Tell me only classification of pulmonary hypertension full details for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have excellent, comprehensive data from Harrison's 22e, Braunwald's Heart Disease, and Murray & Nadel's Respiratory Medicine. Let me compile the full MD exam answer.
Classification of Pulmonary Hypertension - MD Exam Answer (10 Marks)
Definition
Pulmonary hypertension (PH) is defined by a mean pulmonary artery pressure (mPAP) >20 mm Hg measured by invasive right heart catheterization (RHC) at rest in the supine position. This threshold was revised downward from the traditional 25 mm Hg at the 6th World Symposium on Pulmonary Hypertension (WSPH, 2018), based on normative data showing a median mPAP of 14.0 ± 3.1 mm Hg in healthy subjects.
- Harrison's Principles of Internal Medicine 22E, 2025
- Braunwald's Heart Disease, 11E
I. HEMODYNAMIC CLASSIFICATION (Pathophysiologic Basis)
The first step in classifying PH is determining its hemodynamic profile using RHC parameters. This distinguishes the anatomical origin of the elevated pressure.
| Category | mPAP | PAWP | PVR | Clinical Groups |
|---|---|---|---|---|
| Pre-capillary PH | >20 mm Hg | ≤15 mm Hg | ≥3 WU | PAH (Group 1), Lung disease (Group 3), CTEPH (Group 4), Miscellaneous (Group 5) |
| Isolated post-capillary PH (IpcPH) | >20 mm Hg | >15 mm Hg | <3 WU | Left heart disease (Group 2) |
| Combined pre- and post-capillary PH (CpcPH) | >20 mm Hg | >15 mm Hg | ≥3 WU | Left heart disease (Group 2) - advanced, with secondary pulmonary arterial remodeling |
PAWP = pulmonary artery wedge pressure; PVR = pulmonary vascular resistance; WU = Wood units
Key point: PAH is exclusively pre-capillary. CpcPH indicates a post-capillary process (e.g. left heart disease) has caused secondary pulmonary arterial remodeling, raising PVR.
II. CLINICAL CLASSIFICATION: 5-GROUP WHO/WSPH SYSTEM (6th WSPH, 2018/2022)
The WHO clinical classification assigns patients to one of five groups based on their underlying etiology, pathophysiology, and hemodynamic profile. This framework guides treatment decisions.
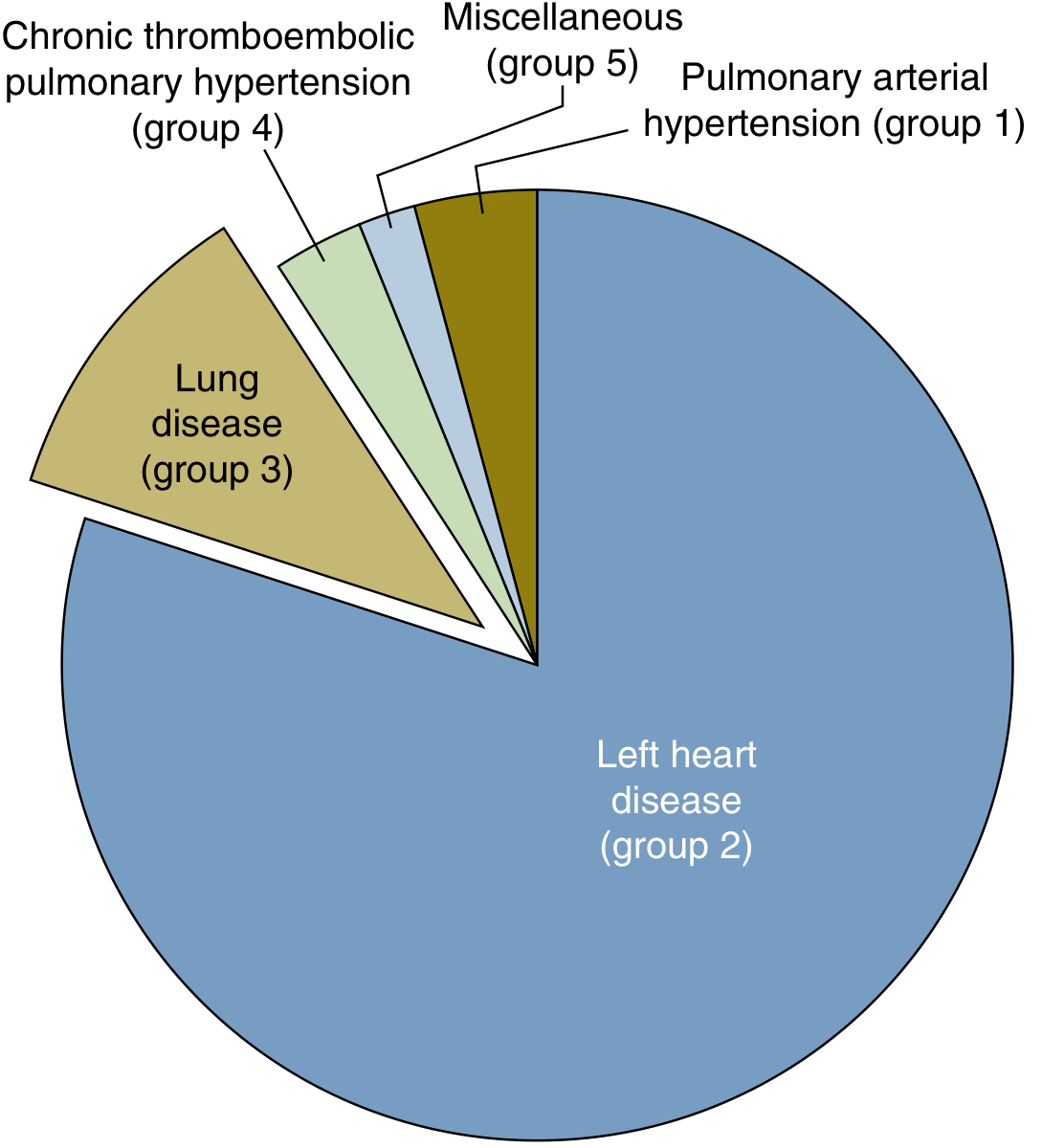
Figure: Relative prevalence of PH groups in the community. Left heart disease (Group 2) is by far the most common cause. - Murray & Nadel's Textbook of Respiratory Medicine
GROUP 1 - Pulmonary Arterial Hypertension (PAH)
Hemodynamics: Pre-capillary; mPAP >20 mm Hg, PAWP ≤15 mm Hg, PVR ≥2-3 WU
Pathology: Marked pulmonary arterial precapillary remodeling - intimal fibrosis, medial hypertrophy, pulmonary arteriolar occlusion, and characteristic plexiform lesions.
Subgroups:
| 1.1 | Idiopathic PAH (IPAH) | Most common form; diagnosis of exclusion; progressive right heart failure; ~3:1 female predominance |
|---|---|---|
| 1.1.1 | Non-responders at vasoreactivity testing | Majority; require targeted PAH therapies |
| 1.1.2 | Acute responders at vasoreactivity testing | ~10%; respond to high-dose calcium channel blockers |
| 1.2 | Heritable PAH | BMPR2 mutation (most common, ~70% heritable cases); younger age, more severe hemodynamics; ~2.3% annual conversion rate in carriers |
| 1.3 | Drug- and toxin-induced PAH | Anorexigens (aminorex, fenfluramine, benfluorex) - definite risk; dasatinib (TKI) - definite risk; bosutinib - possible; leflunomide, sofosbuvir, interferon-α/β - possible risk |
| 1.4 | PAH associated with: | |
| 1.4.1 | Connective tissue disease | Systemic sclerosis most common |
| 1.4.2 | HIV infection | HIV-PAH; pathophysiology unknown |
| 1.4.3 | Portal hypertension (portopulmonary) | |
| 1.4.4 | Congenital heart disease | Includes Eisenmenger syndrome; subclassified into: (a) Eisenmenger syndrome, (b) systemic-to-pulmonary shunts, (c) coincidental small defects, (d) postoperative/closed defects |
| 1.4.5 | Schistosomiasis | Most common worldwide cause of PAH |
| 1.5 | PAH long-term responders to calcium channel blockers | New subgroup in 2018; stable patients on CCBs |
| 1.6 | PAH with overt features of venous/capillary (PVOD/PCH) involvement | Pulmonary veno-occlusive disease / Pulmonary capillary hemangiomatosis |
| 1.7 | Persistent PH of the newborn (PPHN) |
GROUP 2 - PH Due to Left Heart Disease
Hemodynamics: Post-capillary (IpcPH or CpcPH); PAWP >15 mm Hg
Most common cause of PH overall (>60% of all PH cases in community studies).
Virtually any left-sided structural or functional abnormality can cause post-capillary PH. When the post-capillary process induces secondary pulmonary arterial remodeling, PVR rises and CpcPH results.
| 2.1 | Heart failure with preserved ejection fraction (HFpEF) | Most common subtype |
|---|---|---|
| 2.2 | Heart failure with reduced ejection fraction (HFrEF) | EF ≤40% |
| 2.2a | Heart failure with mildly reduced ejection fraction | EF 41-49% |
| 2.3 | Valvular heart disease | Mitral stenosis/regurgitation, aortic stenosis |
| 2.4 | Congenital/acquired cardiovascular conditions leading to post-capillary PH | Stiff left atrial syndrome, obstructive hypertrophic cardiomyopathy |
GROUP 3 - PH Due to Lung Diseases and/or Hypoxia
Hemodynamics: Pre-capillary; driven by hypoxic pulmonary vasoconstriction and structural lung changes
Second most common cause of PH in the community.
| 3.1 | Obstructive lung disease / emphysema | COPD most common |
|---|---|---|
| 3.2 | Restrictive lung disease | Interstitial lung disease (ILD/IPF) |
| 3.3 | Lung disease with mixed restrictive/obstructive pattern | |
| 3.4 | Hypoventilation syndromes | Obesity hypoventilation, obstructive sleep apnea |
| 3.5 | Hypoxia without lung disease | High altitude |
| 3.6 | Developmental lung disorders |
GROUP 4 - PH Due to Pulmonary Artery Obstructions (CTEPH)
Hemodynamics: Pre-capillary; obstruction of large and medium pulmonary arteries
Key entity: Chronic Thromboembolic Pulmonary Hypertension (CTEPH) - results from organized fibrotic thrombi that fail to resolve after pulmonary embolism, causing fixed mechanical obstruction.
Important: CTEPH is potentially curable by pulmonary endarterectomy (PEA) in most patients.
| 4.1 | Chronic thromboembolic PH (CTEPH) | Most important; surgical PEA is curative in ~70% |
|---|---|---|
| 4.2 | Other pulmonary artery obstructions | |
| Sarcomas (angiosarcoma, high/intermediate grade) | ||
| Other malignant tumors (renal, uterine, germ cell) | ||
| Non-malignant tumors (uterine leiomyoma) | ||
| Arteritis without CTD | ||
| Congenital pulmonary artery stenoses | ||
| Parasites: hydatidosis |
GROUP 5 - PH with Unclear and/or Multifactorial Mechanisms
Hemodynamics: Variable; mechanisms include inflammation, direct vascular invasion, and others.
| 5.1 | Hematological disorders | Chronic hemolytic anemia (sickle cell disease, thalassemia), chronic myeloproliferative disorders |
|---|---|---|
| 5.2 | Systemic and metabolic disorders | Pulmonary Langerhans cell histiocytosis, sarcoidosis, neurofibromatosis type 1, Gaucher disease, glycogen storage diseases |
| 5.3 | Metabolic disorders | Glycogen storage disease |
| 5.4 | Chronic renal failure | With or without hemodialysis |
| 5.5 | Pulmonary tumor thrombotic microangiopathy | |
| 5.6 | Fibrosing mediastinitis |
III. FUNCTIONAL CLASSIFICATION (WHO/NYHA)
Although not a separate etiologic classification, the WHO Functional Classification (modified from NYHA) grades severity:
| Class I | No limitation; ordinary activity does not cause PH symptoms |
|---|---|
| Class II | Slight limitation; comfortable at rest; ordinary activity causes symptoms |
| Class III | Marked limitation; comfortable at rest; less than ordinary activity causes symptoms |
| Class IV | Inability to carry on any activity; symptoms at rest; signs of right heart failure |
IV. HISTORICAL CONTEXT - Paul Wood's Original Classification (1950s)
The first systematic PH classification by British cardiologist Paul Wood described six types:
- Passive (due to pulmonary venous hypertension)
- Hyperkinetic (due to increased pulmonary flow)
- Obstructive (precapillary, thrombotic)
- Obliterative (intrinsic vascular remodeling)
- Vasoconstrictive (reactive, e.g. hypoxic)
- Polygenic/Multifactorial
The modern WHO 5-group classification directly evolved from this framework, integrating hemodynamic data with clinical context.
Summary Table
| Group | Name | Hemodynamics | Key Example |
|---|---|---|---|
| 1 | PAH | Pre-capillary | Idiopathic PAH, Eisenmenger |
| 2 | Left heart disease | Post-capillary | HFpEF, mitral stenosis |
| 3 | Lung disease/Hypoxia | Pre-capillary | COPD, IPF, OSA |
| 4 | Pulmonary artery obstruction | Pre-capillary | CTEPH (curable!) |
| 5 | Multifactorial/Unclear | Variable | Sarcoidosis, sickle cell |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - Table 294-1
- Braunwald's Heart Disease, 11th Ed. - Table 88.1 & 88.2
- Murray & Nadel's Textbook of Respiratory Medicine - Table 83.2 (6th WSPH)
- Simonneau G, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019;53(1):1801913
This is a shared conversation. Sign in to Orris to start your own chat.