Babessiois
Reading File
Finding Sources
Searching PubMed
babesiosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Babesiosis
Definition
Babesiosis is a tick-borne, malaria-like disease caused by intraerythrocytic sporozoan (protozoan) parasites of the genus Babesia. They infect red blood cells and produce a hemolytic illness that can range from subclinical to rapidly fatal.
- Goldman-Cecil Medicine, p. 3450; Robbins Pathology, p. 374
Causative Organisms & Vectors
| Species | Region | Vector |
|---|---|---|
| B. microti | Northeastern & upper Midwestern USA, parts of Asia/Europe | Ixodes scapularis (deer tick) |
| B. divergens | Europe | Ixodes ricinus (sheep/castor bean tick) |
| B. duncani (WA-1) | Western USA (California, Washington) | Ixodes spp. |
| B. venatorum / B. crassa | Northeastern China | Ixodes spp. |
Key reservoirs: white-footed mouse (Peromyscus leucopus) and white-tailed deer (Odocoileus virginianus). B. microti survives well in refrigerated blood, making transfusion-transmitted babesiosis a real risk - it is one of the most commonly reported transfusion-transmitted diseases in the USA.
- Goldman-Cecil Medicine, p. 3445-3450; Rosen's Emergency Medicine, p. 2702
Epidemiology
-
~2,000 cases/year reported in the USA (largely underreported); became nationally reportable in 2011.
-
95% of US cases come from 7 states: Connecticut, Massachusetts, Minnesota, New Jersey, New York, Rhode Island, and Wisconsin.
-
Seasonal peak: May to August (nymphal tick-feeding period); average patient age 62, two-thirds male.
-
Co-infection with Lyme disease is common (same tick vector, same reservoirs) - up to 50% of babesiosis cases in some series.
-
250 transfusion-acquired cases of B. microti reported; transplacental transmission documented.
-
Rosen's Emergency Medicine, p. 2701; Goldman-Cecil Medicine, p. 3445
Pathophysiology
-
The nymphal Ixodes tick (only 1-2 mm, easily overlooked) transmits the parasite during feeding; >50% of patients cannot recall a tick bite.
-
Sporozoites enter RBCs and undergo asexual reproduction (merozoites), causing hemolysis.
-
Pro-inflammatory cytokines (TNF-α, IFN-γ, IL-2, IL-6, E-selectin, VCAM-1, ICAM-1) drive fever, sweats, chills, and headache.
-
Severe disease involves vascular stasis contributing to end-organ dysfunction.
-
Parasitemia ranges from <1% in mild cases to 70-85% in asplenic/immunocompromised patients.
-
Goldman-Cecil Medicine, p. 3450
Clinical Features
Incubation period: 1-4 weeks after tick exposure (up to 9 weeks after blood transfusion).
Mild to moderate (most common):
- Gradual onset of flu-like illness: malaise, fatigue, fever (up to 40°C), chills, sweats, myalgias, headache, anorexia
- Nausea, vomiting, emotional lability, hyperesthesias, dark urine
- No rash (differentiates from Lyme disease)
- Splenomegaly and hepatomegaly on exam
- ~25% of adult B. microti infections are subclinical; 50% in children
Lab findings:
- Hemolytic anemia (most patients)
- Thrombocytopenia
- Normal or low WBC (leukopenia)
- Elevated LDH, bilirubin (indirect), aminotransferases
- Hemoglobinuria in severe cases
Severe disease (asplenic, elderly >50 yrs, immunocompromised, HIV, transplant, malignancy):
-
Hypotension, high persistent non-periodic fever (40-41°C)
-
Severe hemolytic anemia, hemoglobinuria, jaundice
-
Acute renal failure
-
Non-cardiogenic pulmonary edema / ARDS (up to 20% of severe cases)
-
DIC, heart failure, hepatic necrosis
-
Multiorgan failure and coma in fatal cases
-
B. divergens in Europe: nearly all in splenectomized patients, ~one-third fatality rate
-
Mortality in hospitalized patients: 6-9%; up to 21% in immunocompromised
-
Goldman-Cecil Medicine, p. 3450; Rosen's Emergency Medicine, p. 2702; Murray & Nadel Respiratory Medicine, p. 1354
Diagnosis
1. Blood Smear (Giemsa-stained, thick and thin)
- Intraerythrocytic ring forms resembling P. falciparum early trophozoites
- Key distinguishing features from malaria:
- No hemozoin (malarial pigment)
- No schizonts or gametocytes
- Parasites can be extracellular (extraerythrocytic merozoites free in plasma)
- Multiple parasites per RBC common
- Tetrad/"Maltese cross" form - pathognomonic but rare in B. microti, more common with B. duncani
Fig. 8.53 from Robbins Pathology - Erythrocytes infected with Babesia, showing ring forms and the classic Maltese cross tetrad:
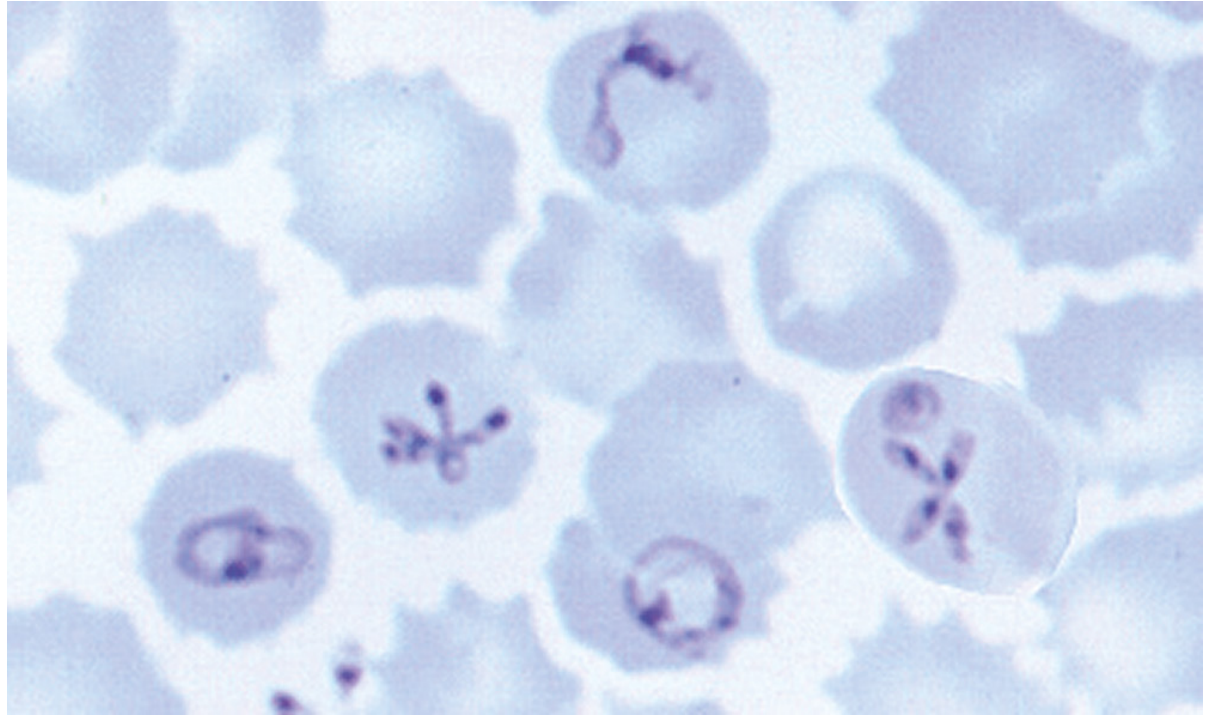
Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 8.53 - Note the characteristic Maltese cross (tetrad) forms within RBCs alongside ring forms.
Fig. 324-1 from Goldman-Cecil Medicine - B. microti blood smear showing ring forms and extraerythrocytic parasite clusters (arrows):
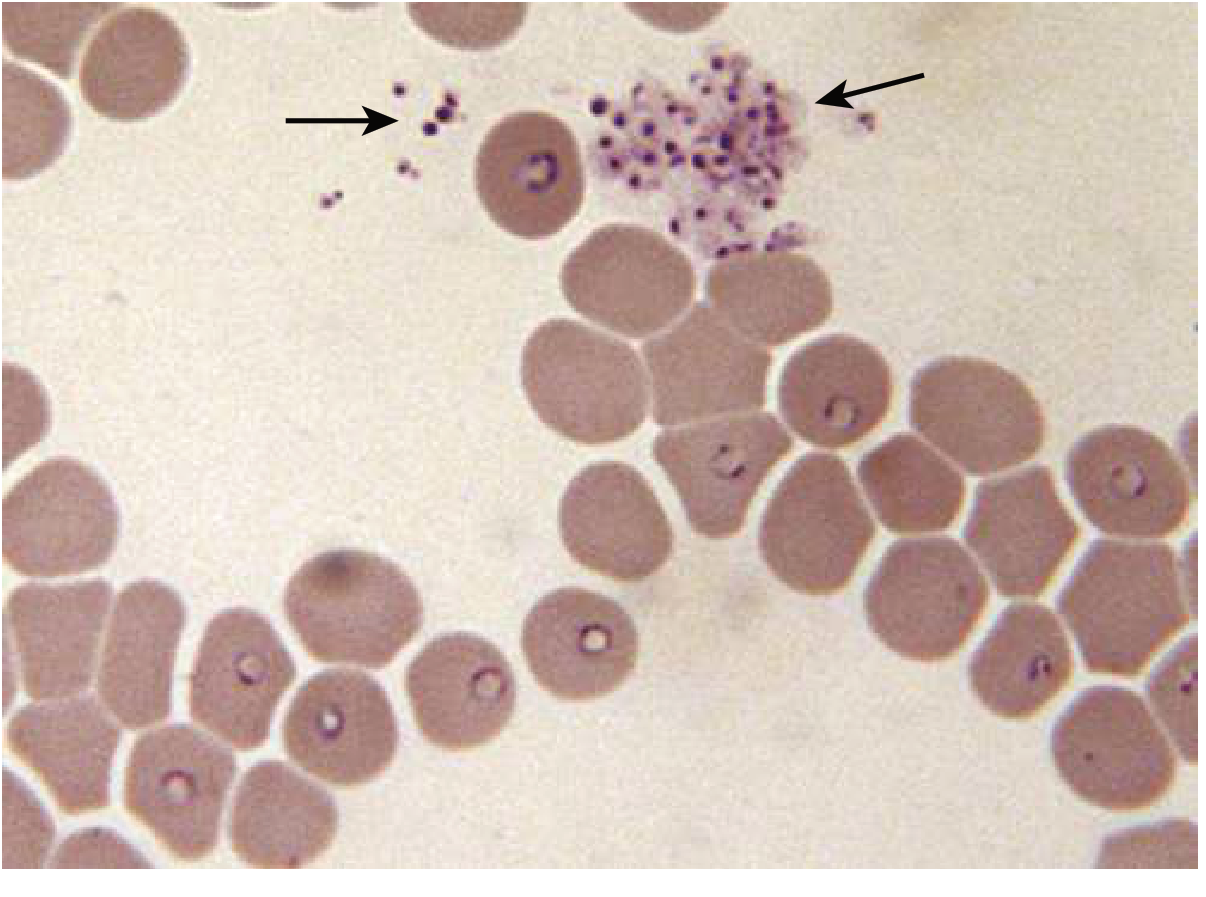
Goldman-Cecil Medicine, Fig. 32-1 - B. microti human infection (Nantucket Island). Predominance of ring forms with cluster of extraerythrocytic parasites (arrows) free in plasma.
2. PCR
- Most sensitive, especially in early infection before antibody response
- Useful for blood donor screening
3. Serology (Indirect Immunofluorescence / IFA)
- IFA titer typically rises to ≥1:1024 within first few weeks
- IgM-IFA sensitive and specific in acute disease
- ELISA and IFA sensitivity rises significantly after 5 days of illness
- High seroprevalence in endemic areas limits usefulness for population screening
- Not useful for B. divergens (fulminant course, too rapid)
4. Animal inoculation
-
Blood injected into hamster/gerbil; parasitemia at 1-4 weeks confirms diagnosis (rarely used clinically)
-
Rosen's Emergency Medicine, p. 2702; Murray & Nadel Respiratory Medicine, p. 1354
Treatment
Mild to Moderate Disease (Immunocompetent, Ambulatory)
| Regimen | Dosing |
|---|---|
| Preferred: Atovaquone + Azithromycin | Atovaquone 750 mg PO q12h (with fatty meal) + Azithromycin 500 mg PO day 1, then 250 mg/day for 7-10 days |
| Alternative: Clindamycin + Quinine | Clindamycin 600 mg PO q8h + Quinine 650 mg PO q8h for 7-10 days (more side effects) |
Severe Disease (Hospitalized)
| Regimen | Dosing |
|---|---|
| Preferred: Atovaquone + Azithromycin | Atovaquone 750 mg PO q12h + Azithromycin 500 mg IV q24h until improvement, then oral step-down |
| Alternative: Clindamycin + Quinine | Clindamycin 600 mg IV q6h + Quinine 650 mg PO q8h until improvement, then oral step-down |
Highly Immunocompromised
- Treat for at least 6 consecutive weeks, including 2 final weeks with no detectable parasitemia on smear
- Azithromycin dose should be 500-1000 mg/day
- Relapsing disease: consider experimental regimens (doxycycline, proguanil, pentamidine, or TMP-SMX) under expert guidance
Exchange Transfusion
- Indicated for severe cases with high parasitemia (>10%), severe hemolysis, or organ compromise
- Rapidly reduces parasite load
Non-splenectomized immunocompetent patients
-
Many recover without specific therapy, but prolonged fatigue is common; treatment is still recommended
-
Goldman-Cecil Medicine, p. 3451 (Table 324-1); Rosen's Emergency Medicine, p. 2702; Murray & Nadel Respiratory Medicine, p. 1354
Key Distinguishing Points: Babesiosis vs. Malaria
| Feature | Babesiosis | Malaria |
|---|---|---|
| Hemozoin pigment | Absent | Present |
| Schizonts | Absent | Present |
| Gametocytes | Absent | Present |
| Maltese cross/tetrad | Present (rare) | Absent |
| Extracellular parasites | Common | Absent |
| RBC enlargement | Absent | Present with P. vivax/ovale |
| Periodicity of fever | Non-periodic | Periodic (tertian/quartan) |
Prevention
- Tick avoidance (protective clothing, permethrin-treated gear, DEET repellent)
- Tick checks after outdoor exposure in endemic areas
- Blood donor screening with B. microti-specific tests in endemic regions (now implemented in the USA)
- Asplenic/immunocompromised patients should be counseled about tick exposure risk
Sources:
- Goldman-Cecil Medicine (International Ed.), pp. 3445-3455
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 373-374
- Rosen's Emergency Medicine, pp. 2701-2702
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1354
Create a quick reference PDF on tick-borne coinfections (Lyme disease, anaplasmosis, babesiosis)
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/tick-coinfections && ls /home/daytona/workspace…
This is a shared conversation. Sign in to Orris to start your own chat.