I am a GP, I don't have any knowledge regarding ventilator, teach me about ventilator
Reading File
Finding Sources
Finding Sources
Searching the Web
mechanical ventilation basics for GP general practitioner overview 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile a thorough, GP-friendly guide on mechanical ventilation.
Mechanical Ventilation: A Complete Guide for the GP
This guide covers everything from first principles to practical management, written assuming no prior ICU/ventilator background.
1. WHY WE VENTILATE - The Basic Concept
Normal breathing is negative pressure: your diaphragm contracts, chest expands, pressure inside the thorax drops, and air flows in passively.
A mechanical ventilator does the opposite - it uses positive pressure to push air into the lungs. This is the single most important concept to grasp. Every mechanical ventilator in use today (except historical "iron lungs") works on positive pressure.
There are two goals a ventilator serves:
| Goal | What it fixes | Key measurement |
|---|---|---|
| Oxygenation | Gets O₂ into the blood | SpO₂, PaO₂ |
| Ventilation | Removes CO₂ from the blood | PaCO₂, pH |
These two are controlled by different ventilator knobs - a key point that trips up beginners.
2. WHEN TO VENTILATE - Indications
Think of mechanical ventilation whenever a patient cannot maintain adequate oxygenation or ventilation on their own. Some objective parameters:
| Criterion | Threshold to consider ventilation |
|---|---|
| PaO₂ on room air | < 50 mmHg |
| PaCO₂ | > 50 mmHg (without metabolic alkalosis) |
| PaO₂/FiO₂ ratio | < 300 mmHg |
| Respiratory rate | > 35 breaths/min |
| Tidal volume | < 5 mL/kg |
| Vital capacity | < 15 mL/kg |
| Max inspiratory force | weaker than -25 cmH₂O |
Clinical situations that commonly lead to ventilation:
-
Severe pneumonia / ARDS
-
Acute exacerbation of COPD or asthma
-
Cardiac arrest (post-ROSC)
-
Severe sepsis with respiratory failure
-
Drug overdose causing respiratory depression
-
Neuromuscular disease (GBS, myasthenia crisis)
-
Head injury (to control CO₂ and ICP)
-
Post-operative airway protection
-
Morgan and Mikhail's Clinical Anesthesiology 7e, p. 2519
3. TYPES OF VENTILATION
Non-Invasive (NIV)
- Uses a tight-fitting mask - no tube in the trachea
- Types: CPAP (one level of pressure) or BiPAP (two levels: IPAP and EPAP)
- Best for: COPD exacerbations, cardiogenic pulmonary oedema, obstructive sleep apnoea
- Advantage: avoids intubation risks (infection, trauma, sedation)
- Contraindications: vomiting, inability to protect airway, facial trauma, uncooperative patient
Invasive (IMV)
- Requires an endotracheal tube (ETT) or tracheostomy
- Used when NIV fails or is contraindicated
- Allows full control over all ventilator parameters
4. THE KEY VENTILATOR PARAMETERS
Understanding 6 core settings gives you a working foundation:
a) Tidal Volume (Vt)
- The volume delivered with each breath
- Target: 6-8 mL/kg ideal body weight (IBW)
- Low tidal volumes (lung-protective) are standard of care in ARDS
- Higher volumes cause lung injury (volutrauma)
b) Respiratory Rate (RR)
- Breaths delivered per minute by the machine
- Typical adult starting point: 12-16 breaths/min
- RR × Vt = Minute Ventilation (MV) - this determines CO₂ clearance
- To reduce CO₂: increase RR or Vt. To raise CO₂: decrease them.
c) FiO₂ (Fraction of Inspired Oxygen)
- The concentration of oxygen delivered (0.21 = room air, 1.0 = 100%)
- Start at 1.0 (100%) in an emergency, then wean down to keep SpO₂ 94-98%
- Prolonged high FiO₂ causes oxygen toxicity - wean as quickly as safe
d) PEEP (Positive End-Expiratory Pressure)
- A baseline positive pressure maintained at the end of every expiration
- Keeps alveoli from collapsing (recruits lung)
- Typical starting PEEP: 5 cmH₂O
- In ARDS, higher PEEP is often used (up to 18-24 cmH₂O) alongside lower FiO₂ (see table below)
- Risks at high PEEP: reduced venous return, decreased cardiac output, barotrauma
e) Peak Pressure
- The highest pressure reached during a breath
- Reflects resistance in the airways (ETT, bronchospasm, secretions)
- Safe limit: generally < 40 cmH₂O
f) Plateau Pressure
- The pressure measured after a brief inspiratory hold (air stops flowing, pressure equilibrates)
- Reflects the stiffness (compliance) of the lung, not airway resistance
- Safe limit: < 30 cmH₂O
- High plateau = poor compliance (ARDS, pneumonia, pulmonary oedema)
- High peak but normal plateau = airway resistance problem (bronchospasm, ETT kink, secretions)
Here is what a normal ventilator waveform looks like (Volume Control mode):
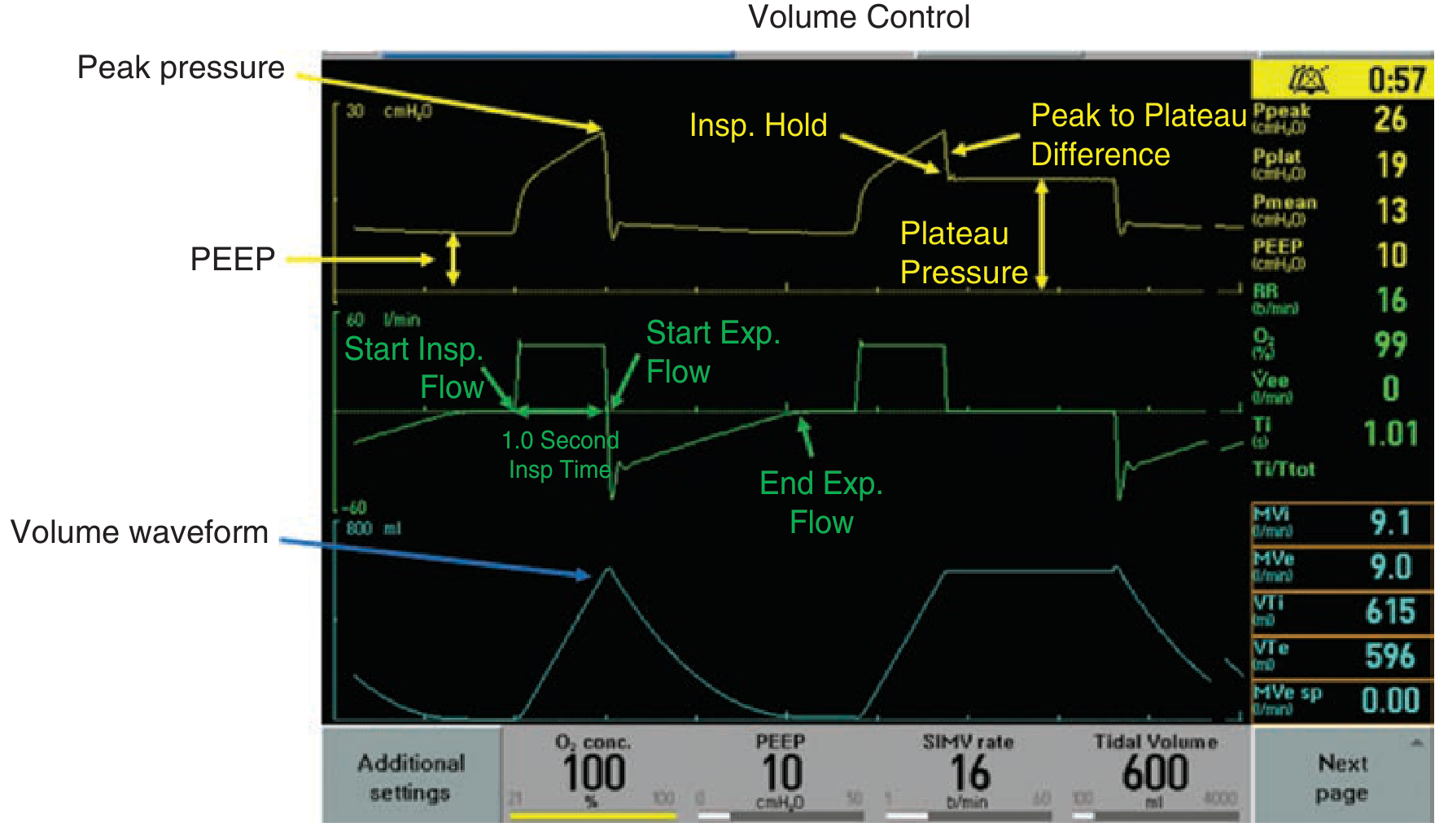
Normal ventilator waveforms for volume control. Yellow = pressure, green = flow, blue = volume. - Tintinalli's Emergency Medicine
5. VENTILATOR MODES
A "mode" is the pattern of how the ventilator delivers breaths. There are three main types:
A) Assist-Control (AC) - the most common starting mode
- The ventilator delivers a full breath every time:
- The set time interval arrives (machine-triggered), OR
- The patient makes any inspiratory effort (patient-triggered)
- Patient can breathe as fast as they want - every breath gets full support
- Best for: newly intubated, severely ill, or apnoeic patients
- Risk: patient can overbreathe (hyperventilate) and cause respiratory alkalosis
AC has two subtypes:
- Volume Control AC (VCAC): you set Vt, the machine varies pressure to deliver it
- Pressure Control AC (PCAC): you set inspiratory pressure, Vt varies depending on lung compliance
B) SIMV (Synchronised Intermittent Mandatory Ventilation)
- The machine delivers a set number of mandatory breaths per minute
- Between mandatory breaths, the patient breathes spontaneously (often with pressure support)
- Advantage: allows gradual weaning - reduce mandatory rate as patient improves
- Risk: patient must do significant work on spontaneous breaths; can be tiring in sick patients
C) Pressure Support Ventilation (PSV)
- No mandatory rate - patient triggers every breath
- Ventilator provides a set pressure boost with each patient breath
- Patient controls their own RR and Vt
- Best for: weaning, trial before extubation
- If patient stops breathing, no backup - only used in patients with reliable respiratory drive
D) CPAP
- A constant pressure maintained throughout the breathing cycle
- Patient breathes entirely spontaneously
- Used mainly for non-invasive ventilation (sleep apnoea, mild cardiogenic oedema)
| Mode | Who triggers? | Who controls Vt? | Best use |
|---|---|---|---|
| AC Volume Control | Machine or patient | You (set Vt) | Acute respiratory failure |
| AC Pressure Control | Machine or patient | Lung compliance | ARDS, stiff lungs |
| SIMV | Machine (mandatory) + patient (spontaneous) | Mixed | Weaning |
| Pressure Support | Patient only | Lung compliance | Weaning, trials |
| CPAP | Patient only | Patient | Non-invasive support |
- Tintinalli's Emergency Medicine, p. 232; Morgan & Mikhail Clinical Anesthesiology 7e, p. 2524-2526
6. INITIAL VENTILATOR SETTINGS (A PRACTICAL STARTING POINT)
For a typical adult intubated for acute respiratory failure:
| Parameter | Starting Value |
|---|---|
| Mode | AC Volume Control |
| Tidal Volume | 6 mL/kg IBW |
| Rate | 14-16 breaths/min |
| FiO₂ | 1.0 (100%) - wean down |
| PEEP | 5 cmH₂O (increase if hypoxic) |
| Peak pressure alarm | Set at 40 cmH₂O |
| I:E ratio | 1:2 (inspiration: expiration) |
IBW calculation (male): 50 + 2.3 × (height in inches - 60)
IBW calculation (female): 45.5 + 2.3 × (height in inches - 60)
7. OXYGENATION vs. VENTILATION - How to Fix Each
This is the most practically important concept for managing a ventilated patient:
Fixing Low SpO₂ / Low PaO₂ (Oxygenation problem):
- Increase FiO₂ (quickest fix)
- Increase PEEP (recruits collapsed alveoli)
- Treat the underlying cause (drain pneumothorax, suction secretions, bronchodilators)
Fixing High PaCO₂ / Low pH (Ventilation problem):
- Increase Respiratory Rate
- Increase Tidal Volume
- Check for and treat auto-PEEP (see below)
8. SPECIAL CLINICAL SCENARIOS
ARDS (Acute Respiratory Distress Syndrome)
- Use lung-protective ventilation: Vt 6 mL/kg IBW, plateau pressure < 30 cmH₂O
- Higher PEEP strategy (per ARDS Network tables):
| FiO₂ | 0.3 | 0.4 | 0.5 | 0.6 | 0.7 | 0.8 | 0.9 | 1.0 |
|---|---|---|---|---|---|---|---|---|
| PEEP | 5 | 5-8 | 8-10 | 10 | 10-14 | 14 | 14-18 | 18-24 |
- Permissive hypercapnia is acceptable (allow pH down to 7.2)
Obstructive Lung Disease (COPD / Asthma)
- Major risk: air trapping / auto-PEEP / dynamic hyperinflation
- Set a slow rate (10-14 breaths/min) to allow full exhalation
- Use a longer expiratory time (I:E ratio of 1:3 or 1:4)
- Tolerate hypercapnia - permissive hypoventilation, target pH ≥ 7.20
- Check for auto-PEEP by end-expiratory hold manoeuvre
- If patient suddenly becomes hypotensive on the ventilator: suspect tension pneumothorax or severe auto-PEEP - disconnect from vent for 15-20 seconds
- Tintinalli's Emergency Medicine, p. 233-234
9. COMPLICATIONS OF MECHANICAL VENTILATION
| Complication | Mechanism | Prevention |
|---|---|---|
| Barotrauma (pneumothorax, pneumomediastinum) | High peak pressures | Keep peak < 40 cmH₂O, plateau < 30 |
| Volutrauma | Overdistension of alveoli | Low Vt (6 mL/kg) |
| Atelectrauma | Repetitive alveolar collapse/reopening | Adequate PEEP |
| Ventilator-Associated Pneumonia (VAP) | Bacterial colonisation via ETT | Head-of-bed elevation 30-45°, oral hygiene, minimise sedation |
| Haemodynamic compromise | Positive pressure reduces venous return | Adequate fluid status, avoid excessive PEEP |
| Oxygen toxicity | Reactive oxygen species at high FiO₂ | Wean FiO₂ to < 0.6 as soon as safely possible |
| Ventilator-induced diaphragm dysfunction | Disuse atrophy | Daily weaning trials, avoid full paralysis unless needed |
| Delirium | Sedation, immobility, ICU environment | Minimise sedation (propofol/dexmedetomidine over benzodiazepines), early mobilisation |
10. WEANING AND EXTUBATION
Weaning means gradually reducing ventilator support so the patient resumes spontaneous breathing. Key principles:
Daily Spontaneous Breathing Trial (SBT):
Once daily, check if the patient can breathe with minimal support:
- Reduce to Pressure Support of 5-8 cmH₂O + PEEP 5 cmH₂O (a "T-piece trial")
- Watch for 30-120 minutes for signs of failure (RR > 35, SpO₂ < 90%, agitation, diaphoresis)
- If tolerated: consider extubation
Before extubation, check:
- Is the underlying problem resolved?
- Is the patient awake and following commands?
- Can they protect their airway? (cough, gag)
- Cuff-leak test positive? (rules out subglottic oedema)
- RSBI (Rapid Shallow Breathing Index = RR/Vt in L) < 105 = likely to succeed
11. SEDATION AND ANALGESIA IN VENTILATED PATIENTS
Ventilated patients are often distressed and uncomfortable. Best practice:
-
Analgesia first: treat pain before targeting sedation (fentanyl, morphine)
-
Sedation target: RASS score -2 to 0 (light sedation, responds to voice)
-
Prefer: propofol or dexmedetomidine over benzodiazepines (less delirium, less prolonged ventilation)
-
Avoid: prolonged benzodiazepine infusions - associated with higher mortality, more delirium
-
Daily sedation holds: allow reassessment, reduce total drug exposure
-
Tintinalli's Emergency Medicine, p. 234-235
12. QUICK REFERENCE SUMMARY
VENTILATOR CHEAT SHEET FOR INITIAL SETUP
=========================================
Mode: AC Volume Control
Vt: 6 mL/kg IBW
Rate: 14-16/min
FiO2: 1.0 → wean to keep SpO2 94-98%
PEEP: 5 cmH2O (start)
Alarm (High): 40 cmH2O
Low SpO2: ↑ FiO2 first, then ↑ PEEP
High CO2: ↑ RR or ↑ Vt
High Peak: Check ETT kink, bronchospasm, secretions
High Plateau: Low compliance (ARDS) → reduce Vt, ↑ PEEP
A useful video walkthrough of ventilator modes and settings (for visual learning):
Key sources used:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide (Chapter 29B)
- Morgan & Mikhail's Clinical Anesthesiology 7e (Chapter 58)
- Morgan & Mikhail's Clinical Anesthesiology 7e, Table 58-4 (indicators for MV)
- Merck Manual: Overview of Mechanical Ventilation
- EMOttawa: Mechanical Ventilation Basics
This is a shared conversation. Sign in to Orris to start your own chat.