Axilla
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Here is the complete anatomy of the axilla:
The Axilla
The axilla (armpit) is an irregularly shaped pyramidal space that serves as the gateway between the neck and the upper limb. All major structures passing into and out of the upper limb transit through it.
- Gray's Anatomy for Students, p. 841
Boundaries
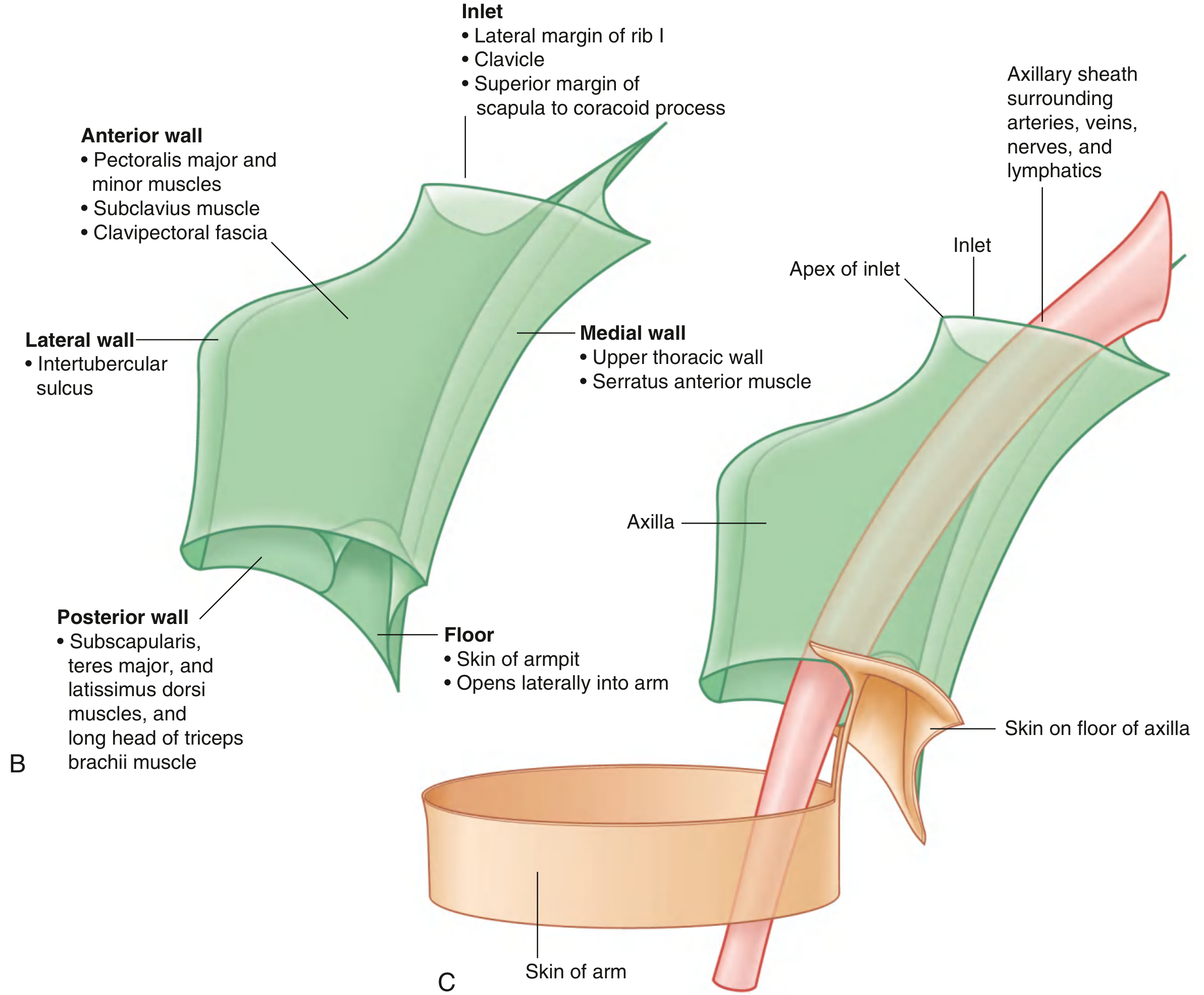
The axilla has four walls, an inlet (apex), and a floor (base).
Axillary Inlet (Apex)
The inlet is triangular, oriented in the horizontal plane, with its apex directed laterally. Its margins are entirely bony:
- Medial - lateral border of rib I
- Anterior - posterior surface of clavicle
- Posterior - superior border of scapula to coracoid process
- Apex - medial aspect of coracoid process
At the inlet, from anterior to posterior: axillary vein > axillary artery > trunks of the brachial plexus.
Walls
| Wall | Structures |
|---|---|
| Anterior | Pectoralis major, pectoralis minor, subclavius, clavipectoral fascia |
| Posterior | Subscapularis, teres major, latissimus dorsi, long head of triceps brachii |
| Medial | Upper thoracic wall (ribs 1-4 + intercostals), serratus anterior |
| Lateral | Intertubercular sulcus of humerus |
Floor (Base)
Formed by the skin of the armpit; it opens laterally into the arm.
Contents of the Axilla
1. Axillary Artery
The subclavian artery becomes the axillary artery at the lateral margin of rib I and becomes the brachial artery at the lower border of teres major. The pectoralis minor crosses it anteriorly and divides it into three parts:
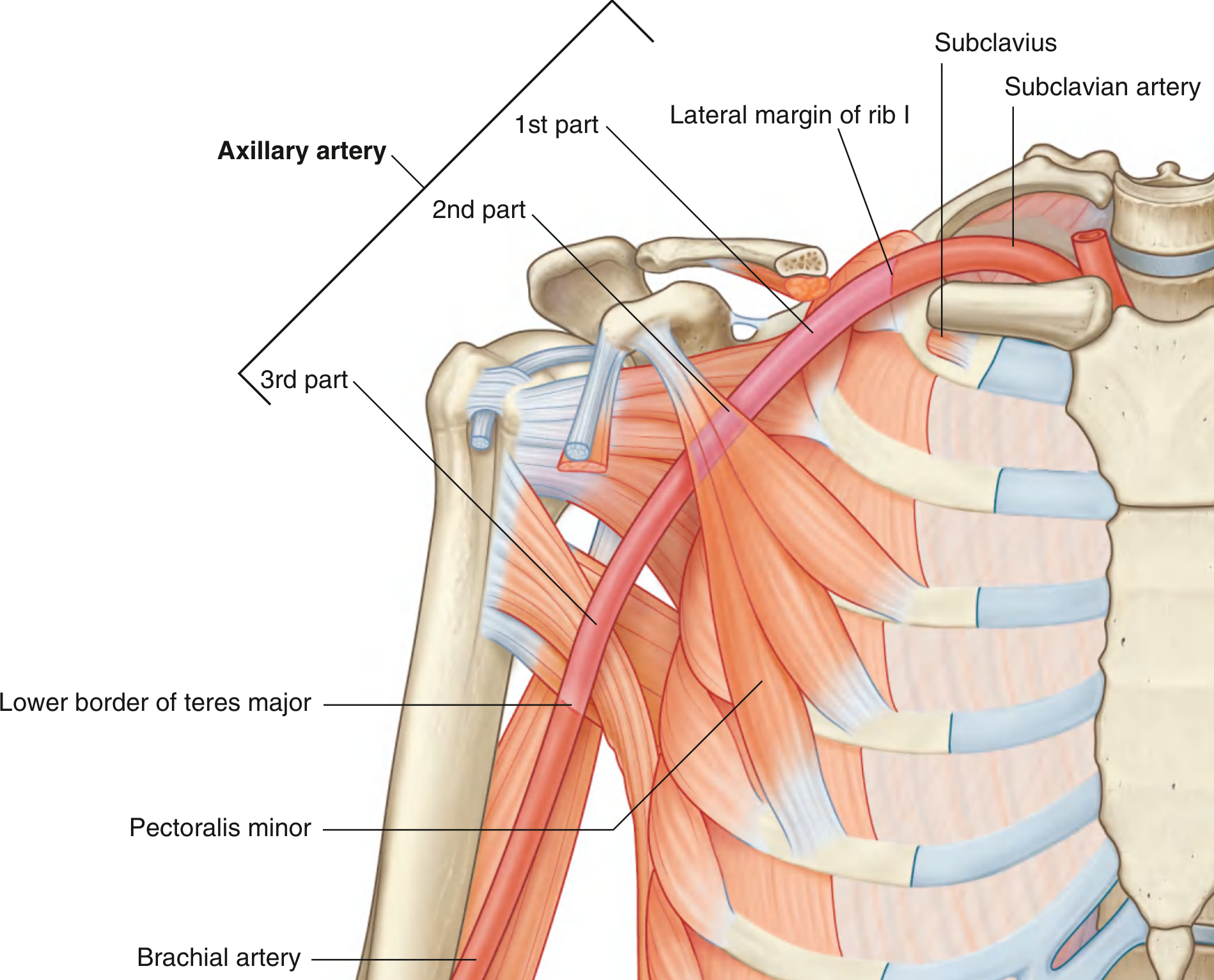
Mnemonic: "1 branch, 2 branches, 3 branches" (one per part)
| Part | Relation to Pec. Minor | Branches |
|---|---|---|
| 1st | Proximal (medial) to pec. minor | Superior thoracic artery (1) |
| 2nd | Posterior to pec. minor | Thoraco-acromial + Lateral thoracic arteries (2) |
| 3rd | Distal (lateral) to pec. minor | Subscapular + Anterior + Posterior circumflex humeral arteries (3) |
2. Axillary Vein
Formed by the union of the brachial veins and the basilic vein at the lower margin of teres major. It lies anteromedial to the axillary artery and becomes the subclavian vein as it crosses the lateral border of rib I. The cephalic vein drains into the axillary vein from the deltopectoral groove.
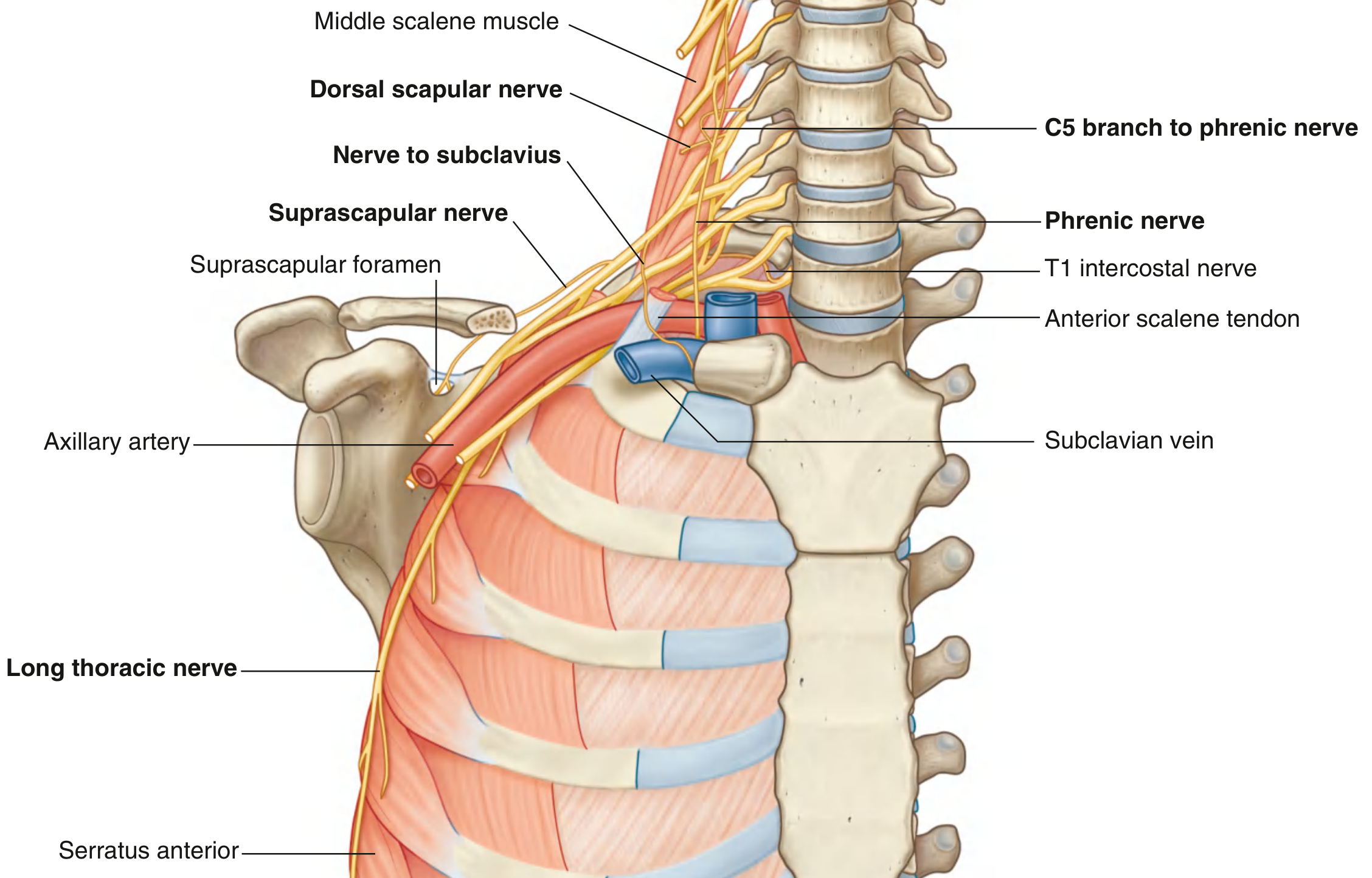
3. Brachial Plexus (Cords and Branches)
The brachial plexus (roots C5-T1) enters the axilla through the inlet and surrounds the axillary artery as three cords named by their relation to the 2nd part of the axillary artery:
Branches from the cords:
Lateral cord (C5-C7):
- Lateral pectoral nerve - pectoralis major
- Musculocutaneous nerve - pierces coracobrachialis; supplies flexors of arm (biceps, brachialis, coracobrachialis)
- Lateral root of median nerve
Medial cord (C8-T1):
- Medial pectoral nerve - pectoralis major and minor
- Medial cutaneous nerve of arm
- Medial cutaneous nerve of forearm
- Ulnar nerve
- Medial root of median nerve
The musculocutaneous nerve + lateral root + median nerve + medial root + ulnar nerve form a characteristic "M" over the 3rd part of the axillary artery - a useful landmark to identify components of the plexus in surgery.
Posterior cord (C5-T1):
- Superior subscapular nerve - subscapularis
- Thoracodorsal nerve - latissimus dorsi
- Inferior subscapular nerve - subscapularis and teres major
- Axillary nerve - exits via quadrangular space; supplies deltoid and teres minor
- Radial nerve - exits via triangular interval; supplies all posterior compartment muscles of arm and forearm
Other direct branches of the plexus in the axilla:
- Long thoracic nerve (C5-C7) - serratus anterior (runs on the medial wall)
- Dorsal scapular nerve (C5) - rhomboids and levator scapulae
4. Muscles Traversing the Axilla
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Biceps brachii (short head) | Coracoid process | Radial tuberosity | Musculocutaneous (C5,C6) | Flexes forearm, supinates, accessory arm flexor |
| Biceps brachii (long head) | Supraglenoid tubercle | Radial tuberosity | Musculocutaneous (C5,C6) | As above; also prevents superior translation of humeral head |
| Coracobrachialis | Coracoid process | Mid-medial humerus | Musculocutaneous (C5,C6,C7) | Arm flexion and adduction |
The musculocutaneous nerve pierces coracobrachialis within the axilla to enter the arm.
5. Axillary Lymph Nodes (20-30 nodes, 5 groups)
The axillary nodes receive drainage from: the entire upper limb, chest wall, upper back and shoulder, lower neck, upper anterolateral abdominal wall, and ~75% of the mammary gland.
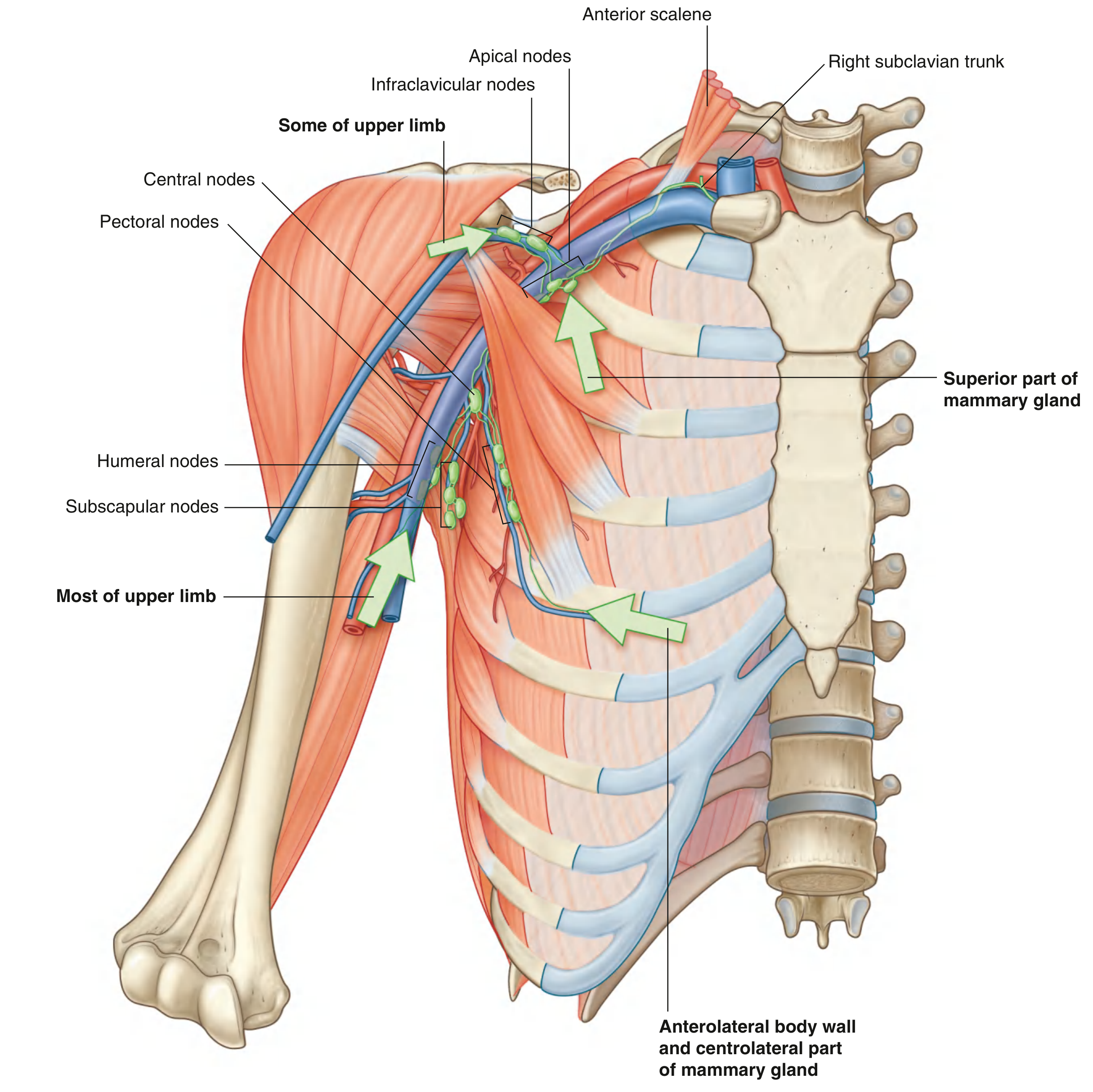
| Group | Location | Drains |
|---|---|---|
| Humeral (lateral) | Posteromedial to axillary vein | Most of upper limb |
| Pectoral (anterior) | Along inferior border of pectoralis minor / lateral thoracic vessels | Chest wall, abdominal wall, breast |
| Subscapular (posterior) | Posterior axillary wall with subscapular vessels | Back, shoulder, neck |
| Central | Embedded in axillary fat | Receives from humeral, subscapular, and pectoral groups |
| Apical | Most superior; along axillary vein near apex | All other groups + superior breast |
Efferent vessels from the apical nodes form the subclavian trunk, which drains into the right lymphatic duct (right side) or thoracic duct (left side).
Clinically, axillary node levels in breast surgery are classified relative to pectoralis minor: Level I = lateral, Level II = posterior, Level III = medial (apical). Sentinel node biopsy targets the first draining node and has reduced the need for full axillary clearance.
Key Clinical Points
- Axillary artery injury from rib I fracture (rapid deceleration) or anterior shoulder dislocation can compromise upper limb blood supply; however, anastomoses around the scapula usually prevent complete ischemia.
- Brachial plexus injuries - Severe trauma to rib I damages trunks; glenohumeral dislocation injures cords and divisions; cervical cord injuries or traction affect roots.
- Long thoracic nerve damage - Causes winging of the scapula (serratus anterior paralysis). The nerve is at risk during axillary surgery.
- Axillary nerve damage - From surgical neck of humerus fractures or shoulder dislocation; causes loss of deltoid function (abduction defect) and loss of skin sensation over the shoulder badge area.
- Thoracodorsal nerve - At risk during axillary dissection; its damage paralyses latissimus dorsi.
Source: Gray's Anatomy for Students, pp. 841-868
This is a shared conversation. Sign in to Orris to start your own chat.