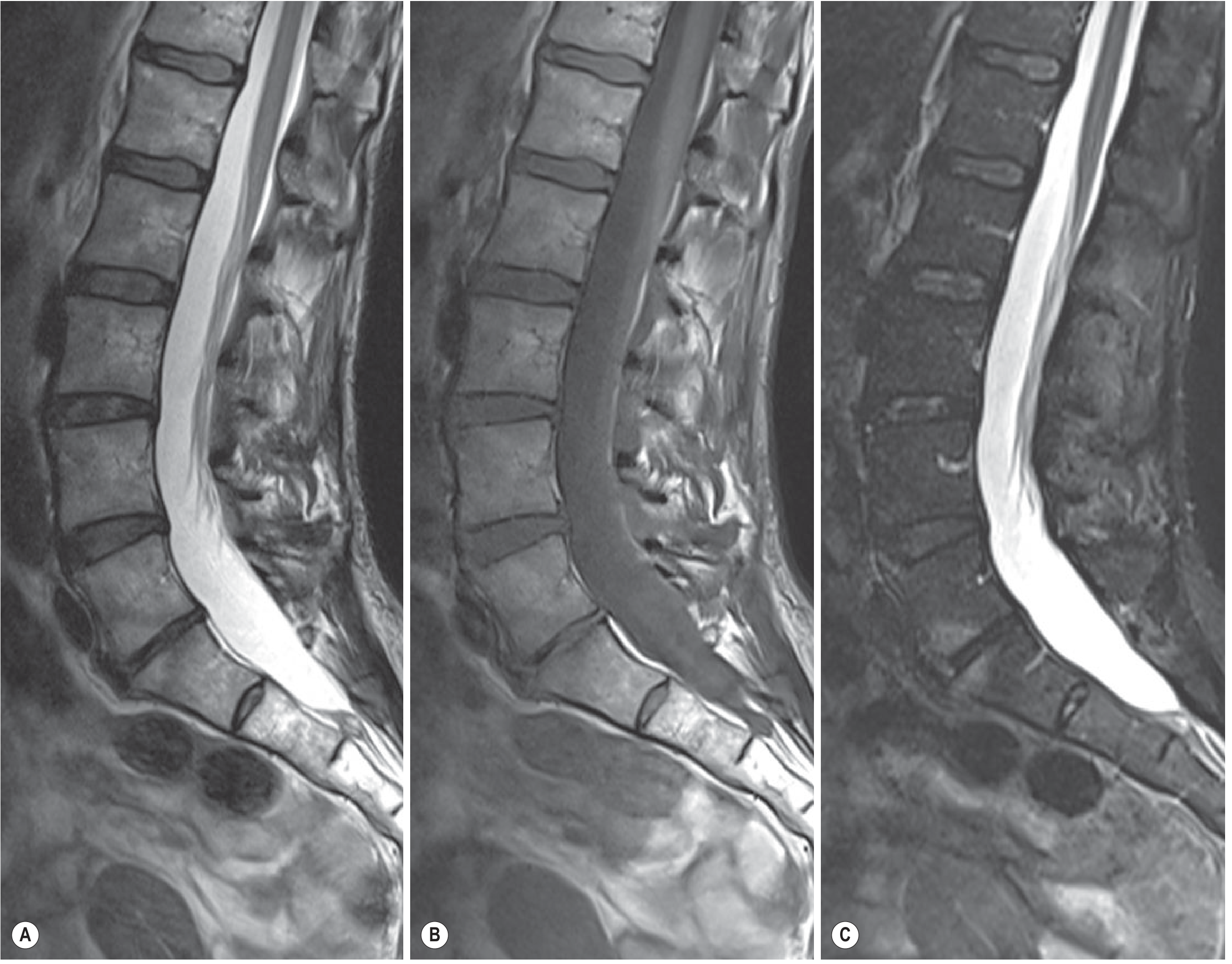
Fig. 47.17 below shows sagittal lumbar spine: T2 (A), T1 (B), and STIR (C). The T2 image demonstrates the classic bright CSF surrounding the cord and cauda equina. The STIR detects bone marrow oedema at L5-S1 not visible on T2.
STIR (Short Tau Inversion Recovery)
- Fat-suppression technique that nulls fat signal by choosing the appropriate inversion time (TI)
- Synergistic effect: prolonged T1 and T2 in abnormal tissue both increase signal, giving very high lesion-to-background contrast
- Excellent for: Modic changes, facet joint degeneration, vertebral metastases, occult fractures, acute vs. chronic fractures, multiple sclerosis plaques, ligamentous injury
- Advantage: works in low-field-strength magnets, insensitive to field inhomogeneity, suitable for large FOV spine coverage
- Disadvantage: noisier images, longer acquisition (more motion artefact in thoracic spine), cannot be combined with Gd (would suppress enhancing lesions)
Frequency-Selective Saturation (Dixon / FS T2)
- Radiofrequency pulse tuned to lipid resonant frequency suppresses fat specifically
- More complete fat suppression than STIR but requires high field strength and uniform field - less reliable at the periphery of large FOV
- Can be added to T1 (pre-Gd) to detect occult vertebral fractures
SPAIR (Spectral Presaturation Attenuated Inversion Recovery)
- Combines elements of frequency-selective sat and STIR
- Better image quality and SNR than STIR with shorter acquisition time
- Preferred over STIR for spine at 1.5T and 3T when field homogeneity is reliable
Gradient-Echo (GRE / GRE T2*)
- Shorter TE available compared to SE - reduces CSF pulsation artefacts
- Particularly useful in the cervical and thoracic spine
- Especially sensitive to haemosiderin/haemorrhage - a prognostic marker after cord injury
- Limitations: lower contrast for intramedullary lesions than FSE; susceptible to metal artefact (avoid near implants)
Gadolinium-Enhanced T1
- Standard dose: 0.1 mmol/kg IV
- Enhancement appears as T1 bright signal where the blood-brain barrier is disrupted or where tissue is hypervascular
- Key uses:
- Distinguish postoperative scar (enhances immediately, uniformly) from recurrent disc (peripheral/delayed enhancement)
- Tumour and infection delineation
- Leptomeningeal disease
- Pre- and post-contrast T1 images over the same region are essential for comparison
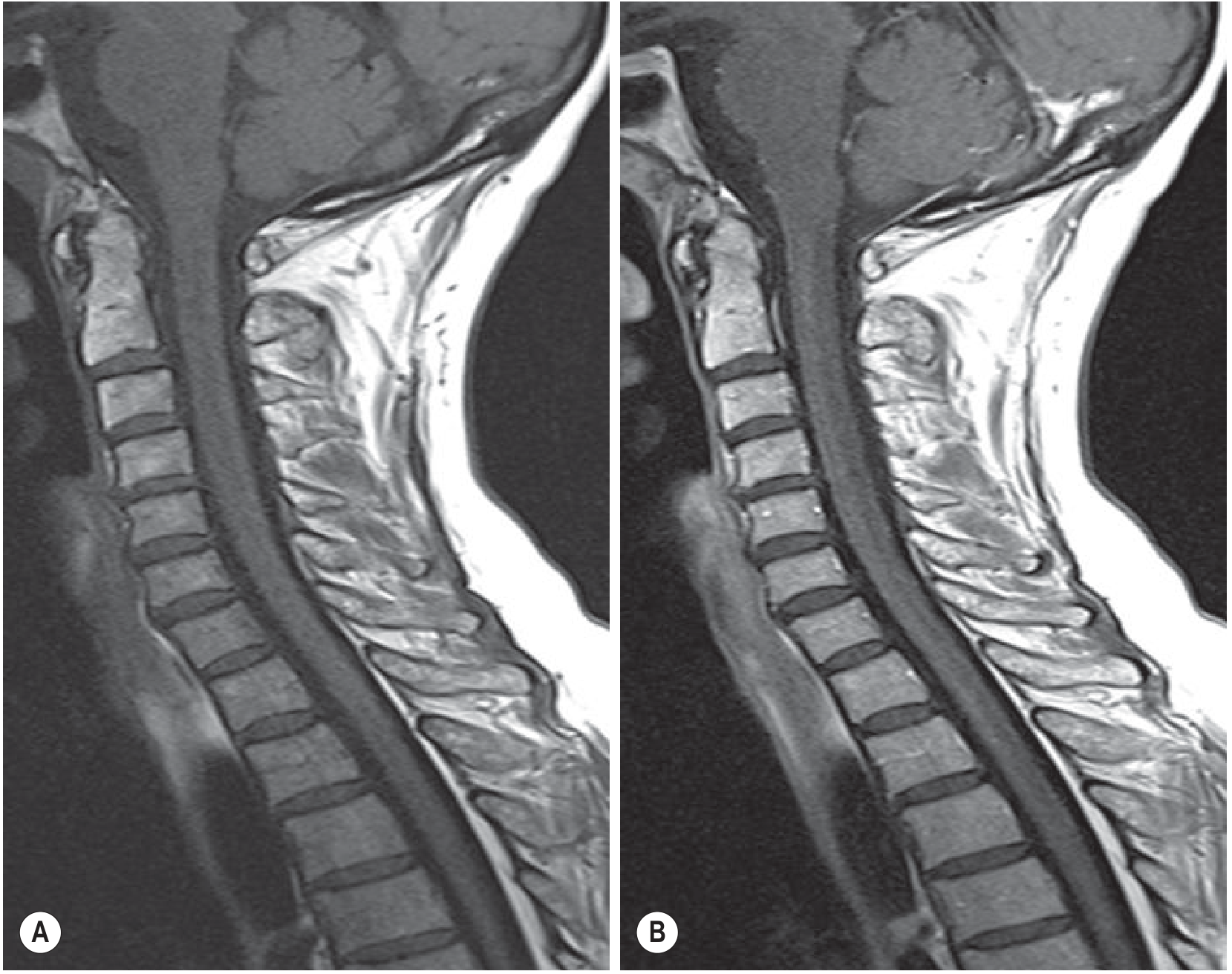
The image below shows sagittal T1 pre- and post-Gd of the cervical spine. Normal vascular enhancement is visible posterior to C2 and in the venous sinuses.
DWI (Diffusion-Weighted Imaging)
- Less established in the spine than brain due to field inhomogeneity, small cord diameter, and respiratory/cardiac motion
- Applications: spinal cord infarction, active MS lesions, cord compression assessment, drop metastases (in children), post-traumatic injury
- DTI (Diffusion Tensor Imaging) can evaluate structural integrity of white matter tracts - still largely a research tool
FLAIR
- Suppresses CSF signal (CSF appears black) - eliminates CSF pulsation artefacts
- Most lesions remain bright
- At 3T, T1-FLAIR has been shown to better delineate tissue interfaces (disc/CSF, soft tissue/bone) than standard T1 FSE in the lumbar spine
3D Imaging
- Uses thin slices (1-2 mm) with GRE or FSE; allows multiplanar reconstructions
- 3D FSE reduces CSF flow void artefacts
- Increasingly used for nerve root and foraminal assessment
Normal Anatomy: Signal Characteristics at a Glance
| Structure | T1 | T2 | STIR |
|---|---|---|---|
| CSF | Dark | Bright | Bright |
| Spinal cord | Intermediate | Intermediate | Intermediate |
| Nerve roots | Intermediate | Intermediate | Intermediate |
| Normal disc (nucleus pulposus) | Intermediate | Bright | Bright |
| Degenerate disc | Low | Dark | Dark |
| Fatty bone marrow | Bright | Intermediate | Suppressed (dark) |
| Cortical bone | Dark | Dark | Dark |
| Ligaments (PLL, LF) | Dark | Dark | Dark |
| Epidural fat | Bright | Intermediate | Suppressed |
| CSF pulsation artefact | Present | Present | Reduced |
Coil & Positioning
- Use a dedicated spine surface coil (or phased-array coil) for maximum SNR and resolution
- A spatial presaturation slab is placed over the larynx/carotid (cervical) or anterior chest/abdomen (thoraco-lumbar) to reduce vascular and respiratory artefacts
- Acquisition starts with a localiser (multidirectional low-resolution sequence) to plan optimal sagittal angulation
- Axial slices are then planned from high-resolution sagittal images, targeting regions of interest
Metal Artefact
When metallic implants are present, MARS (Metal Artefact Reduction Sequences) can be applied. Standard GRE sequences are most affected by metal - FSE-based sequences are more resistant.
Sources: Grainger & Allison's Diagnostic Radiology, Chapter 47 (Spine Imaging) and Chapter 52 (Cervical Spine Trauma)
Create a presentation on common MRI spine pathologies and their imaging features
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Running Command
mkdir -p /tmp/workspace/mri-spine-pptx && ls /tmp/workspace/mri-spine-pptx/
This is a shared conversation. Sign in to Orris to start your own chat.