
IMG_20260513_123937.jpg
Here is given three documents, analyse them properly and answer the diagnosis of given image, with every aspect where there can be question can be arises. Answer the bone fracture x-ray in given image.
Reading File
Reading File
Finding Sources
Finding Sources
Running Command
cd /home/daytona/workspace/attachments/623eca53-7ff1-4013-8d7b-efa1ac97562c && p…
Reading File
Running Command
cd /home/daytona/workspace/attachments/623eca53-7ff1-4013-8d7b-efa1ac97562c && p…
Reading File
Running Command
cd /home/daytona/workspace/attachments/623eca53-7ff1-4013-8d7b-efa1ac97562c && p…
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Searching Images
Galeazzi fracture forearm distal radius fracture DRUJ dislocation X-ray
Loading Image
I now have all the information needed for a comprehensive analysis. Let me provide a complete, detailed answer.
X-Ray Analysis: Galeazzi Fracture-Dislocation
Patient Demographics (from film label)
- Name: Isaev A.V.
- DOB: 25-12-1955 (age ~66 at time of X-ray)
- Sex: Male
- Date of study: 08-10-2022
- Side: Left (L marker visible)
- View: AP/lateral of left forearm
X-Ray Findings
What is visible on the film:
- Fracture of the distal-to-middle third of the radial shaft — complete, displaced, with angulation and foreshortening of the radius
- The ulna appears intact proximally but there is visible disruption at the wrist level
- Significant displacement of the fracture fragments — the distal radial fragment is shortened and angulated (dorsal/volar)
- Disruption of the Distal Radioulnar Joint (DRUJ) — the ulnar head is displaced relative to the sigmoid notch of the radius, indicating DRUJ dislocation/subluxation
- Soft tissue swelling evident around the fracture site
- No visible comminution — fracture appears as a simple (22-A2) or possibly oblique/transverse pattern
Primary Diagnosis
GALEAZZI FRACTURE-DISLOCATION
(aka "Piedmont fracture" / "Reverse Monteggia" / "Fracture of Necessity")
A Galeazzi fracture is defined as a fracture of the radial shaft (middle to distal third) combined with dislocation or subluxation of the Distal Radioulnar Joint (DRUJ).
This is a classic and confirmed pattern on this film.
Classification
OTA/AO Classification:
- 22-A2.3 (Simple radial fracture with DRUJ dislocation = Galeazzi type)
- Code breakdown: 22 = forearm shaft; A = simple fracture; 2 = radius; .3 = with DRUJ dislocation
Galeazzi Subclassification (by distance from articular surface):
- Type I: Fracture within 7.5 cm of the distal radial articular surface → higher DRUJ instability (likely here given the distal location visible)
- Type II: More proximal
In this patient, the fracture appears to be in the distal-to-middle third, placing it in Type I territory, which carries a significantly higher rate of DRUJ instability requiring operative stabilization.
DRUJ Dislocation Subtype:
- Simple (reducible after radial ORIF) vs. Complex (irreducible — interposition of ECU or EDM tendons)
- This distinction is determined intraoperatively.
Mechanism of Injury
| Mechanism | Details |
|---|---|
| Primary | Fall on outstretched hand in forced hyperpronation |
| Biomechanics | Torsional + axial loading → radial shaft fracture → proximal-to-distal propagation through interosseous membrane → rupture of distal radioulnar ligaments → TFCC injury → DRUJ instability |
| Alternative | Direct dorsolateral blow to the forearm |
The sequence of soft tissue disruption:
- Radial shaft fractures
- Interosseous membrane tears (distal to proximal)
- Distal radioulnar ligaments rupture
- TFCC (triangular fibrocartilage complex) injury
- DRUJ becomes unstable/dislocated
Clinical Features (What to Examine)
| Feature | Finding |
|---|---|
| Deformity | Visible forearm deformity at fracture site |
| DRUJ instability | Prominent ulnar head at wrist (piano key sign), tenderness over DRUJ |
| Range of motion | Painful/reduced forearm rotation (pronation/supination) |
| Neurovascular | Check anterior interosseous nerve (AIN), radial nerve, radial artery |
| Soft tissues | Swelling, ecchymosis over mid-distal forearm and wrist |
| Open vs closed | Examine skin integrity; ulnar subcutaneous border prone to skin breach |
Radiographic Diagnostic Criteria (What to Look For)
On AP view:
- DRUJ space widened >2 mm
- Relative shortening of the radius (radial shortening >5 mm suggests DRUJ disruption)
- Fracture at base of ulnar styloid (strong indicator of DRUJ disruption)
On Lateral view:
- Dorsally angulated radial fracture
- Dorsal displacement of the ulnar head
Additional views recommended:
- Dedicated wrist AP + lateral (assess DRUJ, ulnar variance)
- Elbow AP + lateral (rule out associated elbow injury, confirm PRUJ intact)
Differential Diagnosis
| Condition | Key Distinction |
|---|---|
| Monteggia fracture | Ulnar shaft fracture + radial HEAD dislocation at elbow (not wrist) |
| Nightstick (isolated ulnar) fracture | Ulnar shaft only, no DRUJ/joint dislocation |
| Both-bone forearm fracture | Both radius AND ulna shaft fractures |
| Essex-Lopresti lesion | Radial head fracture + interosseous membrane disruption + DRUJ injury (triad) |
| Colles fracture | Distal radial metaphysis (not shaft) fracture |
Treatment
In Adults: "Fracture of Necessity" — Operative Surgery Is Mandatory
Conservative management in adults has poor outcomes due to deforming muscular forces (pronator quadratus, brachioradialis) causing re-displacement even in a cast.
Step-by-Step Surgical Management:
- ORIF of the radius with a 3.5 mm dynamic compression plate (DCP) — gold standard
- Anatomic reduction and rigid fixation restores radial length and alignment
- Restores DRUJ congruency indirectly in most cases
- Assess DRUJ stability after radial fixation:
- If stable → immobilize in supination in long-arm cast ×4-6 weeks
- If unstable (simple dislocation) → closed reduction of DRUJ + supination casting or temporary radioulnar Kirschner wire fixation
- If irreducible (complex dislocation) → open DRUJ, remove interposed ECU/EDM, repair TFCC ± temporary K-wire
- TFCC repair if significant ligamentous injury identified
In Children: Closed reduction + long-arm casting (most cases)
Complications
| Complication | Notes |
|---|---|
| Malunion | Most common if managed non-operatively |
| Nonunion | Less common with plating |
| DRUJ chronic instability/dislocation | If initial DRUJ disruption missed |
| Limited forearm rotation | Due to malunion or DRUJ arthrosis |
| Interosseous membrane synostosis | Radioulnar synostosis (rare) |
| Anterior interosseous nerve palsy | From traction during injury or surgery |
| Compartment syndrome | Emergency → fasciotomy |
| Refracture | After implant removal |
Key Teaching Points for Exams
- "Fracture of Necessity" — Galeazzi fractures in adults ALWAYS require operative treatment; no exceptions
- Never miss the DRUJ — A solitary radial shaft fracture must prompt dedicated wrist views; DRUJ dislocation occurs in ≥25% of radial shaft fractures
- Galeazzi vs Monteggia mnemonic:
- Galeazzi = Gadget at the wrist (DRUJ affected)
- Monteggia = Middle/Monteggia at the elbow (PRUJ/radial head affected)
- DRUJ widening >2 mm on AP or ulnar styloid base fracture = presume DRUJ disruption
- Radial shortening >5 mm correlates with DRUJ ligamentous incompetence
- Type I Galeazzi (fracture within 7.5 cm of distal radius joint surface) = highest rate of DRUJ instability
Reference Images
Classic Galeazzi fracture-dislocation AP and lateral views for comparison:
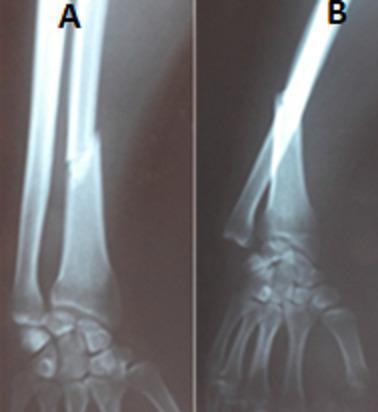
AP (A) and lateral (B) views showing radial shaft fracture at the middle-distal third with DRUJ disruption — identical pattern to the patient's film.
Sources consulted:
- Rockwood and Green's Fractures in Adults, 10th ed. 2025 — Chapter 42 (Diaphyseal Fractures of Radius/Ulna)
- Rosen's Emergency Medicine — Galeazzi Fracture section
- Miller's Review of Orthopaedics, 9th ed.
- Tintinalli's Emergency Medicine
- Provided course documents: Practice Bones and Joints Part 1 (2022), Bones 4th Year
This is a shared conversation. Sign in to Orris to start your own chat.